A 2026 medRxiv preprint found that older adults with mild-cognitive-impairment-level MoCA-J scores showed distinct resting facial action-unit patterns: AU10 upper lip raiser, AU23 lip tightener, and AU28 lip suck differed after correction in 45 analyzable participants.1 The result supports facial-expression screening research, but it does not show that a face video can diagnose MCI or dementia.
Research Highlights
- Analyzed sample was 45: after 5 video exclusions, the study compared 31 MCI-level older adults with 14 healthy controls.1
- MoCA-J separated groups: mean MoCA-J was 23.7 in the MCI-level group and 27.1 in controls, while GDS depression scores did not differ, p = 0.74.1
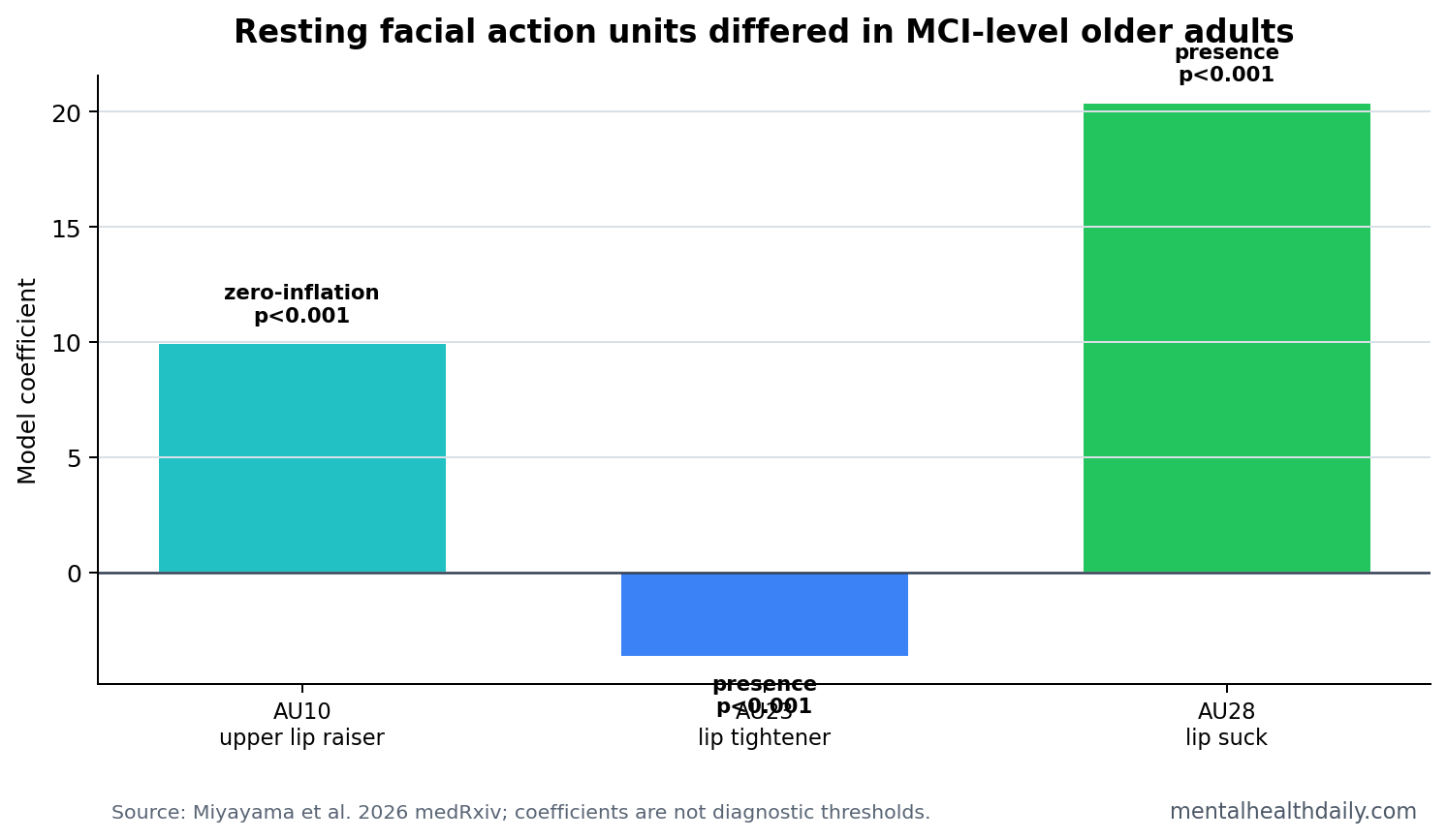
- Upper-lip signal survived correction: AU10 upper lip raiser zero-inflation differed by group, beta_zero = 9.93, SE 2.75, p < 0.001.1
- Lip-presence signals also survived: AU23 lip tightener, beta = −3.62, and AU28 lip suck, beta = 20.36, both differed by group at p < 0.001.1
- Diagnosis was not tested: participants were grouped by cognitive-screening scores in 2026, not by biomarker-confirmed Alzheimer’s disease or clinical dementia diagnosis.
Mild cognitive impairment (MCI) means measurable cognitive difficulty that is greater than expected for age but does not yet meet dementia-level functional impairment. MCI is clinically heterogeneous: some people progress to dementia, some remain stable, and some revert to normal-range testing.
Facial Action Units are standardized facial-muscle movement codes. AU10 refers to upper lip raiser, AU23 to lip tightener, and AU28 to lip suck. Miyayama et al. used OpenFace 2.0 to extract these features from resting facial video rather than from posed emotional expressions.
31 MCI-Level and 14 Control Participants Were Analyzable
The researchers recruited 50 older adults and excluded 5 because OpenFace could not accurately detect eyebrow positions, usually because of eyeglasses or bangs. That left 31 participants in the MCI-level group and 14 healthy controls.1
Group assignment came from the Japanese Montreal Cognitive Assessment (MoCA-J), a brief cognitive screening test. A score of 25 or lower was treated as MCI-level performance. The MCI-level group averaged 23.7, SD 1.4, while controls averaged 27.1, SD 1.3. Depression symptoms were unlikely to explain the facial-expression differences because GDS scores did not differ, p = 0.74.
Screening-status caveat: the paper’s “MCI level” phrase is important. These participants had cognitive screening scores consistent with MCI-level performance. They were not necessarily diagnosed with MCI after a full clinical workup.
AU10 Upper Lip Raiser Was More Often at Zero Intensity
The facial analysis had 2 parts. The first modeled action-unit intensity from 0 to 5, converted to a 0-to-1 scale. Because many frames had exactly zero intensity for a given facial movement, the researchers used zero-inflated beta regression, which can model both intensity and the chance of a zero value.
Across 17 intensity action units, the beta component was not significant for any action unit. The zero-inflation component was significant for AU10 upper lip raiser, beta_zero = 9.93, SE 2.75, p < 0.001, and AU17 chin raiser, beta_zero = 5.39, p = 0.048. Only AU10 survived multiple-comparison correction.1
AU23 Lip Tightener and AU28 Lip Suck Differed in Presence Models
The second analysis modeled whether each facial action unit was present or absent. Among 18 presence variables, 2 survived correction: AU23 lip tightener and AU28 lip suck. AU23 had beta = −3.62, SE 1.03, p < 0.001. AU28 had beta = 20.36, SE 1.42, p < 0.001.1
These are not intuitive bedside signs. A clinician should not look for “lip suck” and infer cognitive impairment. The value is more technical: automated facial analysis may detect subtle resting muscle-use patterns that humans would not score reliably during ordinary observation.
- AU10: upper lip raiser intensity was more likely to be exactly zero in the MCI-level group.
- AU23: lip tightener presence differed between groups after correction.
- AU28: lip suck presence differed between groups after correction.
Facial Screening Could Reduce Burden, but False Signals Are the Risk
The appeal of facial-expression screening is obvious. Video is cheap, passive, and easier to repeat than MRI, lumbar puncture, or even formal cognitive testing. In theory, a low-burden screen could flag people who should receive MoCA testing, blood biomarkers, neurological evaluation, or longitudinal follow-up.
The risk is equally obvious. Facial expression is affected by camera angle, lighting, dental status, medications, Parkinsonism, depression, facial palsy, cultural display rules, fatigue, and ordinary individual differences. Even in this small study, 10% of recruited participants were excluded because automated facial detection struggled with eyewear or hair obstruction.
Implementation standard: a facial-expression tool would need to show calibrated sensitivity and specificity in larger samples, across camera types, ethnic groups, lighting conditions, and clinical diagnoses. It would also need to prove that it adds value beyond age, education, MoCA, depression symptoms, and medical history.
Digital Biomarkers Need Outcome Validation and Group Differences
Adjacent digital-biomarker work has used neutral facial images, speech, typing, gait, and smartphone behavior to look for cognitive decline signals.2 Those approaches are promising because cognition changes behavior in distributed ways. They are also easy to overstate because group differences do not automatically become individual screening tools.
Evidence-strength note: this was a small preprint using MoCA-J grouping, not a diagnosed MCI or dementia outcome. It can identify candidate facial features for larger screening studies. It cannot prove that AU10, AU23, or AU28 detects Alzheimer’s disease, predicts conversion, or should be used outside research.
The most realistic role is a triage layer. Facial-expression markers might eventually combine with brief cognitive tests, speech markers, sleep data, or blood biomarkers to reduce missed early cognitive decline. Alone, the 2026 result is not enough.
Why Resting Faces Are Harder Than Posed Emotion Tasks
Resting facial expression is attractive because it does not require a participant to understand instructions for a complex task, remember a story, or produce a specific emotion on command. That feature helps older adults, multilingual settings, and repeated passive screening. It also makes the signal harder to interpret because the person is not doing one standardized cognitive or emotional action.
In a posed task, a reduced smile or weaker brow movement can be compared with the requested expression. During rest, the model has to infer meaning from ordinary muscle tone, small movements, and how often a facial action appears at all. That is why the 2026 paper’s action-unit-level approach is preferable to a black-box “AI face score” headline: it at least names which movements differed.
Measurement problem: a resting facial marker can reflect cognition, mood, alertness, dental comfort, facial anatomy, medications, or camera conditions. Any clinical version would need quality-control rules and covariate checks before the output could be trusted.
MoCA-Level Grouping Is Useful but Clinically Thin
The MoCA-J threshold gave the study a practical way to divide participants, but a screening score is not a diagnosis. A full MCI workup usually includes clinical history, functional assessment, neuropsychological context, medication review, depression and sleep assessment, and sometimes imaging or fluid biomarkers. MoCA can flag risk; it does not explain why the score is low.
That distinction matters for facial-expression research because a low MoCA score could come from several causes. Hearing problems, low sleep, anxiety during testing, education, vascular disease, early Alzheimer’s biology, Parkinsonian features, or depression can all influence performance. A face-based marker trained only on score groups may learn a mixture of those causes.
- Useful signal: action-unit differences may reveal a low-burden cognitive-risk phenotype.
- Unresolved source: the study cannot say whether the phenotype reflects Alzheimer’s biology, general aging, motor features, or test-performance confounds.
- Needed endpoint: future studies should test clinical MCI diagnosis, longitudinal conversion, and same-day MoCA thresholds together.
For now, the finding should be framed as a candidate screening feature. It is interesting because it is cheap and unobtrusive, not because it is ready to replace cognitive testing.
Bottom line: the 2026 preprint makes resting facial action units worth testing in larger cognitive-aging cohorts, especially if future models report ordinary screening metrics such as sensitivity, specificity, calibration, likelihood ratios, subgroup performance, and false-positive rates.
Validation should also include deliberate failure cases: eyeglasses, facial hair, dentures, facial palsy, Parkinsonian masking, camera angle, low light, and non-Japanese-speaking cohorts. A passive screen that fails quietly under common recording conditions would be risky even if average group differences replicate.
Consent and feedback rules matter too, because facial data are identifiable and hard to anonymize after collection.
Those metrics decide whether passive screening helps real patients.
Questions About Facial Expression and MCI Screening
Can a face video diagnose MCI?
No. This study found action-unit differences between groups defined by MoCA-J score. It did not diagnose MCI clinically or test dementia conversion.
Why were lip-region action units important?
AU10, AU23, and AU28 were the facial features that survived correction in this dataset. The paper does not prove that these movements are specific to cognitive impairment; they are candidate digital markers.
What would make the approach useful?
A useful screening tool would need larger validation samples, diagnostic outcomes, clear error rates, and tests showing that facial features improve detection beyond standard cognitive screening.
References
- Miyayama T, et al. Characteristic resting state facial expressions in older adults with mild cognitive impairment level. medRxiv. 2026. doi:10.64898/2026.04.10.26350581
- Jung H, et al. Facial expression and image-based markers for dementia and cognitive impairment. PubMed
- Baltrusaitis T, et al. OpenFace 2.0: facial behavior analysis toolkit. PubMed
- Nasreddine ZS, et al. The Montreal Cognitive Assessment, MoCA: a brief screening tool for mild cognitive impairment. Journal of the American Geriatrics Society. 2005. PubMed