
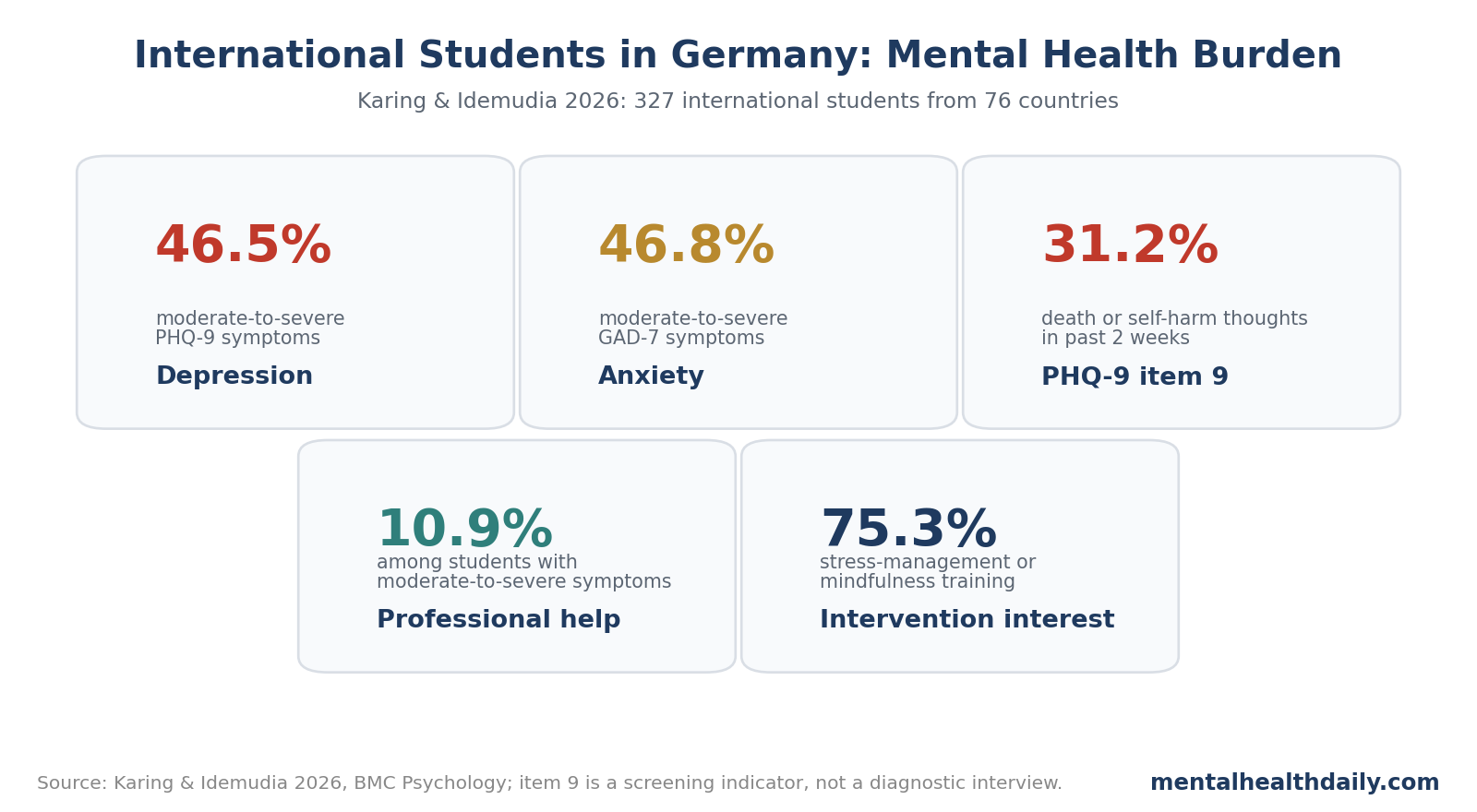
A 2026 survey of 327 international students in Germany found high symptom burden: 46.5% screened positive for moderate-to-severe depression, 46.8% for moderate-to-severe anxiety, and 31.2% endorsed recent death or self-harm thoughts on PHQ-9 item 9. Only 10.9% of students with moderate-to-severe depression and/or anxiety reported professional help.1
Research Highlights
- 327 international students were surveyed: Karing and Idemudia studied students in Germany from 76 countries; 61.5% were female and most were enrolled in degree programs.1
- Depression and anxiety screens were high: 46.5% had moderate-to-severe depressive symptoms and 46.8% had moderate-to-severe anxiety symptoms.1
- PHQ-9 item 9 was elevated: 31.2% endorsed death or self-harm thoughts in the prior 2 weeks, which is a screening signal rather than a diagnostic suicide interview.1
- Treatment use was low: only 10.9% of students with moderate-to-severe depression and/or anxiety received professional help such as psychotherapy.1
- Mindfulness was the strongest protective correlate: higher mindfulness was associated with lower depression, anxiety, and acculturative stress in the regression models.1
Acculturative stress means the psychological strain of adapting to a different cultural, academic, linguistic, and social environment. For international students, that strain can combine with financial pressure, visa uncertainty, isolation, and unfamiliar health systems.
Nearly Half Screened Positive for Depression or Anxiety
Karing and Idemudia used the Patient Health Questionnaire-9 (PHQ-9) for depression and the Generalized Anxiety Disorder-7 (GAD-7) for anxiety. These are symptom screening tools, not structured psychiatric interviews, but they are widely used and easy to interpret in student-health contexts.1
The main prevalence numbers were stark:
- Mean PHQ-9 score: 10.27, consistent with moderate depressive symptoms.
- Moderate-to-severe depression: 46.5%.
- Mean GAD-7 score: 9.39, consistent with mild anxiety symptoms on average.
- Moderate-to-severe anxiety: 46.8%.
- Recent death or self-harm thoughts on PHQ-9 item 9: 31.2%.
The item 9 result needs careful wording. It is not identical to a clinician-confirmed suicidal-ideation diagnosis. PHQ-9 item 9 captures thoughts that the respondent would be better off dead or of hurting themselves in some way. It is a warning signal that should trigger follow-up, not a complete suicide-risk assessment.
The treatment gap was the other major result. Among students with moderate-to-severe depression and/or anxiety, only 10.9% reported professional help. Among the 13% who had been diagnosed with a mental disorder since 2020, only 26.1% received treatments such as psychotherapy.1
The diagnosed subgroup also showed concentrated risk. Depression was the most frequently reported diagnosis, affecting 73.8% of students who reported any mental-disorder diagnosis since 2020, followed by anxiety at 45.2%. Among students diagnosed with depression, 17 endorsed death or self-harm thoughts on PHQ-9 item 9.1
Acculturative Stress Added Risk Beyond Other Predictors
The researchers used hierarchical regressions, which means predictors were entered in blocks. Demographics came first, then psychological factors, then coping strategies, then acculturative stress for the depression and anxiety models.1
The variance pattern is useful because it shows what carried the most explanatory weight:
- Demographics explained only a small share: R² = 0.04-0.10.
- Psychological variables added much more: delta R² = 0.27-0.29.
- Coping strategies added modestly: delta R² = 0.04-0.06.
- Acculturative stress added further variance for depression and anxiety: delta R² = 0.03-0.05.
Acculturative stress remained a significant predictor of depression (beta = 0.252, p < 0.001) and anxiety (beta = 0.208, p < 0.001). Beta is a standardized regression coefficient; here, higher acculturative stress was associated with worse symptoms after accounting for other variables.
That does not prove acculturative stress caused the symptoms. Depressed and anxious students may perceive stress more intensely, and cross-sectional surveys cannot establish temporal order. Still, the association fits the everyday structure of the problem: language barriers, unfamiliar academic expectations, social disconnection, and service navigation are plausible symptom amplifiers.
Mindfulness, Optimism, Self-Efficacy, and Social Support Differed by Outcome
Mindfulness showed the largest standardized protective associations across outcomes:
- Depression: beta = −0.251, p < 0.001.
- Anxiety: beta = −0.219, p < 0.001.
- Acculturative stress: beta = −0.192, p < 0.001.
Mindfulness here should not be read as vague wellness language. In this study, it was measured as a psychological variable: the tendency to pay attention to present experience with awareness rather than automatic judgment.
Other protective variables were more specific:
- Optimism was associated with lower depression and anxiety.
- Self-efficacy was associated with lower anxiety.
- Social support from fellow students was associated with lower depression.
- Social support from friends was associated with lower anxiety.
- Family and institutional support were associated with lower acculturative stress.
That pattern argues against a generic “more support” slogan. Different support sources may solve different student problems. Fellow students can reduce academic and social isolation. Friends may buffer anxiety. Family and institutional support may reduce the strain of navigating a foreign system.
The non-finding for problem-solving is also informative. Problem-solving can be useful when a stressor is controllable, such as scheduling, paperwork, or exam planning. Acculturative stress often includes low-control stressors: homesickness, cultural distance, discrimination, language fatigue, and uncertainty about belonging.
For low-control stressors, acceptance-based coping and mindfulness may fit better than telling students to solve problems they cannot immediately change. That interpretation needs longitudinal testing, but it explains why mindfulness and acceptance signals may have appeared while problem-solving did not clearly protect mental health in this sample.
Service Access Was the Most Actionable Gap
The study's most actionable finding is the mismatch between symptoms and professional help. A university can run mindfulness programs, peer support, and orientation sessions, but a 10.9% help-use rate among students with moderate-to-severe symptoms points to a service-access problem.
Several barriers are plausible:
- Stigma: students may fear judgment from family, peers, or future employers.
- Language: counseling in a second or third language can feel too effortful or emotionally limited.
- System navigation: students may not understand insurance, referrals, waitlists, or where to begin.
- Cultural fit: a service can exist but still feel mismatched to the student's explanatory model, family expectations, or religious background.
- Time and money: work, visa pressure, and academic load can push care-seeking down the list.
The survey also found that only about 40% of students agreed that university facilities provided adequate support. That is not a diagnostic metric, but it is operationally useful: students may be showing up in the country, entering degree programs, and carrying high symptom burden while perceiving the support system as hard to use.
That perception should be measured routinely. Universities often know how many counseling appointments were booked, but not how many international students never entered the system because they could not find culturally comfortable help in the first place.
A basic intake map would separate students who know services exist from students who trust those services enough to use them.
The research did not test an intervention, so it cannot say which service design works best. It does point toward a practical care model: early screening, culturally competent referral, multilingual navigation, peer contact, and stepped care so students with mild symptoms are not handled the same way as students endorsing self-harm thoughts.
Item 9 Requires Follow-Up, Not Panic
PHQ-9 item 9 is intentionally broad. A positive response can mean passive death wishes, self-harm thoughts, or more active suicidal ideation. It should trigger follow-up questions about intent, plan, means, past attempts, protective factors, substance use, and acute stressors.
The 31.2% rate was higher than domestic-student comparison figures cited by the researchers and close to other international-student samples. That convergence points to a broader international-student risk signal, though self-selection bias may inflate the estimate.1
For universities, the safer interpretation is operational: if a third of respondents endorse item 9 in a voluntary international-student survey, the system needs a clear path from screening to same-day risk triage when needed.
That path should include:
- screening language that distinguishes passive death thoughts from active suicidal intent;
- rapid clinical follow-up for any concerning response;
- clear crisis contacts in the student's preferred language when possible;
- coordination with academic and housing supports when immediate stressors are driving risk.
Limitations of the International Student Survey
- Convenience and snowball sampling. Students interested in mental health may have been more likely to participate.
- Cross-sectional data. The study cannot prove whether acculturative stress caused symptoms or whether symptoms changed perceived stress.
- Self-report measures. PHQ-9 and GAD-7 screen symptoms but do not replace diagnostic interviews.
- Germany-specific context. Results may differ in countries with different tuition systems, health insurance, visa policies, and counseling access.
- Broad international category. Students from 76 countries were grouped into a single international-student frame, which can hide country-specific and culture-specific patterns.
Questions About International Student Mental Health in Germany
How common were depression and anxiety symptoms?
Moderate-to-severe depression was reported by 46.5% of students, and moderate-to-severe anxiety by 46.8%.
Does 31.2% mean one-third were actively suicidal?
No. PHQ-9 item 9 is a screening item for death or self-harm thoughts. It requires follow-up to determine intent, plan, and risk level.
Which protective factor was strongest?
Mindfulness had the largest standardized protective associations across depression, anxiety, and acculturative stress.
What should universities prioritize first?
Better access pathways: screening, culturally competent referral, multilingual navigation, peer support, and rapid triage for self-harm responses.
References
- Karing C, Idemudia E. Acculturative stress and mental health among international students in Germany. BMC Psychology. 2026;14:605. doi:10.1186/s40359-026-04576-5
- Berry JW. Immigration, acculturation, and adaptation. Applied Psychology. 1997;46:5-34. doi:10.1111/j.1464-0597.1997.tb01087.x
- Lazarus RS, Folkman S. Stress, appraisal, and coping. Springer. 1984. archive.org
- Joiner TE. Why people die by suicide. Harvard University Press. 2005. publisher page
- Funder DC, Ozer DJ. Evaluating effect size in psychological research. Advances in Methods and Practices in Psychological Science. 2019;2:156-168. doi:10.1177/2515245919847202