
A 12-week text-message intervention for people with schizophrenia spectrum disorders improved diabetes self-management confidence and patient activation, but it did not yet move weight, HbA1c, physical activity, or psychiatric symptoms. SMART looked feasible and psychologically useful in this uncontrolled pilot; cardiometabolic outcomes need a full-scale randomized trial with longer follow-up.1
Research Highlights
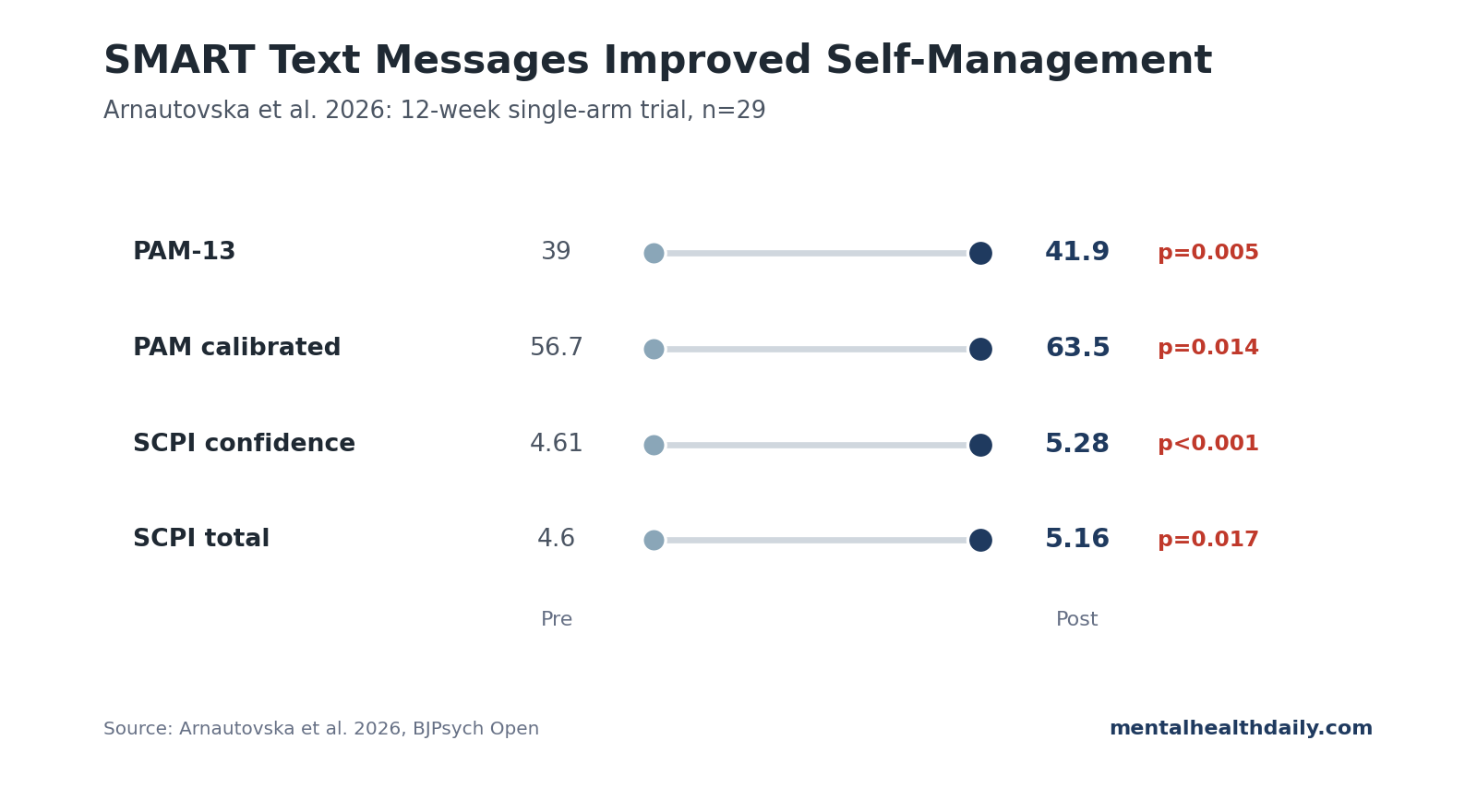
- SMART was tested for 12 weeks: Arnautovska et al. enrolled 29 outpatients with schizophrenia or schizoaffective disorder, type 2 diabetes (T2D) or prediabetes risk, and high cardiometabolic burden.1
- Patient activation improved: PAM-13 total scores increased from 39.0 to 41.9 (difference 2.87, p = 0.005), and calibrated PAM-13 scores increased from 56.7 to 63.5 (p = 0.014).1
- Diabetes confidence improved: SCPI confidence rose from 4.61 to 5.28 (p < 0.001), and SCPI total increased from 4.60 to 5.16 (p = 0.017).1
- Objective metabolic markers did not shift: Weight, BMI, waist circumference, HbA1c, fasting glucose, triglycerides, HDL, LDL, and blood pressure changes were non-significant.1
- Engagement was unusually strong: Recruitment was 67.4%, attrition was 6.9%, and text-message response adherence averaged 93% across 12 weeks.1
SMART stands for Schizophrenia and diabetes Mobile-Assisted Remote Trainer. The intervention is meant for a high-risk care gap: people with schizophrenia spectrum disorders (SSDs) have elevated rates of T2D, metabolic syndrome, obesity, smoking, sedentary behavior, and antipsychotic-associated weight gain.2,4
SMART Enrolled 29 Schizophrenia-Spectrum Outpatients
The trial used a single-arm pre-post design. That means everyone received SMART, and outcomes before the 12-week intervention were compared with outcomes afterward. There was no placebo group, usual-care comparison, or blinded endpoint assessment, so the study can show feasibility and preliminary signal, not causal efficacy.
The sample was clinically relevant rather than pristine:
- Diagnosis: all 29 participants had schizophrenia or schizoaffective disorder.
- Metabolic burden: 58.6% had T2D, 6.9% had prediabetes, and 58.6% met metabolic syndrome criteria.
- Body weight: median BMI was 37 kg/m2, with median weight 104.6 kg.
- Smoking: 44.8% were current smokers, with median 15 cigarettes per day among smokers.
- Cognition: 31.0% had mild cognitive impairment and 20.7% had moderate cognitive impairment on the Montreal Cognitive Assessment.
That cognitive profile changes the design problem. A digital health intervention for schizophrenia cannot assume app fluency, high reading level, stable motivation, or easy executive functioning. SMART used SMS text messages rather than a smartphone app, included check-in calls, and used messages written around an 11- to 12-year reading age.1
SMART Used Texting to Lower the Self-Management Burden
The intervention went beyond motivational texting. Participants selected modules across practical metabolic-health domains, and the text stream then delivered prompts, check-ins, and self-management support around those chosen areas.
The module menu shows what SMART was actually trying to move:
- Weight management: basic weight-control behaviors rather than intensive obesity treatment.
- Physical activity: prompts to increase movement in a population with very low baseline activity.
- Nutrition: diabetes-relevant diet support without assuming high health literacy.
- Stress coping: a relevant target because stress can disrupt eating, smoking, sleep, and medication routines.
- Glucose monitoring: self-management support for people with T2D or prediabetes risk.
- Smoking and vaping: a high-yield target because 44.8% of the sample were current smokers.
A lifestyle handout asks the patient to convert advice into routines. SMART tried to convert the advice into repeated, low-friction prompts that reached people where they already were: on basic mobile phones, without requiring a new app ecosystem.
Patient Activation Improved More Than Metabolic Biomarkers
The primary outcome was the Patient Activation Measure (PAM-13), a scale designed to capture knowledge, skill, and confidence for managing health. This is not a blood test; it is a behavioral mechanism measure. In SMART, it improved significantly after 12 weeks.
- PAM-13 total: 38.98 to 41.85; difference 2.87 (95% CI 0.95-4.80), p = 0.005.
- PAM-13 calibrated: 56.67 to 63.45; difference 6.78 (95% CI 1.48-12.08), p = 0.014.
- Health literacy: HLQ active health management rose from 2.81 to 3.04; p = 0.032.
- Recovery: RAS-DS “Doing things I value” rose from 17.97 to 19.14; p = 0.022.
The diabetes self-management pattern was similar. Overall Skills, Confidence and Preparedness Index (SCPI) scores improved from 4.60 to 5.16, and confidence rose from 4.61 to 5.28. Skills and preparedness improved numerically but did not reach statistical significance.1
SMART improved the “I can manage this” layer before it improved the physiology layer. That is a behavioral signal, but it is not the same thing as proving lower diabetes risk.
HbA1c, Weight, and Physical Activity Did Not Significantly Change
The objective cardiometabolic endpoints were mostly flat over 12 weeks:
- Weight changed from 107.48 kg to 106.42 kg, p = 0.064.
- BMI changed from 36.70 to 36.36, p = 0.083.
- HbA1c moved from 6.10% to 6.13%, p = 0.746.
- Fasting glucose, waist circumference, blood pressure, LDL, HDL, and total cholesterol were non-significant.1
Physical activity and diet self-reports did not clearly move either:
- Moderate-to-vigorous physical activity rose from 0.71 to 0.92 minutes per day, p = 0.114.
- Mediterranean Diet Adherence Screener score rose from 4.54 to 5.15, p = 0.111.
12 weeks of SMS support may be enough to improve confidence and activation, while slow cardiometabolic markers may need longer or more intensive intervention in a small uncontrolled sample with severe baseline metabolic risk.
The weight result is worth reading carefully. A mean loss of about 1.1 kg looked directionally favorable, but p = 0.064 did not meet the usual threshold for statistical significance. That is a reasonable signal to carry into a larger trial, not a result to market as weight loss.
HbA1c is even more constrained by timing. Because HbA1c reflects average glycemia over roughly 2 to 3 months, a 12-week feasibility trial has little room to show durable diabetes improvement unless the behavioral change is large and early. SMART mainly showed the upstream behavioral-readiness signal.
Text-Message Engagement Was the Strongest Implementation Signal
Digital interventions often fail because people stop using them. SMART did not show that pattern. Recruitment was 67.4% (29 of 43), attrition was 6.9% (2 of 29), and average response adherence to text messages was 93%. Engagement stayed at or above 90% across all 12 weeks except week 4, which dropped to 82%, likely because of Christmas timing or phone-credit problems.1
Participants rated usability strongly: median System Usability Scale score was 75, interpreted as grade B usability, and acceptability scores reached the top of the 5-point Acceptability of Intervention Measure range.
The delivery design probably mattered:
- SMS instead of app: no app download, account setup, or constant internet access required.
- Low reading demand: messages were written for accessible comprehension.
- Human support: check-in calls occurred at weeks 4 and 8 and after 3-day non-response periods.
- Personalized module choice: participants prioritized weight management, physical activity, nutrition, stress coping, glucose monitoring, and smoking/vaping modules.
Schizophrenia Diabetes Care Needs More Than Generic Lifestyle Advice
Schizophrenia metabolic care sits inside core psychiatric care. T2D prevalence is substantially elevated in psychiatric disorders, and antipsychotic medication, sedentary behavior, smoking, diet, sleep disruption, poverty, and care fragmentation all contribute.2,4
The Lancet Psychiatry physical-health work has repeatedly argued that metabolic prevention needs to be embedded into mental health care rather than treated as someone else’s problem.4,5 SMART fits that direction because it targets self-management inside a schizophrenia-tailored format.
A text-message system that improves activation is promising; it is not yet a proven diabetes-prevention program. The next test needs randomization, longer follow-up, objective activity measurement, and enough power to detect changes in HbA1c, weight, waist circumference, smoking, diet, and medication adherence.
That next test should also separate 2 questions that get blurred in small feasibility work:
- Can people use it? SMART’s recruitment, attrition, adherence, and usability data say yes, at least in this outpatient sample.
- Does it improve health? The metabolic-outcome data do not answer that yet.
Those are different thresholds. A clinic might reasonably pilot SMS support as a low-burden engagement tool while still recognizing that diabetes prevention requires harder evidence.
Limitations of the SMART Feasibility Trial
- No control group. Without usual care or placebo comparison, regression to the mean, staff contact, expectancy, and repeated testing can all contribute to improvement.
- Small sample. With 29 participants, the study was underpowered for cardiometabolic endpoints and subgroup analyses.
- Short duration. The 12-week window may be too brief to move HbA1c, weight, or lipid markers, especially in people with established T2D and obesity.
- Outpatient-only sample. Results may not generalize to inpatient units, first-episode psychosis, treatment-resistant schizophrenia, non-English speakers, or lower-resource settings without adaptation.
Questions About SMART for Schizophrenia and Diabetes
Did SMART lower blood sugar?
No clear HbA1c effect appeared in this 12-week trial. HbA1c changed from 6.10% to 6.13%, which was non-significant.
What did SMART actually improve?
It improved patient activation, diabetes self-management confidence, overall diabetes self-management, active health management, and one mental-health recovery domain. Those are behavioral mechanism measures, not hard metabolic outcomes.
Why use text messages instead of an app?
SMS lowers the access burden because it works without a smartphone app, data plan, account setup, or high digital literacy. That format fits people with cognitive impairment, low income, or inconsistent internet access.
Should clinics use SMART now?
Not as a proven metabolic treatment. The evidence supports feasibility and preliminary promise. A powered randomized controlled trial is needed before treating SMART as clinically effective.
References
- Arnautovska U, Ritchie G, Korman N, et al. SMART: preliminary efficacy, feasibility and acceptability of a theory-informed digital intervention for metabolic health in people with schizophrenia and related disorders. BJPsych Open. 2026. doi:10.1192/bjo.2026.11032
- Lindekilde N, Scheuer SH, Rutters F, et al. Prevalence of type 2 diabetes in psychiatric disorders: an umbrella review with meta-analysis of 245 observational studies from 32 systematic reviews. Diabetologia. 2022;65:440-456. doi:10.1007/s00125-021-05609-x
- Han L, Doran T, Holt RIG, et al. Impact of severe mental illness on healthcare use and health outcomes for people with type 2 diabetes: a longitudinal observational study in England. British Journal of General Practice. 2021;71:e565-e573. doi:10.3399/bjgp.2020.0884
- Firth J, Siddiqi N, Koyanagi A, et al. The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness. Lancet Psychiatry. 2019;6:675-712. doi:10.1016/s2215-0366(19)30393-1
- Teasdale SB, Machaczek KK, Marx W, et al. Implementing lifestyle interventions in mental health care: third report of the Lancet Psychiatry Physical Health Commission. Lancet Psychiatry. 2025;12:700-722. doi:10.1016/s2215-0366(25)00170-1
- Arnautovska U, Trott M, Vitangcol KJ, et al. Efficacy of user self-led and human-supported digital health interventions for people with schizophrenia: a systematic review and meta-analysis. Schizophrenia Bulletin. 2024;51:1402-1416. doi:10.1093/schbul/sbae143
- Romain AJ, Bernard P, Akrass Z, et al. Motivational theory-based interventions on health of people with severe mental illness: a systematic review and meta-analysis. Schizophrenia Research. 2020;222:31-41. doi:10.1016/j.schres.2020.05.049