A 5-year PPMI cohort analysis found that lower serum uric acid independently predicted incident depression in prodromal Parkinson’s disease (HR = 0.776; 95% CI 0.619-0.974; P = 0.029).1 The signal sits beside a lower-p-value non-motor symptom predictor: higher MDS-UPDRS Part I scores also predicted depression (HR = 1.177; 95% CI 1.093-1.267; P < 0.001).
Research Highlights
- 460 people entered baseline analysis: Liang et al. selected prodromal Parkinson’s disease participants from the PPMI database after excluding incomplete cases.
- 61 people completed the risk analysis: the 5-year depression model used participants without baseline depression who had sufficient annual follow-up.
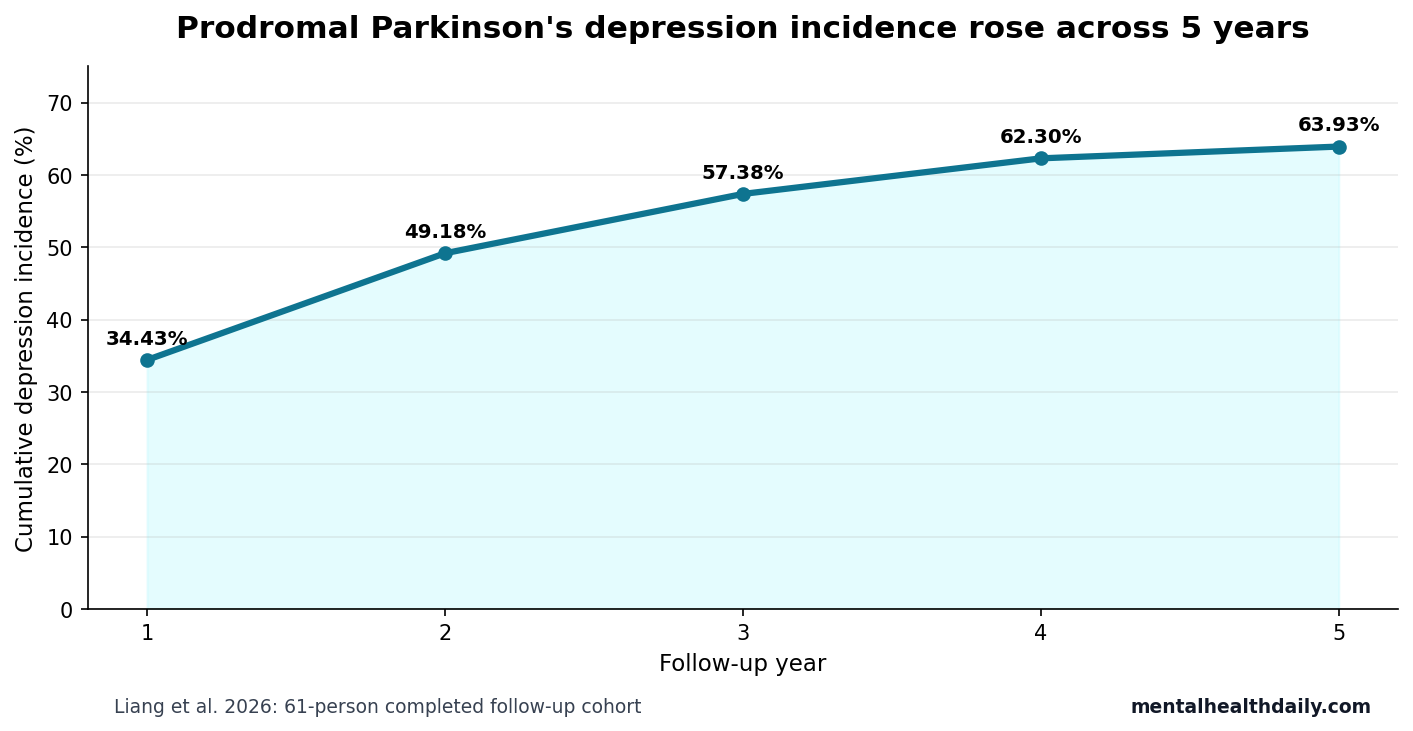
- Depression accumulated quickly: cumulative incidence rose from 34.43% at year 1 to 63.93% at year 5.
- Non-motor burden predicted depression: each higher MDS-UPDRS Part I score unit was associated with higher incident depression risk (HR = 1.177; P < 0.001).
- Lower uric acid added biomarker signal: serum UA independently predicted incident depression (HR = 0.776; P = 0.029), with lower values linked to higher risk.
Prodromal Parkinson’s disease means a risk state in which early non-motor or biomarker features suggest Parkinson’s biology before formal motor diagnostic criteria are met. Depression is one of the non-motor symptoms that can appear before the classic tremor, rigidity, and bradykinesia picture.
Uric acid is the end product of purine metabolism and acts as an antioxidant in blood. In Parkinson’s disease research, lower urate has long been studied as a possible marker of vulnerability, but raising urate has not become an established disease-modifying treatment.
Baseline Depression Was 18.9% in Prodromal Parkinson’s Disease
Liang et al. began with 631 possible PPMI participants, retained 460 people for baseline analysis, and separated those with depression (n = 87) from those without depression (n = 373). Baseline depression prevalence was 18.9%.
The baseline comparison looked like a non-motor Parkinson’s disease profile rather than a simple urate story. The depression group differed on sex (P = 0.027), MDS-UPDRS Part I score (P < 0.001), total MDS-UPDRS score (P < 0.001), apathy (P < 0.001), anxiety score (P < 0.001), and autonomic score (P = 0.019).
MDS-UPDRS Part I is the non-motor experiences of daily living section of the Movement Disorder Society Unified Parkinson’s Disease Rating Scale. It covers mental, behavioral, sleep, sensory, autonomic, and other non-motor problems that often shape Parkinson’s quality of life.
Several baseline non-signals matter for calibration. Age, body mass index, education, levodopa-equivalent daily dose, motor-score components, Hoehn-Yahr stage, MoCA cognitive score, excessive daytime sleepiness, cerebrospinal-fluid amyloid, cerebrospinal-fluid tau markers, serum neurofilament light, and serum uric acid were not significantly different between the depressed and non-depressed baseline groups. The baseline table therefore did not show a clean cross-sectional urate separation.
MoCA means Montreal Cognitive Assessment, a 30-point cognitive screening test. Neurofilament light is a blood or cerebrospinal-fluid marker of nerve-cell injury. In this dataset, those markers were not the headline depression separators at baseline; the sharper baseline pattern was psychiatric and autonomic symptom clustering inside the prodromal Parkinson’s phenotype.
Depression Incidence Rose to 63.93% by Year 5
The longitudinal depression model used 61 prodromal participants who had no baseline depression and completed adequate annual follow-up. Among them, 39 developed depressive symptoms during the 5-year observation period.
Cumulative incidence increased at every annual check: 34.43% at year 1, 49.18% at year 2, 57.38% at year 3, 62.30% at year 4, and 63.93% at year 5. The steep early rise is clinically important because depression risk did not wait for a late Parkinson’s disease stage.
Lower Serum Uric Acid Survived Multivariable Modeling
The authors used univariate Cox regression, LASSO feature selection, and multivariable Cox regression. Cox regression estimates time-to-event risk; here, the event was incident depression during follow-up. LASSO is a feature-selection method that shrinks weaker predictors and reduces overfitting risk in smaller datasets.
After age and sex adjustment, 2 variables survived the multivariable model. Higher MDS-UPDRS Part I predicted higher depression risk (HR = 1.177; 95% CI 1.093-1.267; P < 0.001). Lower serum uric acid also predicted depression (HR = 0.776; 95% CI 0.619-0.974; P = 0.029).
The modeling sequence is the reason the result is more interesting than a one-table association. Univariable Cox analysis initially flagged age, sex, education, MDS-UPDRS Part I, anxiety score, apathy, and serum uric acid at the P ≤ 0.1 screening stage. LASSO then retained a smaller set of candidate predictors before the final Cox model. The small-sample problem remains, but serum uric acid survived beyond the unfiltered baseline comparisons.
- Non-motor symptom signal: higher Part I scores likely captured broader mental, autonomic, sleep, and sensory burden.
- Biomarker signal: lower UA added information after model selection and covariate adjustment.
- Direction: the HR below 1 means higher UA was associated with lower depression risk, so lower UA marks higher risk.
Hazard ratio scale: an HR of 0.776 for serum UA means higher uric acid was associated with lower time-to-depression risk in the fitted model. It should not be read as a 22.4% risk reduction for any individual patient without knowing the unit scaling, distribution, and clinical context. The practical read is directional: lower serum UA remained a risk-marker signal after the model accounted for age and sex.
Urate Biology Fits Oxidative Stress but Does Not Prove Treatment
Uric acid can scavenge reactive oxygen and nitrogen species, and Parkinson’s disease has long been linked to oxidative stress, mitochondrial stress, and dopaminergic neuron vulnerability.2 That makes the urate finding biologically plausible.
The mechanistic chain is still indirect. Lower serum UA could reflect antioxidant capacity, diet, kidney function, medication exposure, genetics, metabolic status, inflammation, or broader health. The study could not fully adjust for every factor that influences uric acid levels.
Clinical boundary: the finding supports risk-marker follow-up, not attempts to raise uric acid. High uric acid can contribute to gout, kidney stones, and cardiometabolic risk. Prior Parkinson’s urate work supports biomarker interest, not a simple supplementation rule.
Urate has a complicated Parkinson’s disease history. Epidemiologic and biomarker studies have often treated higher urate as a possible protective marker, while intervention logic has been much less settled.
- Risk-marker use: low serum UA can help identify prodromal Parkinson’s disease patients who may need closer depression surveillance.
- Treatment boundary: changing serum UA is a different claim and was not tested in this cohort.
- Safety boundary: high uric acid can carry gout, kidney-stone, and cardiometabolic tradeoffs.
A marker can be useful for stratifying risk even when changing the marker is not useful, safe, or proven. For this cohort, the defensible application is closer mood follow-up when low serum UA appears alongside heavier non-motor burden.
Depression in prodromal Parkinson’s disease is also not reducible to oxidation chemistry. Serotonergic signaling, dopaminergic circuitry, sleep disturbance, autonomic dysfunction, anxiety, apathy, and inflammatory biology can all converge on mood symptoms before classic motor Parkinson’s disease is diagnosed. Uric acid may sit inside that network as an antioxidant and purine-metabolism marker, not as a single upstream cause.
Attrition Is the Main Calibration Problem
The largest limitation is the fall from 460 baseline participants to 61 people in the final 5-year Cox analysis. Attrition can distort longitudinal estimates if people who remain in follow-up differ meaningfully from those lost or excluded.
Liang et al. ran a baseline comparison between the included 61-person group and the 399-person lost-to-follow-up or inadequate-follow-up group. Most baseline indicators did not significantly differ, but depression-related status necessarily differed because baseline depression cases were excluded from the incident-risk model.
Evidence-strength note: this is an observational cohort analysis with a small completed follow-up sample. It supports serum UA as a risk marker worth replication, not a causal claim that low uric acid produces depression or that urate-raising therapy prevents it.
The sensitivity comparison is reassuring but incomplete. The included 61-person group and the excluded 399-person group did not significantly differ on age, sex, body mass index, education, motor scores, cognitive score, or several biofluid measures. Still, absence of significant baseline differences is not the same as proof that attrition was harmless. A 61-person risk set can miss moderate confounding and can make estimates sensitive to a small number of events.
The clean next replication would keep the same basic question but widen the denominator: larger prodromal Parkinson’s cohorts, repeated serum UA measurements, kidney-function and medication covariates, and depression outcomes measured with instruments beyond one MDS-UPDRS item. Until then, the study is best read as a focused PPMI warning signal: low serum UA plus non-motor symptom burden may identify a subgroup that deserves closer mood follow-up.
One practical implication follows even before replication: a low-cost blood chemistry marker should not outrank symptom review. The stronger model signal came from MDS-UPDRS Part I, and the baseline profile tied depression to apathy, anxiety, and autonomic symptoms. Serum UA is most useful when it sharpens that clinical pattern, not when it distracts from direct mood assessment.
Questions About Uric Acid and Prodromal Parkinson’s Depression
Was uric acid the strongest predictor?
No. Higher MDS-UPDRS Part I had a stronger statistical signal (P < 0.001). Serum UA added an independent biomarker association (P = 0.029).
Does lower uric acid diagnose depression risk?
No. It is a risk marker from one cohort analysis. Depression screening still depends on symptoms, clinical history, and follow-up assessment.
Should Parkinson’s patients raise uric acid?
No treatment conclusion follows from this study. Uric acid has potential harms at high levels, and the result needs replication before clinical action.
References
- Liang K, Ouyang Y, Li B, et al. Lower serum uric acid levels as a risk factor for depression in prodromal Parkinson’s disease: a cohort study. Open Life Sciences. 2026;21(1):20251309. https://doi.org/10.1515/biol-2025-1309
- Paganoni S, Schwarzschild MA. Urate as a marker of risk and progression of neurodegenerative disease. Neurotherapeutics. 2017;14:148-153. https://pubmed.ncbi.nlm.nih.gov/28063035/
- PubMed search: prodromal depression Parkinson disease systematic review meta-analysis. https://pubmed.ncbi.nlm.nih.gov/?term=prodromal+depression+Parkinson+disease+systematic+review+meta-analysis
- PubMed search: PPMI prodromal Parkinson biomarkers depression urate. https://pubmed.ncbi.nlm.nih.gov/?term=PPMI+prodromal+Parkinson+biomarkers+depression+urate