A 2026 Spanish Rett Syndrome Behavior Questionnaire validation preprint found strong test-retest reliability across 51 caregivers, including an intraclass correlation coefficient of 0.907 and a 31-person short-interval subset with Pearson r2 = 0.8663.1 The result supports Spanish-language research access, but it is linguistic validation rather than proof that the scale diagnoses Rett syndrome or measures treatment response alone.
Research Highlights
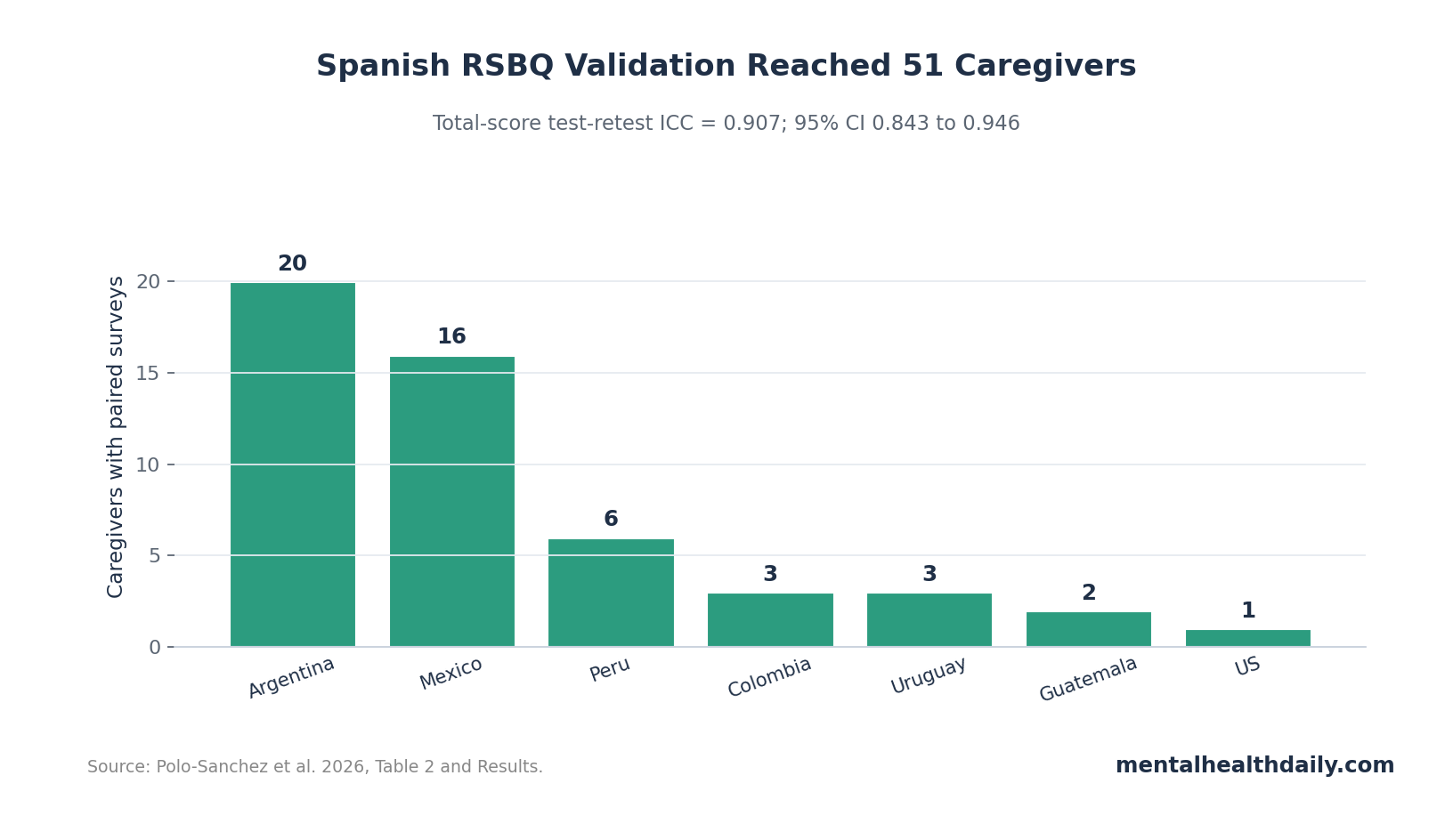
- 51 caregivers completed both surveys: The final test-retest sample included caregivers from Argentina, Mexico, Peru, Colombia, Uruguay, Guatemala, and 1 Spanish-speaking US caregiver.1
- Reliability was strong: Total-score test-retest intraclass correlation was 0.907, with 95% CI 0.843 to 0.946.1
- Short-interval results held: Among 31 caregivers retesting within 7-21 days, 28 of 31 averages fell within 2 standard deviations and Pearson r2 was 0.8663.1
- Translation changes were targeted: 12 of 45 items stayed unchanged, 7 needed critical wording changes, and the rest received minor grammar or word-order edits.1
- Clinical validation remains separate: The RSBQ is a widely used Rett outcome tool, but translation reliability does not by itself prove treatment sensitivity or diagnostic accuracy.2,3
Rett syndrome is a severe neurodevelopmental disorder, most often linked to MECP2 dysfunction, that can involve regression, loss of purposeful hand use, gait impairment, seizures, breathing abnormalities, autistic-like features, and major communication disability. Caregiver-reported outcome measures are questionnaires completed by caregivers to quantify symptoms that patients may not be able to report directly.
The Rett Syndrome Behavior Questionnaire (RSBQ) is one of the main behavioral scales used in Rett research. A Spanish version matters because trials and observational studies can underrepresent families when the validated outcome tools exist mainly in English.
51 Caregivers Passed the Full Test-Retest Workflow
Polo-Sanchez et al. used a two-stage design. Phase I involved 12 guided administrations, where Spanish-speaking caregivers could ask for clarification and identify confusing wording. Phase II used independent online administration of the refined questionnaire, followed by retest at least 7 days later.1
The final analytic sample included 51 caregivers after duplicate removal and quality control. Countries were distributed as follows: Argentina 20, Mexico 16, Peru 6, Colombia 3, Uruguay 3, Guatemala 2, and the United States 1. The sample was mostly female caregivers, 47 of 51.
The sample was not enormous, but it did include a real cross-country Spanish-speaking caregiver pool rather than a single-clinic translation check.
Rare-disease context: a 51-caregiver analytic sample is modest for ordinary psychometrics, but Rett syndrome research often works under recruitment constraints because the condition is rare and many affected children have severe communication and motor impairment. For that reason, the better question is not whether this study provides final validation. It is whether the translation performed consistently enough to justify larger Spanish-language clinical and trial use.
ICC 0.907 Supports Strong Total-Score Reliability
Intraclass correlation coefficient (ICC) measures agreement between repeated measurements. An ICC near 1.0 means repeated scores are highly consistent; an ICC near 0 means repeated scores are mostly noise.
The Spanish RSBQ total-score ICC was 0.907, with 95% CI 0.843 to 0.946.1 That is a strong reliability result for a caregiver questionnaire, especially given the multicountry sample and rare-disease recruitment constraints.
Mean total scores also stayed stable: Test 1 averaged 46.8 ± 17.0, and Test 2 averaged 47.2 ± 17.4, with paired t-test p = 0.6540. That means the group average did not shift meaningfully between administrations.
Total-score stability: stable means alone are not enough, because a group average can stay flat while individual families move around. The ICC and short-interval scatter are therefore more informative than the paired t-test by itself. They show that the same caregivers tended to give similar total scores across administrations, while the group average also stayed stable.
That distinction matters for trial readiness. A behavioral outcome measure has to preserve rank-order information well enough that a real treatment signal is not buried under translation noise. The Spanish RSBQ is not proven treatment-sensitive yet, but the reliability pattern is compatible with using it in studies that also include clinician ratings and global-impression anchors.
Long Retest Delays Were the Main Measurement Caveat
The study originally required retest after at least 7 days, but recruitment reminders and community events created long delays for some responders. The mean response interval was 45.4 days, the median was 11 days, and the standard deviation was 56.5 days. Responses clustered around 7-8 days and 80-100 days.1
Long retest intervals can blur reliability. If a child’s symptoms genuinely change across 80-100 days, lower agreement may reflect real clinical change rather than translation failure.
The researchers handled that by analyzing the 31 caregivers who completed retest within 7-21 days. In that short-interval subset, 28 of 31 Bland-Altman averages fell within 2 standard deviations, and test-retest scores showed Pearson r2 = 0.8663 with p < 0.0001.1
Short-interval subset: this 31-caregiver analysis is the cleaner reliability check because it reduces the chance that true symptom change explains score differences. Rett symptoms can fluctuate with seizures, sleep, illness, medication changes, and caregiving context. A 7-21-day retest window is not perfect, but it is much closer to a measurement-repeat test than a several-month gap.
Translation Edits Preserved the Original Scale Structure
The study did not reinvent the RSBQ. It kept the original 45-question structure and scoring approach, while changing wording where caregivers found the certified translation unclear or culturally awkward. That matters because outcome scales lose comparability if translations quietly change the construct being measured.
The item review showed 12 questions unchanged from the certified medical translation, 7 questions with critical changes, and the rest with minor grammar or word-order revisions.1
Measurement logic: translation should improve comprehension without changing the symptom target. If a hand stereotypy item, breathing item, or mood-behavior item becomes easier to understand but still asks the same question, cross-language data become more credible.
The study’s 2-stage structure was useful for that reason. Guided administration exposed misunderstood wording before the online retest phase, while independent completion tested whether the final wording could work without a researcher explaining each item. That sequence is closer to real-world research use than a translation produced only by back-translation paperwork.
Cross-country wording is the practical problem. A Spanish phrase that works in one country can sound medicalized, vague, or uncommon in another. By drawing caregivers from Argentina, Mexico, Peru, Colombia, Uruguay, Guatemala, and the United States, the study at least tested whether the final wording could survive more than one regional Spanish context.
The remaining caution is that Latin America and Spanish-speaking families are not one homogeneous population. Education, health literacy, trial access, rural vs. urban care, and local clinical language can all affect questionnaire use. A good translation reduces one barrier; it does not erase broader access problems in rare-disease research.
One practical implication is that future trials should add the Spanish questionnaire with measurement monitoring. They should track missingness, completion time, caregiver questions, and whether item-level responses behave similarly across regions. That would show whether the translation remains stable when moved from validation into treatment research.
Spanish RSBQ Expands Trial Access While Clinical Validation Remains Separate
The original RSBQ was developed to refine the behavioral phenotype of Rett syndrome, and modern Rett treatment trials such as trofinetide have reinforced the need for standardized outcomes.2,3 A Spanish translation can make those outcome systems more inclusive.
Evidence-strength note: this was a linguistic validation preprint, not a full psychometric validation across all Spanish-speaking populations. It can support comprehension and short-term retest reliability. It cannot prove sensitivity to treatment change, diagnostic accuracy, minimally important clinical difference, or performance across every dialect and care setting.
Several next steps are still needed:
- Clinical anchoring: compare Spanish RSBQ changes with clinician-rated severity, seizure history, motor function, and caregiver global impression.
- Treatment sensitivity: test whether the scale detects expected changes in interventional trials.
- Dialect robustness: evaluate whether wording performs similarly across more Spanish-speaking regions.
- Caregiver burden: measure whether questionnaire completion remains practical for families managing severe disability.
Until those steps are done, the Spanish RSBQ should be treated as a stronger access tool, not a standalone endpoint that can carry a trial by itself. It can help include Spanish-speaking families in Rett research, but treatment claims still need clinician ratings, biological context, and patient-centered change anchors.
Questions About the Spanish RSBQ
Does this questionnaire diagnose Rett syndrome?
No. The RSBQ is a behavioral assessment tool, not a genetic or diagnostic test. Rett diagnosis still depends on clinical evaluation and, often, MECP2 testing.
Why does Spanish validation matter?
Without validated translated measures, Spanish-speaking families can be excluded from trials or measured with tools that are less reliable. Translation quality directly affects research access.
It also affects interpretation after families are included. If a scale is linguistically unstable, an apparent treatment effect might reflect confusing wording, and a true treatment effect might be missed because caregiver responses are noisy. Reliable translation is part of the measurement infrastructure, not a courtesy add-on.
Is ICC 0.907 enough?
It is a strong reliability signal for repeated total scores. Full clinical validation still needs larger samples, clinical anchors, and treatment-response testing.
References
- Polo-Sanchez M, Lesmes AC, Muni N, Vigneault F, Novak R. Linguistic validation of the Rett Syndrome Behavior Questionnaire Spanish translation: a two-stage caregiver study across Latin America. medRxiv. 2026. doi:10.64898/2026.04.16.26349544
- Mount RH, Charman T, Hastings RP, Reilly S, Cass H. The Rett Syndrome Behaviour Questionnaire: refining the behavioural phenotype of Rett syndrome. Journal of Child Psychology and Psychiatry. 2002;43(8):1099-1110. doi:10.1111/1469-7610.00236
- Neul JL, Percy AK, Benke TA, et al. Trofinetide for the treatment of Rett syndrome: a randomized phase 3 study. Nature Medicine. 2023;29:1468-1475. doi:10.1038/s41591-023-02398-1
- Chahrour M, Zoghbi HY. The story of Rett syndrome: from clinic to neurobiology. Neuron. 2007;56(3):422-437. doi:10.1016/j.neuron.2007.10.001
- Moretti P, Zoghbi HY. MeCP2 dysfunction in Rett syndrome and related disorders. Current Opinion in Genetics & Development. 2006;16(3):276-281. doi:10.1016/j.gde.2006.04.009