A 2026 prospective German aneurysm cohort found risky alcohol use in 4.6% of 954 intracranial aneurysm patients, and that exposure carried 2.00x higher adjusted odds of aneurysm rupture plus 3.26x higher adjusted odds of clinically severe aneurysmal subarachnoid hemorrhage.
Research Highlights
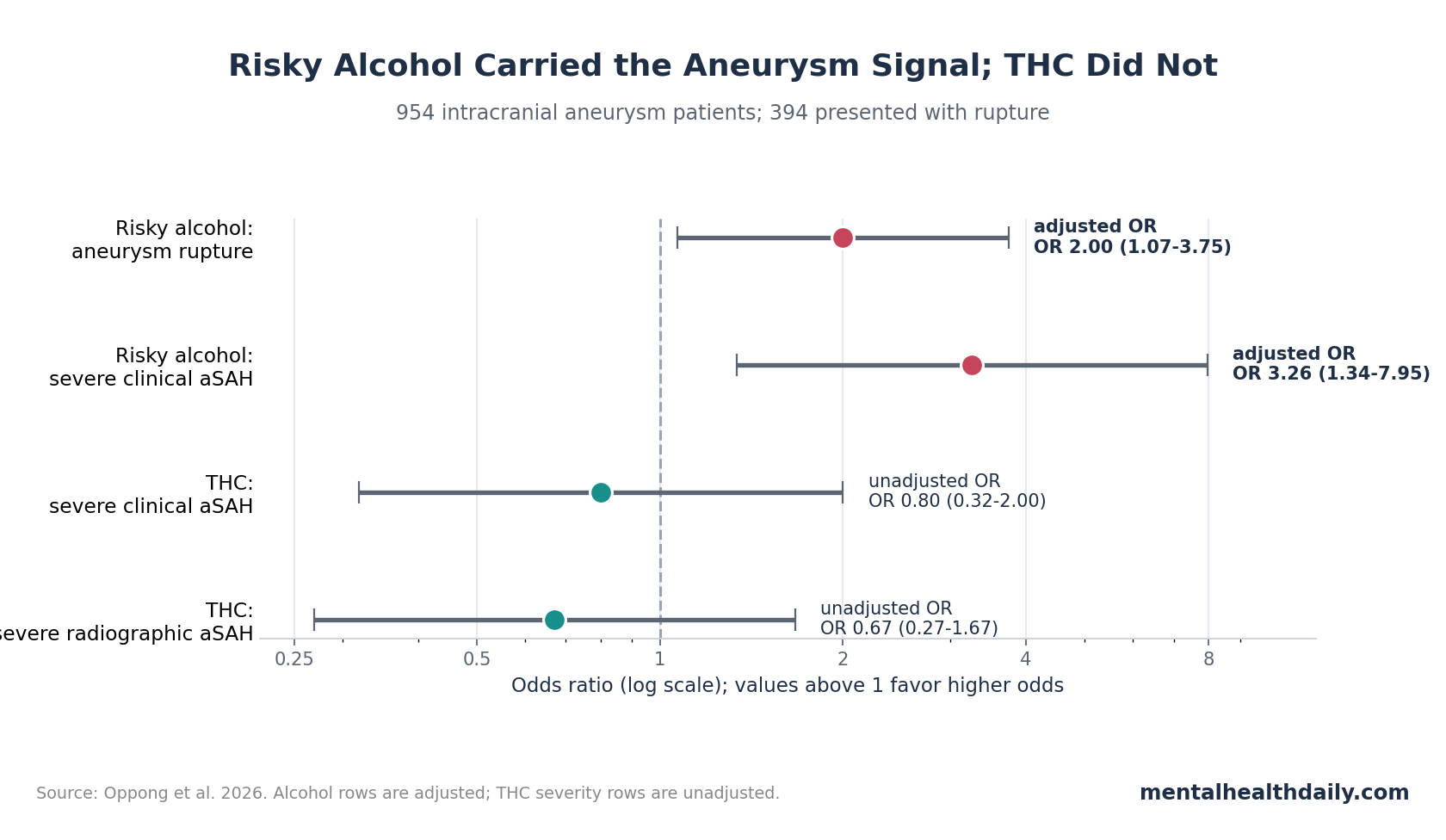
- Risky alcohol was the main signal: drinking above the study threshold was independently associated with aneurysm rupture (aOR = 2.00; 95% CI 1.07-3.75; p = 0.031).
- Clinical severity rose more sharply: among patients with aneurysmal subarachnoid hemorrhage, risky alcohol use was tied to 3.26x higher adjusted odds of severe WFNS grade IV-V presentation.
- THC did not separate rupture or severity: THC use was reported by 5.3% of the cohort, but rupture (p = 0.756), clinical severity (OR = 0.80), and radiographic severity (OR = 0.67) were not significantly different.
- Polysubstance reporting was sparse: polytoxicomania was documented in 3.2%, leaving the analysis underpowered for firm claims about mixed illicit drug exposure.
- The clinical message is threshold-specific: any alcohol use was not the finding; the signal appeared at >20 g/day in males and >10 g/day in females.
Aneurysmal subarachnoid hemorrhage means bleeding into the space around the brain after an intracranial aneurysm ruptures. It is a neurological emergency, and prevention counseling works best when it separates specific exposures that still predict rupture or severe presentation after ordinary aneurysm risk factors are considered.
Oppong et al. found a clear risky-alcohol signal and a non-significant THC signal in the same prospective aneurysm registry. That split is useful because “recreational substance use” is too broad a category for counseling patients with known intracranial aneurysms.
Risky Alcohol Use Was Linked to 2.00x Higher Rupture Odds
Oppong et al. analyzed 954 adults treated for intracranial aneurysm at a German tertiary center between July 2016 and October 2023. The cohort included both unruptured and ruptured aneurysms, with 394 patients (41.3%) presenting after aneurysm rupture.
Risky alcohol use was defined as average intake above 20 g/day for males or above 10 g/day for females over the prior 12 months. That threshold separated the study from simpler “any drinking” analyses, because any alcohol consumption was common but did not predict rupture in this dataset.
The exposure counts were small but clinically relevant:
- Risky alcohol use: 4.6% of the full aneurysm cohort.
- THC use: 51 patients, or 5.3% of the cohort.
- Polytoxicomania: 31 patients, or 3.2% of the cohort, defined as using 2 or more recreational drugs other than alcohol.
In univariate analysis, risky alcohol use was associated with ruptured intracranial aneurysm (OR = 2.13; 95% CI 1.15-3.94; p = 0.014). The signal survived adjustment for sex, age over 70 years, smoking, arterial hypertension, family history of intracranial aneurysm, and aneurysm sac size over 7 mm: aOR = 2.00 (95% CI 1.07-3.75; p = 0.031).
How to read the adjusted odds ratio: within this treated aneurysm cohort, patients who crossed the risky-alcohol threshold had roughly 2x higher adjusted odds of presenting with rupture than patients who did not cross that threshold. The analysis does not prove that reducing alcohol intake will prevent rupture in a specific individual, but it identifies a modifiable exposure that remained visible after major covariates were included.
Clinically Severe aSAH Rose 3.26x, But Radiographic Severity Did Not
Among patients with ruptured aneurysm, the study separated clinical severity from radiographic severity. Clinical severity used the World Federation of Neurosurgical Societies scale, where grades IV-V indicate poor-grade aneurysmal subarachnoid hemorrhage. Radiographic severity used the modified Fisher scale, where grades 3-4 indicate more severe bleeding patterns on imaging.
Risky alcohol use was associated with severe clinical presentation. In the adjusted model, risky alcohol use carried aOR = 3.26 for WFNS grade IV-V presentation (95% CI 1.34-7.95; p = 0.009).
Radiographic severity did not show the same pattern. Risky alcohol use was not significantly associated with modified Fisher grade 3-4 bleeding (OR = 0.93; 95% CI 0.40-2.14; p = 0.856).
Interpretation: risky alcohol use may track neurological impairment at presentation through pathways beyond larger visible hemorrhage volume. The study team proposed several plausible mechanisms, including transient or chronic hypertension, platelet dysfunction, alcohol-related coagulopathy, oxidative stress, mitochondrial injury, and worse baseline frailty.
Clinical limit: the clinical-vs.-radiographic split is an association, not mechanism proof. A patient can arrive with severe neurological impairment for reasons that include hemorrhage burden, early brain injury, hydrocephalus, seizures, systemic illness, or pre-rupture physiology. The study shows that risky alcohol use tracked severe WFNS presentation after adjustment; it does not isolate which pathway did the damage.
THC Showed No Significant Rupture or Severity Signal
THC (tetrahydrocannabinol) is the main intoxicating cannabinoid in cannabis. In this cohort, THC use did not significantly predict intracranial aneurysm rupture, clinical severity, radiographic severity, aneurysm size, irregular aneurysm shape, posterior circulation location, or multiple aneurysm status.
The key numbers were flat:
- Aneurysm rupture: THC use was not significantly associated with rupture (p = 0.756).
- Clinical severe aSAH: THC users had OR = 0.80 for WFNS grade IV-V presentation (95% CI 0.32-2.00; p = 0.633).
- Radiographic severe aSAH: THC users had OR = 0.67 for modified Fisher grade 3-4 bleeding (95% CI 0.27-1.67; p = 0.384).
This is not the same as proving cannabis safety. Only 51 patients reported THC use, exposure was self- or relative-reported, and the data mostly came from the pre-legalization period in Germany, when disclosure could have been especially incomplete.
Adjacent evidence is also mixed. Behrouz et al. reported worse crude outcomes among cannabis users after aneurysmal subarachnoid hemorrhage, but an independent association was not established. Akbik et al. later reported that cannabis use was not associated with aneurysmal subarachnoid hemorrhage complications or outcomes. Chiu et al. found higher perioperative complication rates in cannabis-abuse-coded aneurysm patients, but administrative coding studies can miss dose, route, frequency, and concurrent substance use.
Calibrated read: the 2026 cohort weakens a broad “THC clearly worsens aneurysm rupture” claim, but it does not justify telling patients with intracranial aneurysms that cannabis is cerebrovascularly irrelevant. The honest statement is narrower: in this single-center cohort, reported THC use did not show a statistically significant aneurysm rupture or severity association.
Alcohol Evidence Fits Older Heavy-Drinking Data Better Than Any-Drinking Data
Alcohol has a stronger prior aSAH evidence base than THC. Feigin et al. identified heavy alcohol consumption as a subarachnoid hemorrhage risk factor in a systematic review of epidemiologic studies. Yao et al. later meta-analyzed 14 observational studies and also found higher subarachnoid hemorrhage risk with heavier alcohol consumption. Ali et al. updated the risk-factor literature in 2025 and again kept alcohol in the risk frame.
Can et al. sharpened the aneurysm-specific framing by linking alcohol consumption to aneurysmal subarachnoid hemorrhage and reporting that cessation appeared to remove the excess rupture association. That is not a randomized alcohol-reduction trial, but it supports a modifiable-risk interpretation rather than a fixed-trait interpretation.
The Oppong et al. result fits that literature because the observed signal was not “any alcohol.” Any alcohol consumption was reported by about 2 thirds of the cohort, and it did not predict rupture. The relevant exposure was drinking above the sex-specific risky threshold.
Patient-counseling implication: vague advice to “watch substances” is less useful than explicitly asking about average daily alcohol intake, binge patterns, tobacco, stimulant use, cannabis route and frequency, and polysubstance combinations. The study’s strongest actionable finding sits with alcohol above a risk threshold.
Polysubstance Use Was Too Sparse for Reassurance
Polytoxicomania did not show a significant rupture or severity association in this cohort, but only 31 patients met that definition. Low count, underreporting, and survival bias all matter here: people with severe drug-related hemorrhage may be missed if they die before transfer, never reach specialist aneurysm care, or do not disclose use.
Older adjacent literature gives reasons not to overread the null. Cocaine has been linked to aneurysmal subarachnoid hemorrhage in systematic review work, and stimulant exposure has been associated with vasospasm or poor outcomes in some cohorts. Heroin use has also been linked to ruptured saccular aneurysms in electronic-health-record data.
Evidence-strength note: this was an observational registry analysis with structured interviews, not toxicology-confirmed exposure measurement. It can identify clinically important signals, but it cannot establish causality, dose-response curves, or substance-specific safety thresholds. The THC and polysubstance nulls are especially vulnerable to low power and underreporting.
How to Use the Finding in Aneurysm Counseling
For patients with known intracranial aneurysm, the finding supports direct alcohol screening rather than vague lifestyle documentation. Asking “do you drink?” is weaker than quantifying average grams per day, binge drinking, recent change in intake, and co-exposures that raise blood pressure or impair coagulation.
A practical counseling structure has 4 parts:
- Quantify alcohol exposure: estimate average intake against the study thresholds of >20 g/day for males and >10 g/day for females.
- Separate any drinking from risky drinking: the 2026 result did not make any alcohol use the risk signal.
- Ask about THC without overclaiming: reported THC use was null here, but exposure reporting and sample size were weak.
- Screen stimulant and polysubstance exposure: cocaine, amphetamines, and mixed drug use remain clinically important even if this cohort could not estimate them precisely.
That framing keeps the advice honest. The patient-facing message is not that alcohol is the only vascular concern or that THC is cleared. It is that risky alcohol use was the substance exposure that stayed significant in this specific aneurysm cohort.
Questions About Alcohol, THC, and Aneurysm Rupture
Did the study show that alcohol causes aneurysm rupture?
No. The study showed an independent association between risky alcohol use and rupture in a treated aneurysm cohort. Causality would require prospective intervention or causal-inference designs, but alcohol is modifiable and the result fits older heavy-drinking evidence.
Was ordinary alcohol use associated with rupture?
No clear signal appeared for any alcohol consumption. The significant finding was risky alcohol use above the sex-specific daily threshold.
Does the THC null mean cannabis is safe for people with aneurysms?
No. Reported THC use was not significantly associated with rupture or severity, but the THC subgroup was small and likely affected by underreporting. The result is a null signal in this dataset, not proof of no risk.
Why would alcohol affect clinical severity without increasing radiographic severity?
Alcohol could affect early neurological status through blood pressure instability, impaired clotting, platelet effects, oxidative stress, systemic frailty, or complications not captured by initial blood-volume grading. The study did not prove the mechanism.
References
- Oppong MD, Witte A, Dammann P, Rexhepi A, Ahmadipour Y, Gümüs M, et al. Recreational substance use and aneurysmal subarachnoid hemorrhage: differential effects of alcohol and THC. Neurosurgical Review. 2026;49:369. doi:10.1007/s10143-026-04295-w
- Feigin VL, Rinkel GJ, Lawes CM, Algra A, Bennett DA, van Gijn J, et al. Risk factors for subarachnoid hemorrhage: an updated systematic review of epidemiological studies. Stroke. 2005;36(12):2773-2780. doi:10.1161/01.STR.0000190838.02954.e8
- Yao X, Zhang K, Bian J, Chen G. Alcohol consumption and risk of subarachnoid hemorrhage: a meta-analysis of 14 observational studies. Biomedical Reports. 2016;5(4):428-436. doi:10.3892/br.2016.743
- Ali M, van Eldik MJA, Rietkerken S, Schoones JW, Kruyt ND, Rinkel GJE, et al. Risk factors of aneurysmal subarachnoid hemorrhage including analysis by sex: a systematic review and meta-analysis. Neurology. 2025;104(8):e213511. doi:10.1212/wnl.0000000000213511
- Can A, Castro VM, Ozdemir YH, Dagen S, Dligach D, Finan S, et al. Alcohol consumption and aneurysmal subarachnoid hemorrhage. Translational Stroke Research. 2018;9(1):13-19. doi:10.1007/s12975-017-0557-z
- Behrouz R, Birnbaum L, Grandhi R, Johnson J, Misra V, Palacio S, et al. Cannabis use and outcomes in patients with aneurysmal subarachnoid hemorrhage. Stroke. 2016;47(5):1371-1373. doi:10.1161/STROKEAHA.116.013099
- Akbik F, Konan HD, Williams KP, Ermias LM, Shi Y, Takieddin O, et al. Cannabis use is not associated with aneurysmal subarachnoid hemorrhage complications or outcomes. Stroke. 2022;53(8):e375-e376. doi:10.1161/STROKEAHA.122.038951
- Chiu RG, Fuentes AM, Patil SN, Chiu R, McGuire LS, Mehta AI. Cannabis abuse and perioperative complications after treatment of intracranial aneurysms: a nationwide analysis. World Neurosurgery. 2022;158:e184-e195. doi:10.1016/j.wneu.2021.10.156
- Florez-Perdomo WA, Reyes Bello JS, Garcia-Ballestas E, Moscote-Salazar LR, Barthelemy EJ, Janjua T, et al. Aneurysmal subarachnoid hemorrhage and cocaine consumption: a systematic review and metanalysis. World Neurosurgery. 2024;184:241-252.e2. doi:10.1016/j.wneu.2023.12.020
- Can A, Castro VM, Ozdemir YH, Dagen S, Dligach D, Finan S, et al. Heroin use is associated with ruptured saccular aneurysms. Translational Stroke Research. 2018;9(4):340-346. doi:10.1007/s12975-017-0582-y