A 2026 case-control study found that treatment-naive adults with attention-deficit/hyperactivity disorder (ADHD) had much lower serum SIRT-1, Nrf-2, and HO-1 than matched controls, while TNF-α did not differ. The pattern points more toward impaired antioxidant-defense regulation than a simple broad-inflammation story.
Research Highlights
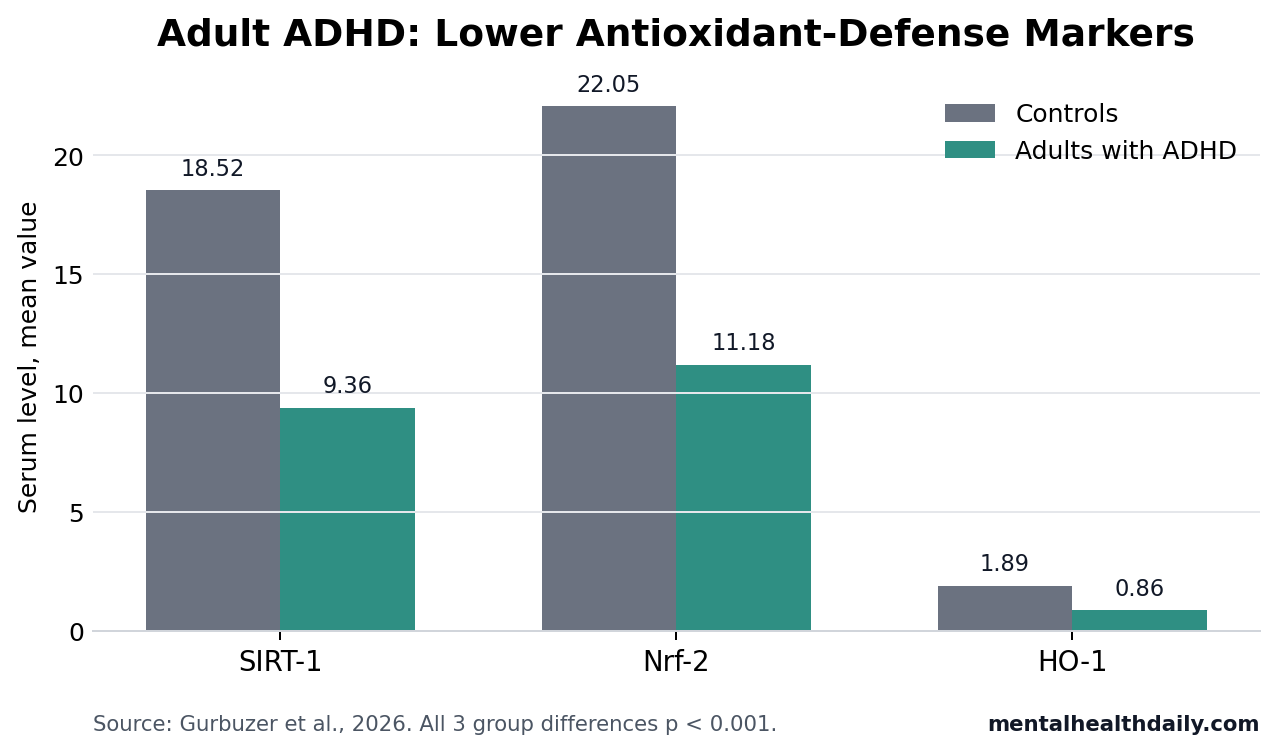
- Antioxidant-defense markers were lower: adults with ADHD had lower SIRT-1 (9.36 vs. 18.52), Nrf-2 (11.18 vs. 22.05), and HO-1 (0.86 vs. 1.89) than controls, all with p < 0.001.
- Classic cytokine inflammation did not separate groups: TNF-α was 7.49 in ADHD vs. 7.78 in controls (p = 0.439), even though CRP was modestly higher (3.50 vs. 2.86 mg/L; p = 0.036).
- Symptoms tracked the same axis: lower Nrf-2 correlated with higher total Adult ADHD Self-Report Scale scores (r = −0.446; p < 0.001), with similar correlations for SIRT-1 and HO-1.
- Classification was moderate, not diagnostic: HO-1 reached AUC 0.797, Nrf-2 AUC 0.756, and SIRT-1 AUC 0.753 for separating ADHD from controls.
- The causal question remains open: 120 adults were measured at 1 time point, so the data cannot show whether redox dysregulation drives ADHD symptoms, follows them, or reflects a related exposure.
Oxidative stress means that reactive oxygen and nitrogen molecules are outpacing the cell’s ability to neutralize them. In the brain, that imbalance is plausible because neurons consume high amounts of oxygen, contain oxidation-prone lipids, and depend on tightly regulated mitochondrial energy production.
The useful part of the Gurbuzer et al. study was not another generic oxidative-stress marker. It measured 3 upstream defense regulators: SIRT-1, an enzyme involved in stress resistance and metabolic regulation; Nrf-2, a transcription factor that turns on antioxidant-response genes; and HO-1, an Nrf-2-linked enzyme that helps process heme and respond to oxidative stress. Those 3 markers sit closer to the cell’s defense machinery than a downstream damage product.
Adults With ADHD Had About Half the SIRT-1 and Nrf-2 Levels of Controls
The 2026 study enrolled 60 adults with ADHD and 60 healthy controls matched by age and sex. ADHD diagnosis used the Structured Clinical Interview for DSM-5 and the Diagnostic Interview for ADHD in Adults, and the ADHD group was treatment-naive with no comorbid psychopathology other than ADHD.
Compared with controls, adults with ADHD showed a broad reduction across the SIRT-1/Nrf-2/HO-1 axis:
- SIRT-1: 9.36 in ADHD vs. 18.52 in controls (p < 0.001; Cohen’s d = 0.73).
- Nrf-2: 11.18 in ADHD vs. 22.05 in controls (p < 0.001; Cohen’s d = 0.75).
- HO-1: 0.86 in ADHD vs. 1.89 in controls (p < 0.001; Cohen’s d = 0.77).
Those effect sizes were medium-to-large for a peripheral biomarker study. They also moved together: within the ADHD group, HO-1 correlated strongly with Nrf-2 (r = 0.965) and SIRT-1 (r = 0.922), and Nrf-2 correlated strongly with SIRT-1 (r = 0.932).
That clustering makes the result more coherent than 3 isolated positive findings. It suggests a coordinated redox-regulatory signal, although it also means the markers are not independent biological facts in the statistical sense.
TNF-α Did Not Support a Simple Inflammation Claim
TNF-α (tumor necrosis factor alpha) is a proinflammatory cytokine, meaning a signaling protein that can amplify immune activity. If the study had found a large TNF-α difference, the easy headline would have been that adult ADHD looks like a peripheral inflammatory state.
It did not. TNF-α averaged 7.49 in adults with ADHD and 7.78 in controls (p = 0.439), a near-null group contrast. CRP (C-reactive protein, a nonspecific systemic inflammation marker) was modestly higher in the ADHD group, but the effect size was small-to-moderate: 3.50 vs. 2.86 mg/L (p = 0.036; d = 0.39).
Biological interpretation: the data fit impaired antioxidant-defense regulation better than a claim that adult ADHD is defined by overt peripheral inflammation. That distinction is useful because oxidative stress and inflammation are connected, but they are not interchangeable. A single cytokine can be unchanged while upstream stress-response systems still look altered.
Lower SIRT-1, Nrf-2, and HO-1 Tracked Worse ADHD Symptoms
The biomarker pattern also related to symptom burden inside the ADHD group. Total Adult ADHD Self-Report Scale scores correlated negatively with HO-1 (r = −0.424; p = 0.001), Nrf-2 (r = −0.446; p < 0.001), and SIRT-1 (r = −0.430; p = 0.001).
The inattention subscale showed the clearest relationship. After controlling for age, SIRT-1 added 16.6% explained variance for inattention severity (R2 change = 0.166; p = 0.001), with lower SIRT-1 linked to higher inattention scores (β = −0.407; p = 0.001).
Hyperactivity/impulsivity also moved in the same direction, but less strongly. SIRT-1 explained 8.1% of the variance in hyperactivity/impulsivity scores (p = 0.028), and the standardized association was smaller (β = −0.284).
Practical read: this is a severity signal, not a treatment rule. It does not say that raising SIRT-1 would reduce ADHD symptoms. It says that, in this sample, lower measured antioxidant-defense activity traveled with higher reported symptoms.
Prior ADHD Oxidative-Stress Evidence Was Real but Messy
Earlier work makes the 2026 result plausible, but not settled. Joseph et al. performed a meta-analysis of oxidative-stress markers in ADHD and found enough abnormality to keep the biology on the map, while also exposing marker-level heterogeneity.2 Lopresti’s review reached a similar calibrated position: oxidative and nitrosative stress may contribute to ADHD biology, but antioxidant-targeted therapy was still an evidence question rather than a proven clinical approach.3
Alvarez-Arellano et al. framed antioxidants as possible targets against inflammation and oxidative stress in ADHD, which is a narrower claim than saying ADHD has a validated redox treatment pathway.4 Uzun Cicek et al. reported reduced SIRT1 in children with ADHD and linked it to cognitive performance, giving the adult study a developmental comparison point rather than a completely isolated finding.5
What changed in the adult study: the strongest signal came from an upstream regulatory axis, not from a broad cytokine panel. That helps explain why ADHD biomarker studies can look inconsistent when they mix damage markers, inflammatory markers, antioxidant enzymes, iron indices, medication exposure, age groups, and assay platforms.
HO-1, Nrf-2, and SIRT-1 Are Not Ready as ADHD Blood Tests
Receiver operating characteristic analysis tested whether each biomarker separated adults with ADHD from controls. HO-1 performed best, with AUC 0.797 (95% CI 0.716-0.878). Nrf-2 reached AUC 0.756 (95% CI 0.668-0.844), and SIRT-1 reached AUC 0.753 (95% CI 0.665-0.841).
AUC (area under the curve) ranges from 0.5 for chance-level separation to 1.0 for perfect separation. Values around 0.75-0.80 are meaningful for group-level biology, but they are not strong enough to diagnose an individual adult with ADHD.
The cutoffs also show the limits. HO-1 at 0.87 yielded 78.3% sensitivity and 76.7% specificity. Nrf-2 at 9.8 yielded 70% sensitivity and 73.3% specificity. SIRT-1 at 8.3 yielded 75% sensitivity and 70% specificity. Those numbers miss too many cases and misclassify too many controls for standalone clinical use.
Limitations of This Adult ADHD Biomarker Study
The main boundary is design. A cross-sectional case-control study can identify associations, not causation. Lower SIRT-1, Nrf-2, and HO-1 could reflect ADHD biology, stress load, sleep differences, diet, activity, socioeconomic factors, unmeasured inflammation, or another exposure correlated with ADHD symptoms.
Several constraints matter for interpretation:
- Peripheral measurement: serum markers are indirect proxies for central nervous system biology.
- Single-center sample: all participants came from one clinical setting, which limits generalizability.
- Selective eligibility: the study excluded obesity, acute or chronic inflammatory disease, recent infection, psychotropic medication use, and comorbid psychopathology.
- Unmeasured daily exposures: diet and sleep patterns were not systematically evaluated, even though both can affect oxidative and inflammatory markers.
- No longitudinal direction: the study did not test whether the biomarker pattern changes with treatment, symptom improvement, or time.
That makes the result best read as a biologically coherent signal in a carefully selected adult ADHD sample, not a diagnostic tool or supplement recommendation.
Questions About Adult ADHD and Antioxidant-Defense Biomarkers
Does this mean oxidative stress causes adult ADHD?
No. The study measured adults with and without ADHD at 1 time point, so it cannot establish cause. It supports an association between adult ADHD and lower SIRT-1/Nrf-2/HO-1 antioxidant-defense markers.
Could SIRT-1, Nrf-2, or HO-1 become part of an ADHD blood test?
Not as standalone markers based on these data. AUC values between 0.753 and 0.797 show moderate group separation, but the sensitivity and specificity values are not strong enough for individual diagnosis.
Does the study support anti-inflammatory treatment for ADHD?
Not directly. TNF-α did not differ between groups, and CRP was only modestly higher. The stronger signal was in antioxidant-defense regulation, which is related to inflammation but not the same target.
What would make this finding clinically useful?
Longitudinal studies would need to show whether SIRT-1, Nrf-2, and HO-1 predict symptom course, treatment response, or biologically defined ADHD subgroups. Intervention studies would then need to test whether changing that pathway improves ADHD-relevant outcomes.
Bottom line: the 2026 adult ADHD study found a coherent SIRT-1/Nrf-2/HO-1 antioxidant-defense deficit, with moderate links to symptom severity and moderate group-separation statistics. The finding strengthens the redox-biology case in ADHD, but it does not establish causality, diagnosis, or treatment guidance.
References
- Gurbuzer N, Ozkaya A, Mercantepe F. The SIRT-1/Nrf-2/HO-1 antioxidant defense axis in adult attention-deficit/hyperactivity disorder. Metabolic Brain Disease. 2026;41:85. doi:10.1007/s11011-026-01845-5
- Joseph N, Zhang-James Y, Perl A, Faraone SV. Oxidative stress and ADHD: a meta-analysis. Journal of Attention Disorders. 2015;19(11):915-924. doi:10.1177/1087054713510354
- Lopresti AL. Oxidative and nitrosative stress in ADHD: possible causes and the potential of antioxidant-targeted therapies. ADHD Attention Deficit and Hyperactivity Disorders. 2015;7:237-247. doi:10.1007/s12402-015-0170-5
- Alvarez-Arellano L, Gonzalez-Garcia N, Salazar-Garcia M, Corona JC. Antioxidants as a potential target against inflammation and oxidative stress in attention-deficit/hyperactivity disorder. Antioxidants. 2020;9(2):176. doi:10.3390/antiox9020176
- Uzun Cicek A, Mercan Isik C, Bakir S, et al. Evidence supporting the role of telomerase, MMP-9, and SIRT1 in attention-deficit/hyperactivity disorder (ADHD). Journal of Neural Transmission. 2020;127:1409-1418. doi:10.1007/s00702-020-02231-w
- Leffa DT, Torres ILS, Rohde LA. A review on the role of inflammation in attention-deficit/hyperactivity disorder. Neuroimmunomodulation. 2018;25:328-333. doi:10.1159/000489635