A 2026 secondary analysis of the HomePAP trial found that each 10 L/min more unintentional CPAP mask leak was associated with 26.6 fewer PAP minutes per night and 7.2 percentage-point fewer adherent days, but the new Real Leak metric did not significantly outperform ordinary device-reported Average Leak.1
Research Highlights
- Real Leak tracked poorer adherence: each 10 L/min higher Real Leak was associated with 26.6 fewer PAP minutes per night and 7.2 percentage-point fewer days with at least 4 hours of use.1
- Average Leak gave a similar signal: each 10 L/min higher Average Leak was associated with 20.1 fewer PAP minutes per night and 5.5 percentage-point fewer adherent days.1
- Real Leak was not clearly stronger than Average Leak: the 2 metrics were highly correlated at 3 months (rho = 0.90, 95% CI 0.85-0.93), and the researchers reported no significant performance difference.1
- Adherence remained low: only 46.2% of patients met the usual “4 and 70” PAP adherence rule at 3 months, meaning at least 4 hours of use on at least 70% of nights.1
- Leak is measurable but not the whole problem: race and apnea-hypopnea index (AHI) independently predicted adherence, while education time, troubleshooting interventions, and PAP optimism did not in the adjusted models.1
Positive airway pressure (PAP) therapy keeps the upper airway open during sleep with pressurized air. CPAP is the best-known PAP format, and it can normalize obstructive sleep apnea (OSA) physiology when the mask fits, the pressure is adequate, and the patient can tolerate nightly use.
PAP success extends beyond prescribing the device. PAP has to be used long enough, often enough, and comfortably enough to matter. Across 20 years of CPAP adherence data, nonadherence has remained stubbornly common rather than disappearing as machines improved.2
Real Leak Means Unintentional Mask Leak
Intentional leak is expected vent flow built into a PAP mask so carbon dioxide does not build up inside the mask. Unintentional leak is the extra air escaping because the mask seal is poor, the mouth opens, the interface shifts during sleep, or pressure overwhelms the fit.
Andrews et al. called their derived unintentional-leak metric Real Leak. They took device-reported Average Leak over the prior 30 days, then subtracted mask-specific intentional leak based on the manufacturer table for that mask and pressure setting.1
The idea is clinically sensible. A nasal mask, nasal pillow mask, and full-face mask can have different expected leak at the same pressure. Raw leak numbers therefore mix 2 things:
- Expected venting: flow the mask needs to be safe.
- Actionable leak: unintended air loss that may cause noise, dry mouth, eye irritation, pressure instability, residual events, or sleep disruption.
The study tested whether separating those 2 sources made adherence prediction better than using Average Leak alone.
HomePAP Supplied a Cleaner Adherence Dataset
The analysis used data from the multisite HomePAP trial, a randomized study comparing a home sleep apnea testing and autotitration pathway against laboratory polysomnography and laboratory titration for diagnosing and treating OSA.3 Andrews et al. analyzed PAP download data from 139 participants at 1 month and 124 participants at 3 months.1
Participants had high pretest probability of moderate-to-severe OSA. Median diagnostic apnea-hypopnea index was 36.8 events/hour, meaning the typical participant was in the severe OSA range. Mean age was 48.4 years, 65.3% were male, median body mass index was 36.3 kg/m2, and 68.7% were White.1
Mask distribution also matters because leak is partly interface-dependent: 62.6% used nasal masks, 18.5% used nasal pillows, and 16.9% used full-face masks. Median intentional leak was 26.6 L/min, while median Real Leak was 15.5 L/min at 3 months. Device-reported Average Leak was much higher at 41.4 L/min because it included both expected venting and unintended leak.1
Every 10 L/min More Leak Predicted Less PAP Use
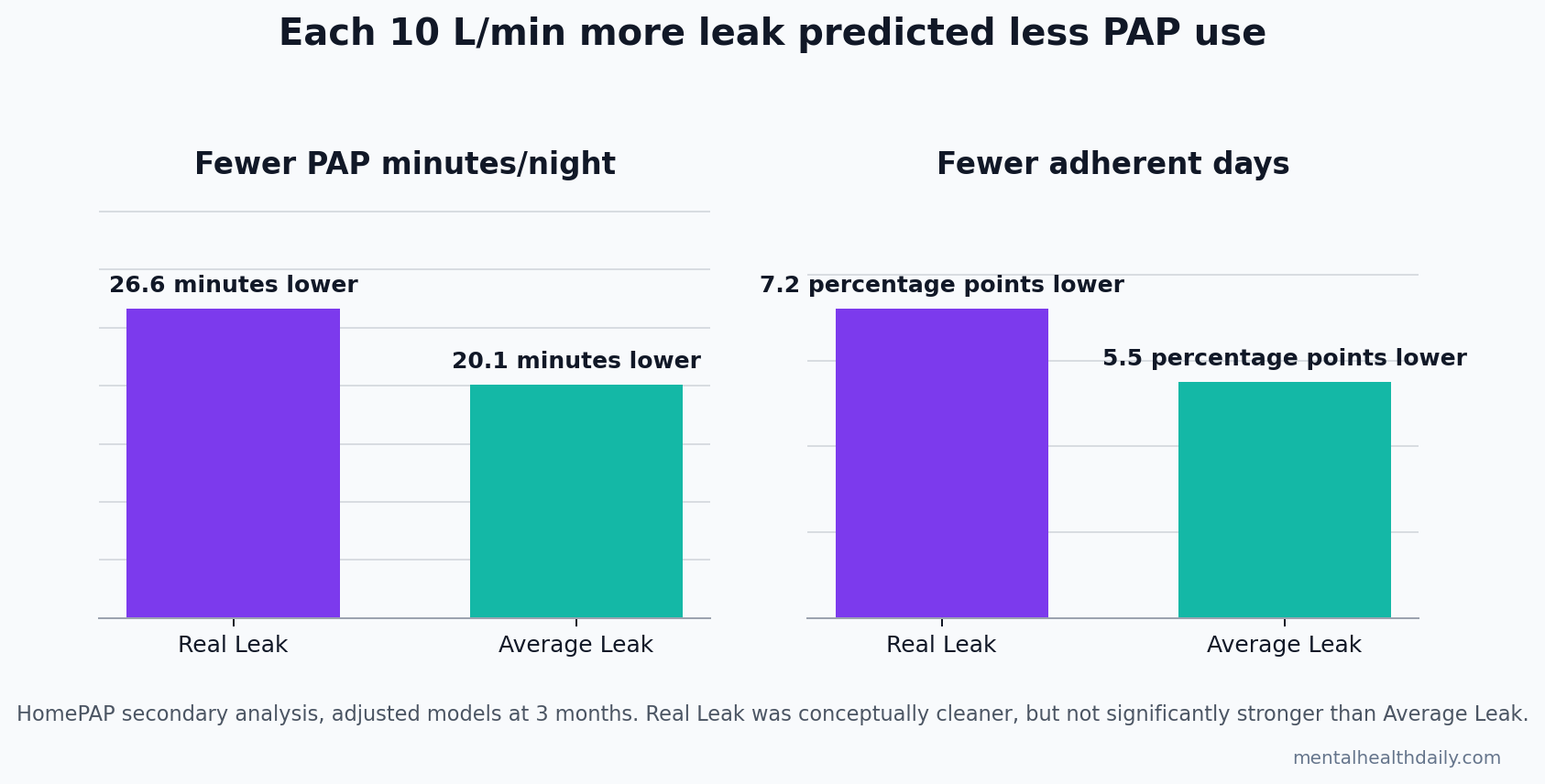
The strongest reader-facing result is the 10 L/min translation. For Real Leak, 10 L/min more leak corresponded to 26.6 fewer PAP minutes per night and 7.2 percentage-point fewer days with at least 4 hours of use. For Average Leak, the corresponding numbers were 20.1 fewer minutes and 5.5 percentage-point fewer adherent days.1
The 1 L/min regression coefficients were smaller but point in the same direction: Real Leak predicted 2.66 fewer minutes per night (95% CI −4.79 to −0.53, p = 0.015) and 0.72 percentage-point fewer adherent days (95% CI −1.24 to −0.19, p = 0.008). Average Leak predicted 2.01 fewer minutes per night (95% CI −3.87 to −0.15, p = 0.035) and 0.55 percentage-point fewer adherent days (95% CI −1.01 to −0.10, p = 0.018).1
Those associations were adjusted for age, sex, body mass index, race, education, baseline Epworth Sleepiness Scale score, and AHI. The design still cannot prove that fixing leak would automatically recover 20-27 minutes per night, but the direction is clinically coherent: more air escaping from the system went with less use.
Real Leak Was Clearer, Not Clinically Dominant
The result should not be oversold as a new metric replacing the old one. Real Leak and Average Leak were highly correlated because Real Leak was derived from Average Leak. At 1 month, rho was 0.73 (95% CI 0.61-0.81); at 3 months, rho was 0.90 (95% CI 0.85-0.93), with p < 0.001 at both timepoints.1
Point estimates leaned toward Real Leak, but Andrews et al. reported no significant performance difference between Real Leak and Average Leak. The calibrated conclusion is narrow: adjusting for intentional leak made the concept cleaner, but the available HomePAP data did not prove meaningfully better prediction.
That still leaves a practical reason to care. Sleep-device leak reports can be difficult to compare across masks, devices, pressure settings, and manufacturers. A metric that names unintentional leak directly may help patients, technologists, and clinicians talk about the same problem without confusing expected vent flow with an avoidable mask-seal problem.
Prior Leak Evidence Was Inconsistent but Pointed the Same Way
Earlier leak research already suggested that leak belongs in adherence conversations. Valentin et al. analyzed AutoPAP therapy and found that air leak was associated with poor adherence, making leak both a technical problem and an adherence problem.4
Lebret et al. reviewed unintentional leak during CPAP treatment and found that leak reporting was surprisingly thin: only 21 randomized controlled trials over 26 years reported unintentional leak, and studies used inconsistent leak definitions.5 That inconsistency is exactly the gap the Real Leak paper tried to address.
Mask interface evidence also fits the same pattern. Bakker et al. compared nasal and oronasal CPAP masks and found that interface choice can alter pressure requirement, residual disease, and leak.6 For a patient struggling with PAP, leak is therefore part of a broader interface-and-pressure system rather than a single number on a download.
Leak Repair Is Necessary but Not Sufficient
Adherence in the HomePAP leak analysis improved from 36.9% at 1 month to 46.2% at 3 months, but more than half of participants still failed the usual threshold at 3 months.1 Leak alone does not explain that.
Several non-leak signals stood out:
- Race: White participants had a higher percentage of adherent days than Black participants, 63.14 vs. 41.33, after adjustment (p = 0.02). The study did not identify the cause, so the finding should be treated as an access, support, trust, equipment, follow-up, or social-context signal rather than a biological claim.
- OSA severity: each 1-point higher AHI was associated with 0.46 percentage-point more adherent days (p < 0.001), possibly because more severe symptoms create more noticeable benefit from PAP.
- Troubleshooting did not predict adherence: number of interventions, PAP education time, and baseline optimism were not independent predictors in the model. Those null model terms should be read narrowly: this dataset did not isolate a measurable effect from them.
Evidence strength is therefore moderate for association and weaker for intervention. This secondary analysis supports measuring and addressing leak, but it does not prove that a specific leak-reduction protocol will improve long-term adherence across routine clinics.
Practical PAP Takeaways From the Leak Data
Watch leak trends, not one-night noise. Andrews et al. used 30-day averages. A single bad night after congestion or mask displacement is less informative than a persistent rise in leak across weeks.
Ask which leak number the device is showing. Average Leak, large leak time, intentional leak, and unintentional leak are not the same measurement. A clinician or sleep technologist should know whether the number includes expected mask venting.
Translate leak into symptoms. Dry mouth, air blowing into the eyes, mask noise, pressure surges, awakenings, residual sleepiness, and bed-partner complaints can make a download number clinically meaningful.
Fix the interface before blaming motivation. A patient who removes PAP after 3 hours may not be “noncompliant” in the moral sense. The mask may be leaking enough to make sleep worse than untreated OSA.
Questions About CPAP Mask Leak and PAP Adherence
Does Real Leak mean my CPAP machine is giving the wrong pressure?
Not automatically. Real Leak estimates unintended air loss after expected mask venting is subtracted. Large or persistent leak can interfere with comfort, pressure delivery, and device algorithms, but the exact clinical meaning depends on the device, mask, pressure, residual AHI, symptoms, and leak pattern.1
Is Real Leak better than Average Leak?
It is conceptually cleaner because it tries to remove intentional mask venting. In the HomePAP analysis, however, Real Leak did not significantly outperform Average Leak, and the 2 metrics were highly correlated at 3 months (rho = 0.90).1
What should a patient do if leak is high?
Start with mask fit, cushion age, strap tension, sleeping position, nasal congestion, mouth leak, humidification, and whether the mask type matches pressure needs. A sleep clinic can review the detailed download rather than relying on a single summary number.
Does a full-face mask cause worse adherence?
Not proven here. At 3 months, adherence was 65.0% for nasal masks, 58.6% for nasal pillows, and 41.7% for full-face masks, but the difference was not statistically significant (p = 0.76).1
Can leak explain every CPAP adherence problem?
No. Leak is one modifiable technical barrier. Claustrophobia, insomnia, pressure intolerance, nasal obstruction, cost, follow-up quality, work schedule, depression, bed-partner dynamics, and whether the patient feels symptomatic benefit can all affect PAP use.
References
- What’s leak got to do with it? Association of mask leak and positive airway pressure adherence from the HomePAP study. Andrews ND et al. Journal of Clinical Sleep Medicine. 2026;22:55. doi:10.1007/s44470-026-00046-2
- Trends in CPAP adherence over 20 years of data collection: a flattened curve. Rotenberg BW, Murariu D & Pang KP. Journal of Otolaryngology – Head & Neck Surgery. 2016;45:43. doi:10.1186/s40463-016-0156-0
- A multisite randomized trial of portable sleep studies and positive airway pressure autotitration versus laboratory-based polysomnography for the diagnosis and treatment of obstructive sleep apnea: the HomePAP study. Rosen CL et al. Sleep. 2012;35(6):757-767. doi:10.5665/sleep.1870
- Air leak is associated with poor adherence to AutoPAP therapy. Valentin A, Subramanian S, Quan SF, Berry RB & Parthasarathy S. Sleep. 2011;34(6):801-806. doi:10.5665/SLEEP.1054
- Factors contributing to unintentional leak during CPAP treatment: a systematic review. Lebret M et al. Chest. 2017;151(3):707-719. doi:10.1016/j.chest.2016.11.049
- Nasal versus oronasal continuous positive airway pressure masks for obstructive sleep apnea: a pilot investigation of pressure requirement, residual disease, and leak. Bakker JP, Neill AM & Campbell AJ. Sleep and Breathing. 2012;16(3):709-716. doi:10.1007/s11325-011-0564-3