A 2026 EEG study of 106 Army National Guard recruits found that higher negative emotionality predicted poorer Go/No-Go discrimination (β = −.234, 95% CI −.392 to −.076) and lower frontal midline theta (β = −.149, 95% CI −.290 to −.001). The key result was not a vague personality-brain link: frontal midline theta, not occipital alpha, mediated the path from negative emotionality to worse cognitive-control performance than lower-NEM recruits.1
Research Highlights
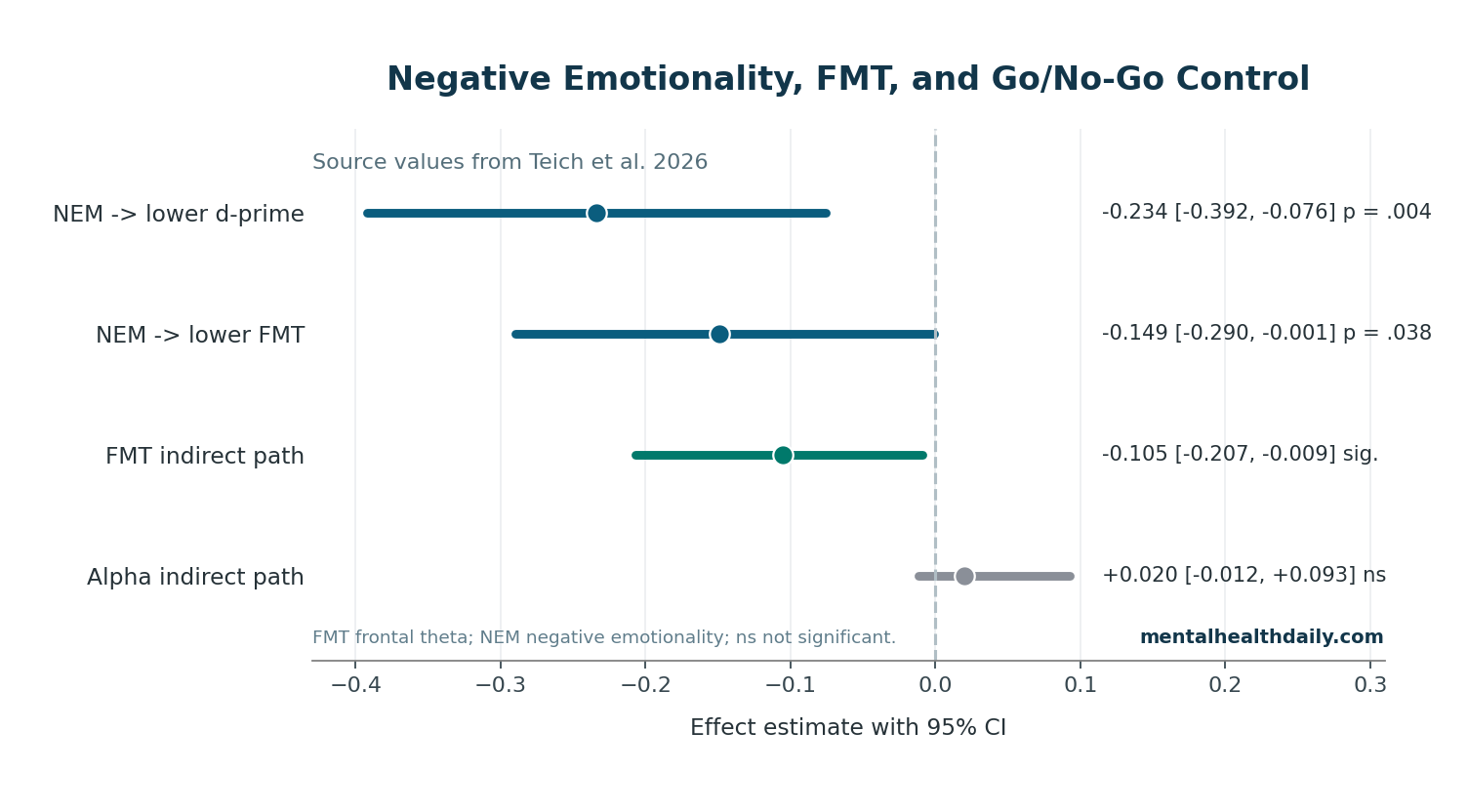
- Higher NEM tracked worse discrimination than lower NEM: recruits with higher negative emotionality had lower d-prime across task blocks (β = −.234, 95% CI −.392 to −.076; p = .004).1
- FMT moved in the predicted low-control direction: higher NEM was associated with attenuated frontal midline theta during correct Go/No-Go trials (β = −.149, 95% CI −.290 to −.001; p = .038).1
- The mediation signal was source-specific: FMT mediated the NEM-to-d-prime relationship (ab = −.105, 95% bootstrapped CI −.207 to −.009), while occipital alpha did not (ab = .020, 95% CI −.012 to .093).1
- The difficult block behaved as intended: d-prime dropped to 1.30 in Block 2 vs. 1.44 in Block 1 and 1.53 in Block 3, with Block 2 lower than both standard blocks (p < .001).1
- This is not a clinical EEG test: the design used 106 mostly healthy pre-training recruits, cross-sectional mediation, and correct-trial EEG windows; it cannot diagnose anxiety, PTSD, or depression in 1 person.1
Negative emotionality (NEM) is a stable personality dimension covering stress reactivity, fearfulness, anger, alienation, and emotional volatility. Teich et al. studied it because NEM is a broad vulnerability trait, but the paper’s more interesting move was mechanistic: it asked whether a measurable EEG control signal explains why high-NEM people perform worse when a task requires response inhibition.
Frontal midline theta (FMT) is 3–8 Hz electrical activity recorded over front-central scalp sites such as FCz. In cognitive-control tasks, it usually rises when the brain needs to detect conflict, inhibit a response, monitor errors, or allocate effort.2
The 2026 recruit study therefore gives a fairly direct test of whether the control system engages normally when high-NEM participants face a demanding Go/No-Go task.
106 Recruits Were Tested Before Basic Combat Training
Teich et al. analyzed 106 Minnesota Army National Guard recruits from the ARMOR cohort before they shipped to Basic Combat Training. The larger substudy enrolled 123 participants, enriched the lab sample for psychosocial-risk range, and excluded 4 of 110 valid-EEG participants because response-validity scores on the Multidimensional Personality Questionnaire were outside prespecified thresholds.1
The final sample was young and mostly male: mean age 20.2 years, 67.0% male, 31.1% female, 63.2% White, and 14.2% multiracial. The average NEM T-score was 56.7 (SD 12.6), which means the group was not a diagnosed clinical sample but still contained enough trait variation to test whether emotional reactivity was tied to EEG control signals.
The Go/No-Go task required recruits to press for ordinary letter trials and withhold a response when the current letter repeated the prior letter. Block 2 was the stress-test block: it used fewer trials, harsher penalties, and less added response time after No-Go errors.
That design produced the expected performance squeeze, with d-prime falling to 1.30 in Block 2 vs. 1.44 in Block 1 and 1.53 in Block 3.
Higher Negative Emotionality Predicted Lower D-Prime and More Variable Responses
D-prime is a signal-detection score: higher values mean a participant more cleanly separated Go targets from No-Go lures. The NEM effect was not limited to the hardest block.
Across blocks, higher NEM predicted lower d-prime (β = −.234, 95% CI −.392 to −.076; F(1, 102) = 8.63; p = .004).1
Reaction-time variability pointed in the same control-instability direction. Higher NEM predicted greater response-time standard deviation (β = .139, 95% CI .008 to .271; F(1, 107) = 4.44; p = .038), meaning high-NEM recruits were more than slower or faster on average. Their response timing was less stable.
Constraint was a side signal: this separate personality dimension covering planfulness and harm avoidance predicted slower mean reaction time (β = .201, 95% CI .038 to .364; p = .016), but Teich et al. did not carry that result forward as the central mechanism.
The source-specific pattern was NEM plus FMT plus d-prime, not a broad claim that every personality trait maps neatly onto control performance.
Attenuated FMT Carried the NEM-to-Control Pathway
Correct No-Go trials produced more FMT than correct Go trials, confirming that the EEG measure was behaving like a cognitive-control signal. FMT also declined from Block 1 to Blocks 2 and 3, a pattern the researchers interpreted as possible habituation, fatigue, practice, or changing effort as the block structure shifted.
The individual-difference result was sharper: higher NEM predicted attenuated FMT (β = −.149, 95% CI −.290 to −.001; p = .038). Absorption also predicted attenuated FMT (β = −.152, 95% CI −.293 to −.010; p = .036), but only NEM produced the central mediated pathway to d-prime.
The mediation model tied those pieces together. For d-prime, the indirect effect through FMT was significant (ab = −.105, 95% bootstrapped CI −.207 to −.009).
The NEM-to-FMT a-path was negative (a = −.200), and the FMT-to-d-prime b-path was positive (b = .527), so the readable interpretation is direct: higher NEM was linked to lower FMT, and lower FMT was linked to poorer discrimination.
Occipital alpha desynchronization did not do the same job. Alpha tracked task demand, especially Block 2, but its indirect effect for the NEM-to-d-prime pathway was not significant (ab = .020, 95% bootstrapped CI −.012 to .093).
That narrows the claim: Teich et al. identified the frontal control signal as the specific mediator of NEM-related performance, while occipital alpha failed the same mediation test.
This Recalibrates the Anxiety-Theta Story
A common shortcut says anxiety raises FMT because anxious people recruit more control during uncertainty. Cavanagh and Shackman, for example, synthesized evidence that FMT often reflects the overlap between anxiety and cognitive control, especially under action-outcome uncertainty.3
Teich et al. found a different pattern in a mostly nonclinical recruit sample: higher NEM was linked to lower task-evoked FMT during correct trials.
The difference is not necessarily a contradiction. The recruit study measured MPQ-NEM, a broader trait that includes stress reaction, alienation, and aggression, more than anxious threat sensitivity.
It also analyzed correct trials in a behavioral-inhibition task with relatively clear action outcomes, rather than error-locked theta or ambiguous threat processing. Under those conditions, attenuated FMT may mark under-recruitment of control resources rather than compensatory over-engagement.
Buzzell et al. gives the closest adjacent signal. In adolescents, disrupted mediofrontal theta during cognitive control linked early psychosocial neglect to broad psychopathology risk, and theta functioned as a mediator rather than a disorder-specific marker.4
White et al. similarly found that stronger cognitive-control network engagement during emotional interference was associated with lower PTSD symptom severity in a trauma-exposed sample.5 Together with McTeague et al.’s cross-disorder control-circuit findings, the pattern favors a transdiagnostic control-system account over a narrow “theta equals anxiety” rule.6
What the Study Can and Cannot Support
It can support a mechanistic risk model. NEM predicted worse discrimination and unstable response timing; attenuated FMT explained part of the NEM-to-d-prime pathway; and posterior alpha failed as the mediator. For a trait-level vulnerability study, that is a coherent source-specific mechanism.
It cannot prove causality. Mediation language can sound causal, but this study measured trait NEM, EEG, and task behavior in the same broad pre-training window. The MPQ was administered before EEG by 53 days on average, which helps temporal ordering, but unmeasured state stress, sleep, motivation, or baseline cognitive ability could still contribute.
It cannot diagnose 1 person. Group-level EEG associations are not individual clinical tests. A high-NEM person may perform well under pressure, and a low-NEM person may still show poor inhibitory control.
The useful claim is population-level vulnerability: under task demand, higher NEM was linked to weaker recruitment of a frontal control rhythm.
It does not settle all theta findings. The paper focused on total FMT power from 200 to 500 ms after correct Go and No-Go stimuli. Error-related theta, feedback-locked theta, emotional-threat tasks, and source-localized medial frontal activity could show different relationships with NEM or psychiatric symptoms.
Practical Read: FMT Is a Research Biomarker, Not a Self-Control Score
The strongest reader-facing takeaway is not that high-NEM people have “less willpower.” The better read is that emotional reactivity and stress sensitivity may load the same control system that supports inhibition, timing stability, and adaptive response selection. When demand rises, the control system may recruit less efficiently in high-NEM individuals.
That interpretation fits ordinary experience without moralizing it. People high in NEM often report that cognitive performance deteriorates under stress, conflict, or sleep loss.
Teich et al. gives that complaint a plausible neural pathway: less frontal theta engagement during control-demanding trials, followed by worse discrimination and more variable responses.
For interventions, the paper points toward research targets rather than routine recommendations. Cognitive-control training, neurofeedback, mindfulness-based attention practice, sleep stabilization, and evidence-based treatment for anxiety or depression could all be studied with FMT as an outcome.
None should be sold as an FMT-normalizing treatment on the basis of this single cross-sectional study.
Questions About Negative Emotionality, FMT, and Control
Did Teich et al. find higher or lower FMT in high-NEM recruits?
Lower. Higher NEM was associated with attenuated FMT (β = −.149, 95% CI −.290 to −.001), which is why the article should not be written as a generic “negative emotion increases theta” story.
Was the Go/No-Go effect only a reaction-time artifact?
No. Higher NEM predicted lower d-prime, a discrimination metric that combines hit rate and false-alarm rate.
NEM also predicted greater response-time variability, but the primary accuracy-style result was lower d-prime.
Why did occipital alpha fail as the mediator?
Occipital alpha desynchronization tracked task demand, especially the difficult Block 2, but it did not explain why higher NEM related to worse d-prime. That separates general visual-attentional engagement from the frontal control pathway.
Can this EEG result predict who will develop PTSD or depression?
Not from this paper. The sample was assessed before Basic Combat Training, but the reported analysis did not test later disorder onset.
The result is a plausible vulnerability mechanism, not a validated prospective psychiatric-risk test.
Does lower FMT mean high-NEM people have poor self-control?
No. The result concerns a group-level EEG pathway during a lab task.
It supports the narrower claim that higher NEM was linked to weaker task-evoked frontal control signaling and worse discrimination in this sample.
References
- Teich CD, Rawls E, Stevens KL, Kang SSS, Davenport ND, Sponheim SR, Polusny MA, Marquardt CA. Neural mechanisms of negative emotionality and cognitive control: The role of frontal midline theta. Cognitive, Affective, & Behavioral Neuroscience. 2026. doi:10.3758/s13415-026-01434-0
- Cavanagh JF, Frank MJ. Frontal theta as a mechanism for cognitive control. Trends in Cognitive Sciences. 2014;18(8):414-421. doi:10.1016/j.tics.2014.04.012
- Cavanagh JF, Shackman AJ. Frontal midline theta reflects anxiety and cognitive control: Meta-analytic evidence. Journal de Physiologie-Paris. 2015;109(1-3):3-15. doi:10.1016/j.jphysparis.2014.04.003
- Buzzell GA, Troller-Renfree SV, Wade M, Debnath R, Morales S, Bowers ME, Fox NA. Adolescent cognitive control and mediofrontal theta oscillations are disrupted by neglect: Associations with transdiagnostic risk for psychopathology in a randomized controlled trial. Developmental Cognitive Neuroscience. 2020;43:100777. doi:10.1016/j.dcn.2020.100777
- White SF, Costanzo ME, Thornton LC, Mobley AM, Blair JR, Roy MJ. Increased cognitive control and reduced emotional interference is associated with reduced PTSD symptom severity in a trauma-exposed sample: A preliminary longitudinal study. Psychiatry Research: Neuroimaging. 2018;278:7-12. doi:10.1016/j.pscychresns.2018.06.006
- McTeague LM, Huemer J, Carreon DM, Jiang Y, Eickhoff SB, Etkin A. Identification of common neural circuit disruptions in cognitive control across psychiatric disorders. American Journal of Psychiatry. 2017;174(7):676-685. doi:10.1176/appi.ajp.2017.16040400
- Patrick CJ, Curtin JJ, Tellegen A. Development and validation of a brief form of the Multidimensional Personality Questionnaire. Psychological Assessment. 2002;14(2):150-163. doi:10.1037/1040-3590.14.2.150
- Messel MS, Raud L, Hoff PK, Stubberud J, Huster RJ. Frontal-midline theta reflects different mechanisms associated with proactive and reactive control of inhibition. NeuroImage. 2021;241:118400. doi:10.1016/j.neuroimage.2021.118400