
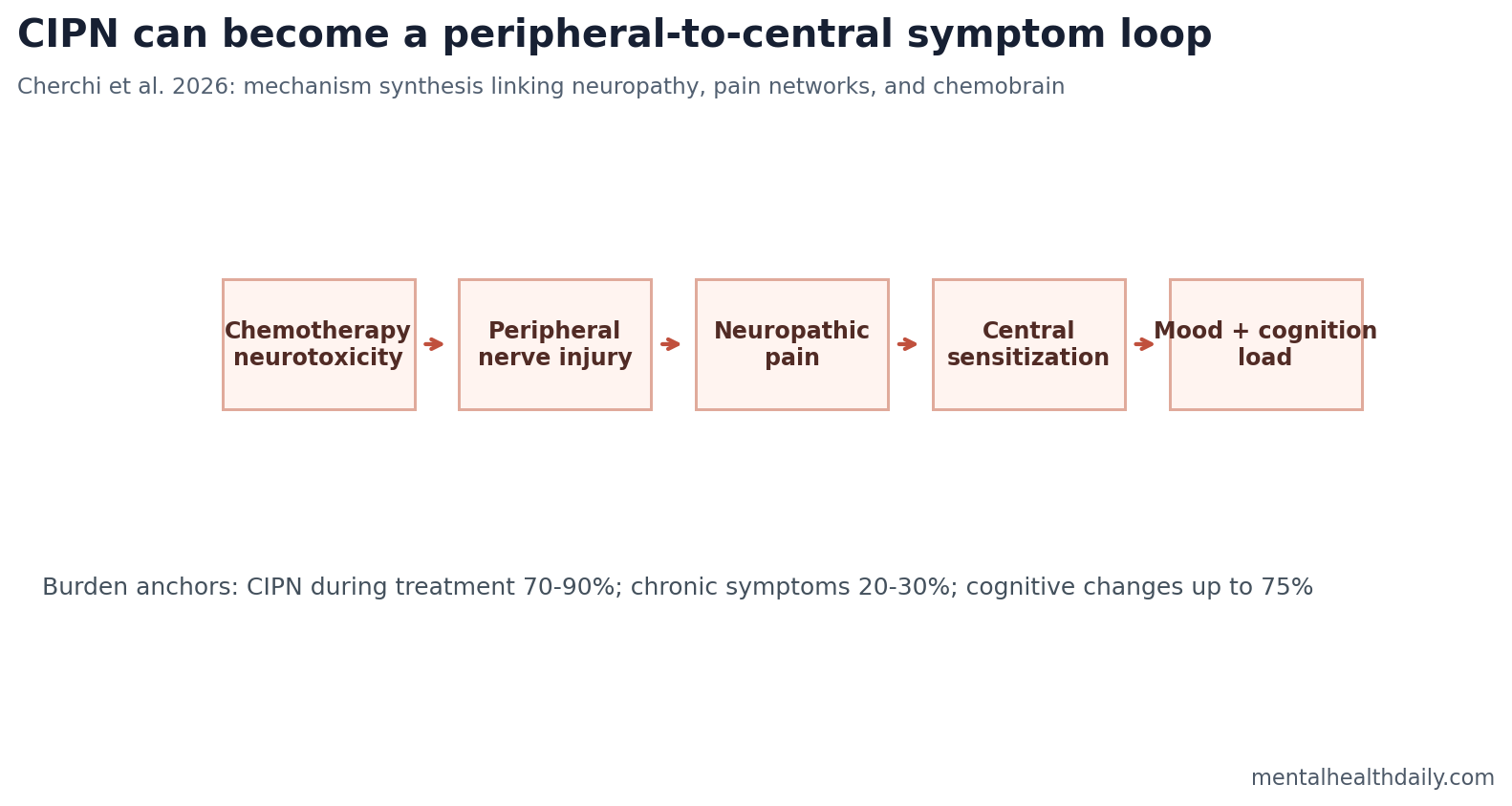
A 2026 neuroscience review argues that chemotherapy-induced peripheral neurotoxicity should not be treated as a purely peripheral nerve problem: CIPN affects 70-90% of patients during chemotherapy, persists chronically in 20-30% of survivors, and may interact with central sensitization, pain networks, mood, sleep, and chemobrain.1 The strongest claim is mechanistic connection, not proof that neuropathy alone causes every cognitive symptom after cancer treatment.
Research Highlights
- CIPN is common during treatment: Cherchi et al. summarize chemotherapy-induced peripheral neurotoxicity as affecting 70-90% of patients during chemotherapy.1
- Chronic symptoms persist in survivors: The review cites persistent chronic CIPN in 20-30% of survivors, making this a survivorship problem rather than only an acute toxicity.1
- Cognition can also be affected: Chemotherapy-related cognitive changes may affect up to 75% of treated patients, with variable persistence for years.1
- Taxanes are high-risk pain drugs: Taxane-related neuropathic pain can occur in 70-80% of treated patients in the review’s summary.1
- Duloxetine remains the clearest drug option: Clinical treatment evidence is strongest for duloxetine, while gabapentinoids, tricyclics, opioids, and topical agents remain mixed or limited.1,2
Chemotherapy-induced peripheral neurotoxicity (CIPN) means nerve damage caused by chemotherapy drugs, often producing numbness, tingling, burning pain, cold sensitivity, weakness, or balance problems. It is usually discussed as a peripheral side effect because the first injury is in nerves outside the brain and spinal cord.
Chemobrain is the common patient term for cancer-related cognitive impairment: slowed thinking, poor concentration, word-finding difficulty, memory complaints, and mental fatigue during or after cancer treatment. Cherchi et al. connect these 2 topics by emphasizing that persistent peripheral pain can remodel central pain and attention networks.
CIPN Is Peripheral Injury With Central Consequences
CIPN begins with chemotherapy effects on peripheral nerves. Platinum drugs, taxanes, vinca alkaloids, proteasome inhibitors, and related agents can injure axons, mitochondria, ion channels, dorsal-root ganglia, or microtubule systems. Different drugs produce different sensory patterns and time courses.1
Central sensitization means the brain and spinal cord become more responsive to pain input after repeated or intense signals. In that state, pain can persist after the original injury, spread beyond the initial site, or feel amplified compared with the measurable peripheral damage.
The review’s core model is therefore a chain, not a single lesion: chemotherapy injures peripheral nerves, persistent pain input changes spinal and brain processing, and those central changes can interact with sleep, mood, fatigue, attention, and cognition.
Pain Networks Overlap With Attention and Emotion Networks
Cherchi et al. point to the thalamus, anterior cingulate cortex, prefrontal cortex, insula, amygdala, periaqueductal gray, rostral ventromedial medulla, and descending pain modulation systems as plausible nodes in the CIPN-to-central-symptom pathway.1
Descending pain modulation is the brain’s top-down control over spinal pain processing. It can dampen pain signals, but it can also fail or become maladaptive. When descending control is impaired, peripheral nerve injury may feel larger, last longer, and become more emotionally and cognitively costly.
Those brain regions are not pain-only switches. The anterior cingulate and insula participate in salience and interoception, the prefrontal cortex supports control and working memory, and the amygdala helps assign threat value. That overlap explains why chronic pain, fatigue, anxiety, sleep disruption, and cognitive complaints often cluster in survivorship.
Chemobrain Has Multiple Chemotherapy and Survivorship Drivers
Cancer-related cognitive impairment has many possible contributors: chemotherapy, inflammation, hormonal treatment, anemia, sleep disruption, depression, anxiety, pain, cancer biology, menopause, steroids, and cognitive load from treatment itself. Ahles and Root emphasized that chemobrain is best understood as a multifactorial syndrome rather than a single drug lesion.3
The Cherchi review adds a useful bridge: CIPN and chronic neuropathic pain may be one route into the same central systems that support attention and emotional regulation. Pain and cognition therefore deserve joint assessment instead of fully separate survivorship silos.
Seretny et al. estimated that CIPN prevalence declines after treatment but remains clinically important months later, supporting the survivorship framing.4 A patient whose neuropathy persists after chemotherapy may also carry sleep loss, fear of movement, reduced activity, and attention drain from chronic pain.
That does not make neuropathy the master explanation for every cognitive complaint. It makes neuropathy a measurable pressure point inside a larger survivorship system. If cognitive symptoms rise only when pain, insomnia, or fatigue worsens, pain-network treatment may be clinically relevant. If cognition declines independent of neuropathy, clinicians should keep looking for anemia, endocrine treatment effects, depression, medication burden, cancer recurrence, neurodegenerative disease, or ordinary age-related cognitive change.
Treatment Evidence Is Narrower Than the Mechanism
Duloxetine has the clearest pharmacologic support for painful CIPN. Loprinzi et al. and guideline-style reviews have repeatedly found that many intuitive pain drugs have weaker or inconsistent evidence in this setting.2
Duloxetine is a serotonin-norepinephrine reuptake inhibitor used for depression, anxiety, and several pain conditions. In CIPN, the rationale includes descending pain modulation because norepinephrine and serotonin systems help regulate top-down pain control.
Gabapentinoids, tricyclic antidepressants, opioids, topical agents, exercise, rehabilitation, and neuromodulation may help selected patients, but the evidence varies by endpoint and population. A mechanistic model should not be mistaken for a permission slip to prescribe every neuropathic-pain drug for every chemotherapy survivor.
What This Review Can and Cannot Support
Supported: CIPN is common, can persist, and plausibly involves central nervous system remodeling when neuropathic pain becomes chronic. Pain, sleep, mood, fatigue, and cognition can interact through shared brain networks.
Not supported: a new incidence estimate, a single cause of chemobrain, or a claim that treating neuropathy automatically fixes cognition. The paper is a narrative/mechanistic review, so it synthesizes evidence rather than adding a new patient cohort.
Best clinical implication: survivorship care should ask about neuropathy, pain interference, sleep, mood, fatigue, and cognition together. Treating them as disconnected complaints risks missing the central amplification loop that keeps symptoms alive.
Assessment Should Combine Nerve Symptoms, Pain Interference, and Cognition
A narrow neuropathy checklist can miss the survivorship pattern that patients actually experience. Numbness and tingling matter, but so do burning pain, balance problems, sleep fragmentation, fear of walking, reduced activity, mood symptoms, and cognitive effort. Central sensitization is most clinically visible when the symptom network becomes self-reinforcing.
Minimum assessment bundle: sensory symptoms, neuropathic pain intensity, pain interference, falls or near-falls, sleep quality, fatigue, depression/anxiety symptoms, concentration, memory complaints, and daily function. That bundle does not assume one cause. It gives clinicians and researchers enough structure to see whether pain and cognition move together.
Mechanism-aware interpretation: cognitive complaints after chemotherapy may worsen when pain disrupts sleep, when neuropathy reduces activity, or when fear of symptom flare keeps the nervous system in a threat state. Treating pain, sleep, mood, and movement separately may still help, but the plan should recognize that each domain can feed the others.
Drug-Class Differences Should Shape Monitoring
Cherchi et al. emphasize that chemotherapy drugs do not all injure the nervous system in the same way. Taxanes, platinum drugs, vinca alkaloids, proteasome inhibitors, and other agents can produce different sensory profiles, timing, and reversibility patterns.1
That means monitoring should be drug-specific. A patient receiving a high-risk neurotoxic regimen may need earlier symptom screening, dose-toxicity discussion, and rehabilitation planning than a patient receiving a lower-risk regimen. Taxane-related neuropathic pain rates of 70-80% in the review’s summary are not interchangeable with every chemotherapy exposure.
Drug-specific monitoring also protects cognition research from a common error. If a study groups all chemotherapy exposures together, it may hide the pathways most likely to connect nerve injury, pain, inflammation, sleep, and cognition. Better phenotyping makes the central-sensitization model easier to test.
Rehabilitation endpoints: a trial that measures only pain intensity may miss gains in walking confidence, sleep, concentration, or daily activity. A trial that measures only cognition may miss the pain and sensory drivers that keep the cognitive complaint active. The central pathway model argues for combined endpoints.
That combined approach also helps patients describe symptoms without having to choose one label. A survivor may report “neuropathy,” “fatigue,” and “brain fog” as separate complaints, while the nervous system is processing them through overlapping pain, sleep, attention, and threat circuits.
Clinically, that means a better visit asks how symptoms interact across the day and whether each symptom exists in isolation.
It also changes trial design. Studies that enroll all chemotherapy survivors as one group may miss the subgroup with persistent neuropathic pain, poor sleep, and cognitive load. Enriching for that phenotype would test the review’s mechanism more directly than treating chemobrain as a uniform aftereffect.
Questions About CIPN, Pain, and Chemobrain
Does chemotherapy neuropathy cause chemobrain?
Not by itself. The review argues for plausible shared pathways and symptom interaction, not a one-cause explanation for all cognitive problems after cancer treatment.
Why would nerve pain affect cognition?
Persistent pain competes for attention, disrupts sleep, increases stress arousal, and recruits brain networks that also support salience, control, and emotion regulation.
Is duloxetine a cure for CIPN?
No. Duloxetine has the clearest drug evidence for painful CIPN, but responses vary and it does not reverse all nerve injury or cognitive symptoms.
What should patients track?
Track numbness, burning pain, balance, sleep, fatigue, mood, concentration, and daily function. The pattern across symptoms is often more informative than a pain score alone.
References
- Cherchi F, et al. From peripheral neurotoxicity to central sensitization: chemotherapy-induced peripheral neuropathy, pain and chemobrain. Reviews in the Neurosciences. 2026. doi:10.1515/revneuro-2025-0146
- Loprinzi CL, Lacchetti C, Bleeker J, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers: ASCO guideline update. Journal of Clinical Oncology. 2020. doi:10.1200/jco.20.01399
- Ahles TA, Root JC. Cognitive effects of cancer and cancer treatments. Annual Review of Clinical Psychology. 2018. doi:10.1146/annurev-clinpsy-050817-084903
- Seretny M, Currie GL, Sena ES, et al. Incidence, prevalence, and predictors of chemotherapy-induced peripheral neuropathy. Pain. 2014. doi:10.1016/j.pain.2014.09.020