A 2026 review argued that G protein-coupled receptor 30 may connect estrogen signaling, trigeminal pain pathways, and migraine biology, but migraine-specific human trials of GPR30-targeted drugs are still missing.
Research Highlights
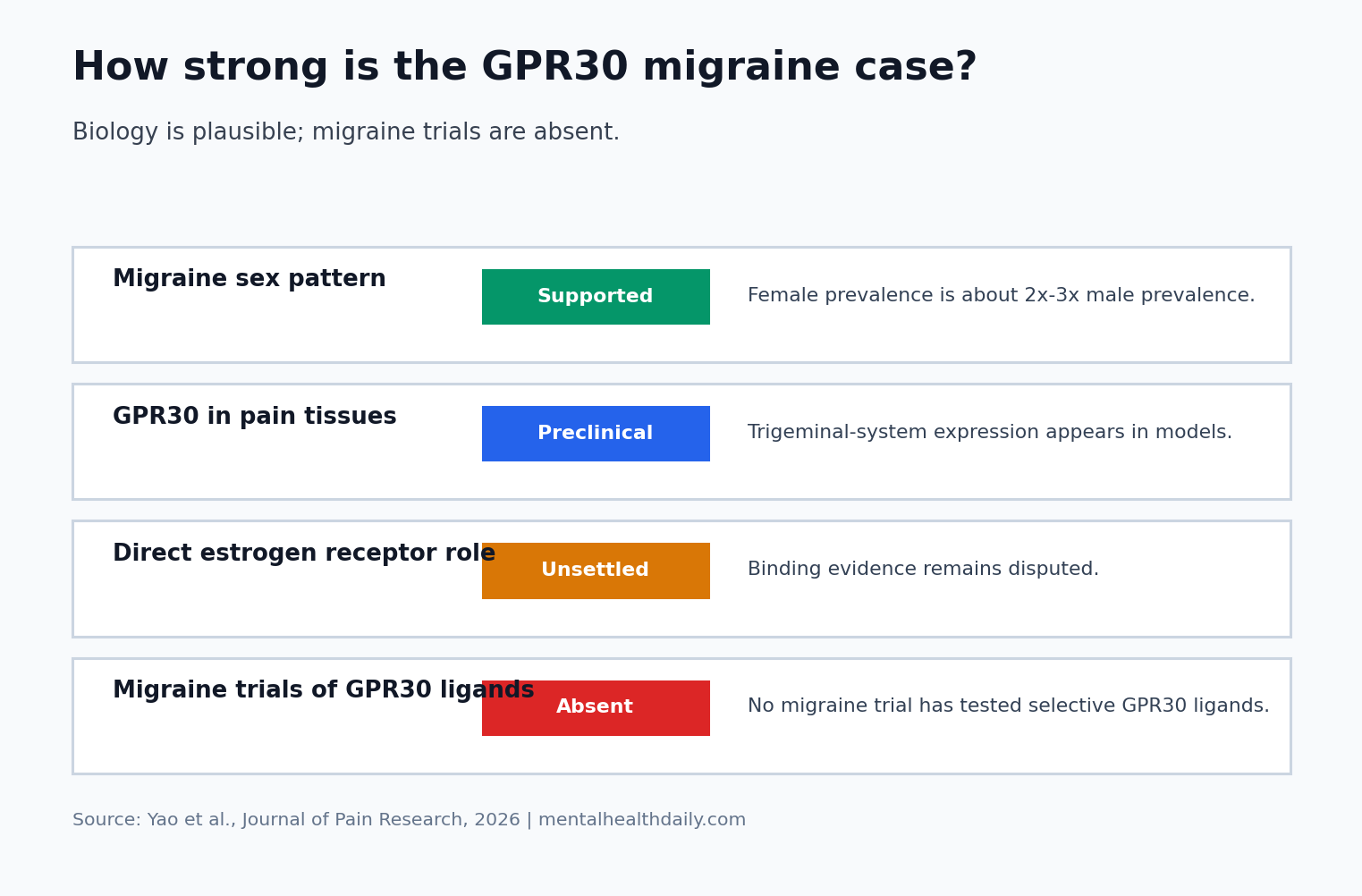
- The migraine rationale is hormone-linked: women have roughly 2 to 3 times the migraine prevalence of men, and 50% to 60% of women with migraine report attacks related to menstruation.
- GPR30 sits near relevant pain circuitry: preclinical work has reported GPR30 expression in the trigeminal ganglion and trigeminal spinal nucleus, structures that transmit head and face pain.
- The receptor biology is unsettled: GPR30 was once treated as a membrane estrogen receptor, but direct estrogen binding remains controversial.
- The clinical evidence is indirect: no migraine-specific human trial has tested a selective GPR30 ligand such as G-1.
G protein-coupled receptor 30, often called GPR30 or GPER, is a 7-transmembrane receptor encoded on chromosome 7p22.3. A 7-transmembrane receptor crosses the cell membrane 7 times and can trigger intracellular signaling when activated.
GPR30 has been discussed as a rapid estrogen-signaling receptor because it can influence cell pathways faster than classic nuclear estrogen receptors.
Migraine is a recurrent brain and trigeminal-pain disorder involving attacks of headache, light sensitivity, sound sensitivity, nausea, and sensory amplification. The trigeminal ganglion is a nerve-cell cluster that carries pain and sensory signals from the face, meninges, and cranial blood vessels. The trigeminal spinal nucleus receives those signals in the brainstem and upper cervical cord, making the trigeminal system central to migraine pain transmission.
Why Estrogen Biology Keeps Appearing in Migraine Research
The sex pattern in migraine is too large to ignore. Yao et al. summarized the female-to-male prevalence ratio as roughly 2:1 to 3:1, and 50% to 60% of women with migraine have menstrually related migraine. Menstrually related migraine means attacks cluster around estrogen withdrawal in the late luteal phase or early menstruation window.
Estrogen-linked systems: estrogen can affect vascular tone, cortical excitability, inflammation, serotonin signaling, calcitonin gene-related peptide release, and trigeminal neuron excitability.
Calcitonin gene-related peptide, or CGRP, is a neuropeptide released by trigeminal nerves that can dilate blood vessels, sensitize pain pathways, and trigger migraine biology. CGRP-blocking antibodies and small-molecule antagonists already have clinical roles in migraine prevention and acute treatment.
GPR30 enters this landscape because it may provide a membrane-linked route through which estrogen-related signals influence trigeminal pain. That is a plausible mechanism, but plausibility is not the same as a proven treatment target.
Study Snapshot
- Article type: narrative review of GPR30 in migraine pathophysiology.
- Main evidence base: receptor biology, animal studies, trigeminal-system experiments, estrogen-signaling literature, and indirect clinical observations.
- Central claim: GPR30 could connect estrogen changes with migraine-relevant trigeminal inflammation and sensitization.
- Main clinical gap: no selective GPR30 drug has been tested in a migraine-specific human trial.
GPR30 Could Affect Migraine Through Trigeminal Sensitization
Sensitization: a pain pathway becomes easier to activate and more likely to amplify ordinary signals. In migraine, trigeminal sensitization can help explain throbbing pain, scalp tenderness, light sensitivity, and attack persistence after the initial trigger has passed.
Cell signaling: Yao et al. described several pathways through which GPR30 could influence trigeminal excitability. These included phospholipase C-protein kinase C signaling, cyclic adenosine monophosphate-protein kinase A signaling, phosphoinositide 3-kinase/Akt signaling, mitogen-activated protein kinase/extracellular signal-regulated kinase signaling, and β-arrestin pathways. Receptor activation through these systems can change ion-channel behavior, inflammatory signaling, and peptide release in pain neurons.
Ion channels: the review linked GPR30 to transient receptor potential vanilloid 1, or TRPV1, a heat- and irritant-sensitive ion channel involved in burning pain and neurogenic inflammation. It also discussed sodium channels Nav1.7 and Nav1.8, which help pain neurons fire electrical signals. If GPR30 changes these channels in trigeminal neurons, estrogen-linked receptor signaling could alter how easily migraine pain circuits activate.
Neuropeptides and cytokines: CGRP and substance P can promote inflammation and pain transmission in the trigeminal system. The review described GPR30 as a possible upstream regulator of those migraine-relevant mediators, while also emphasizing inflammatory cytokines such as tumor necrosis factor-α, interleukin-1β, and interleukin-10.
The Direct Estrogen-Receptor Claim Is Still Unsettled
GPR30 has often been described as a membrane estrogen receptor because 17β-estradiol and synthetic ligands such as G-1 can activate GPR30-linked signaling in some experimental systems. Tamoxifen, raloxifene, curcumin, selective estrogen receptor modulators, and selective estrogen receptor degraders have also been discussed in relation to GPR30.
The strongest version of the treatment hypothesis would require a direct chain: estrogen binds GPR30, GPR30 activates trigeminal pain pathways, and a GPR30 drug reduces menstrual migraine. The available evidence supports a more cautious sequence:
- Estrogen fluctuation is strongly linked to migraine timing in many women: that epidemiologic and clinical pattern is real.
- GPR30 can influence pain and inflammatory signaling in experimental systems: that makes the receptor mechanistically relevant.
- Direct estrogen binding to GPR30 is disputed: structural and pharmacologic work has not produced a settled receptor-ligand mechanism.
- Migraine trials are absent: no selective GPR30 ligand has shown that modifying this receptor reduces migraine frequency, intensity, or acute medication use in patients.
An unsettled receptor mechanism can still be scientifically productive. GPR30 remains a candidate node in estrogen-linked migraine biology, while the clinical claim has to wait for direct migraine experiments.
Indirect Clinical Clues Do Not Prove a GPR30 Treatment Effect
Hormone-linked clues: estrogen stabilization can reduce migraine attacks in some hormonally sensitive patients, especially when attacks track estrogen withdrawal. Raloxifene studies in endometriosis monitored migraine as a secondary adverse event and reported changes in the proportion of patients with migraine in the overall population.
Attribution limit: raloxifene affects estrogen receptor α, estrogen receptor β, and GPR30-linked pathways, and endometriosis trials were not designed as migraine treatment trials. A secondary adverse-event or symptom observation can generate a hypothesis about migraine biology, but it cannot show that GPR30 caused the migraine change.
Evidence-strength note: this 2026 review is useful for mapping mechanisms and identifying testable hypotheses. It cannot establish GPR30 as a validated migraine drug target because the evidence is mostly preclinical, indirect, and mechanistically disputed at the receptor-binding level.
What Would Make GPR30 Clinically Relevant for Migraine?
Drug requirements: a credible migraine program would need selective GPR30 tools that reach relevant tissues, have acceptable safety, and can distinguish GPR30 effects from classic estrogen receptor effects. The review noted practical barriers: tool compounds can have low bioavailability, poor tissue selectivity, rapid metabolism, and uncertain long-term safety.
Trial endpoints: a prevention trial should measure monthly migraine days, monthly headache days, acute medication days, attack intensity, disability, adverse events, and menstrual-cycle timing when relevant. A mechanistic trial could measure CGRP-related changes, trigeminal sensitivity, or imaging markers, but symptom endpoints would still be needed before clinical use.
Patient selection: a receptor tied to estrogen-linked pathways may be most relevant in menstrual migraine, perimenstrual attack clustering, perimenopausal migraine worsening, or migraine phenotypes with strong hormonal fluctuation sensitivity. Testing GPR30 modulation in an unselected migraine population could dilute a real effect limited to a hormonal subgroup.
Comparator choice: the first clinically useful test would not be “does a GPR30 ligand change a laboratory marker?” It would be whether GPR30 modulation adds anything beyond existing migraine prevention, acute medication access, and hormonal-pattern management. A small mechanistic study could justify the biology, but a treatment claim would need randomized evidence against placebo or usual care, prespecified menstrual-cycle strata, and enough follow-up to show whether attack reduction persists across several cycles.
Safety threshold: estrogen-linked biology also raises a higher safety bar than an ordinary receptor-screening story. A migraine drug aimed at GPR30 would need monitoring for vascular effects, reproductive-hormone effects, mood or sleep changes, and off-target signaling in tissues where GPR30 has been discussed outside migraine.
That does not make the target unusable. It means the human program has to be designed as a hormone-linked migraine trial with pain endpoints, cycle timing, and safety monitoring built into the same protocol.
GPR30 Is a Hypothesis, Not a Migraine Treatment Target
- Strongest claim: GPR30 belongs on the migraine research map because it can connect estrogen-linked signaling with trigeminal pain, inflammation, ion channels, and neuropeptides.
- Weakest claim: selective GPR30 drugs are ready for migraine prevention. No migraine-specific human trial supports that step.
- Most relevant patient question: people with menstrual migraine should not treat GPR30 supplements, phytoestrogens, or experimental ligands as proven migraine therapies.
- Best research direction: subtype-specific human studies should test whether GPR30-related biology predicts menstrual migraine patterns or response to targeted intervention.
GPR30 may help explain how estrogen-linked biology reaches trigeminal pain circuits, but the receptor needs direct human migraine evidence before it can guide prescribing.
Questions About GPR30 and Migraine
What role did the 2026 review assign to GPR30?
GPR30, also called GPER, is a membrane receptor that can trigger rapid intracellular signaling. It has been studied as a possible estrogen-linked receptor, but direct estrogen binding remains debated.
Why would GPR30 matter for migraine?
GPR30 may influence trigeminal pain signaling, inflammatory cytokines, CGRP, substance P, TRPV1 channels, and sodium channels involved in pain-neuron firing. These pathways are relevant to migraine attacks.
Are there GPR30 drugs for migraine?
No GPR30-targeted drug is approved for migraine, and no migraine-specific human trial has shown that a selective GPR30 ligand reduces migraine frequency or severity.
Does this explain menstrual migraine?
It may contribute to a research explanation, but it does not fully explain menstrual migraine. Estrogen withdrawal, CGRP biology, serotonin signaling, cortical excitability, sleep, stress, and individual susceptibility can all change migraine risk around menstruation.
References
- Yao H, Liu Y, Hao S, et al. Potential roles of G protein-coupled receptor 30 (GPR30) in migraine pathophysiology. Journal of Pain Research. 2026;19:1863–1875. https://doi.org/10.2147/jpr.s594943
- Edvinsson L. The CGRP pathway in migraine as a viable target for therapies. Headache. 2018;58 Suppl 1:33–47. https://doi.org/10.1111/head.13305
- Pavlovic JM, Akcali D, Bolay H, Bernstein C, Maleki N. Sex-related influences in migraine. Journal of Neuroscience Research. 2017;95(1–2):587–593. https://doi.org/10.1002/jnr.23903
- Revankar CM, Cimino DF, Sklar LA, Arterburn JB, Prossnitz ER. A transmembrane intracellular estrogen receptor mediates rapid cell signaling. Science. 2005;307(5715):1625–1630. https://doi.org/10.1126/science.1106943
- Benemei S, Nicoletti P, Capone JG, Geppetti P. CGRP receptors in the control of pain and inflammation. Current Opinion in Pharmacology. 2009;9(1):9–14. https://doi.org/10.1016/j.coph.2008.12.007