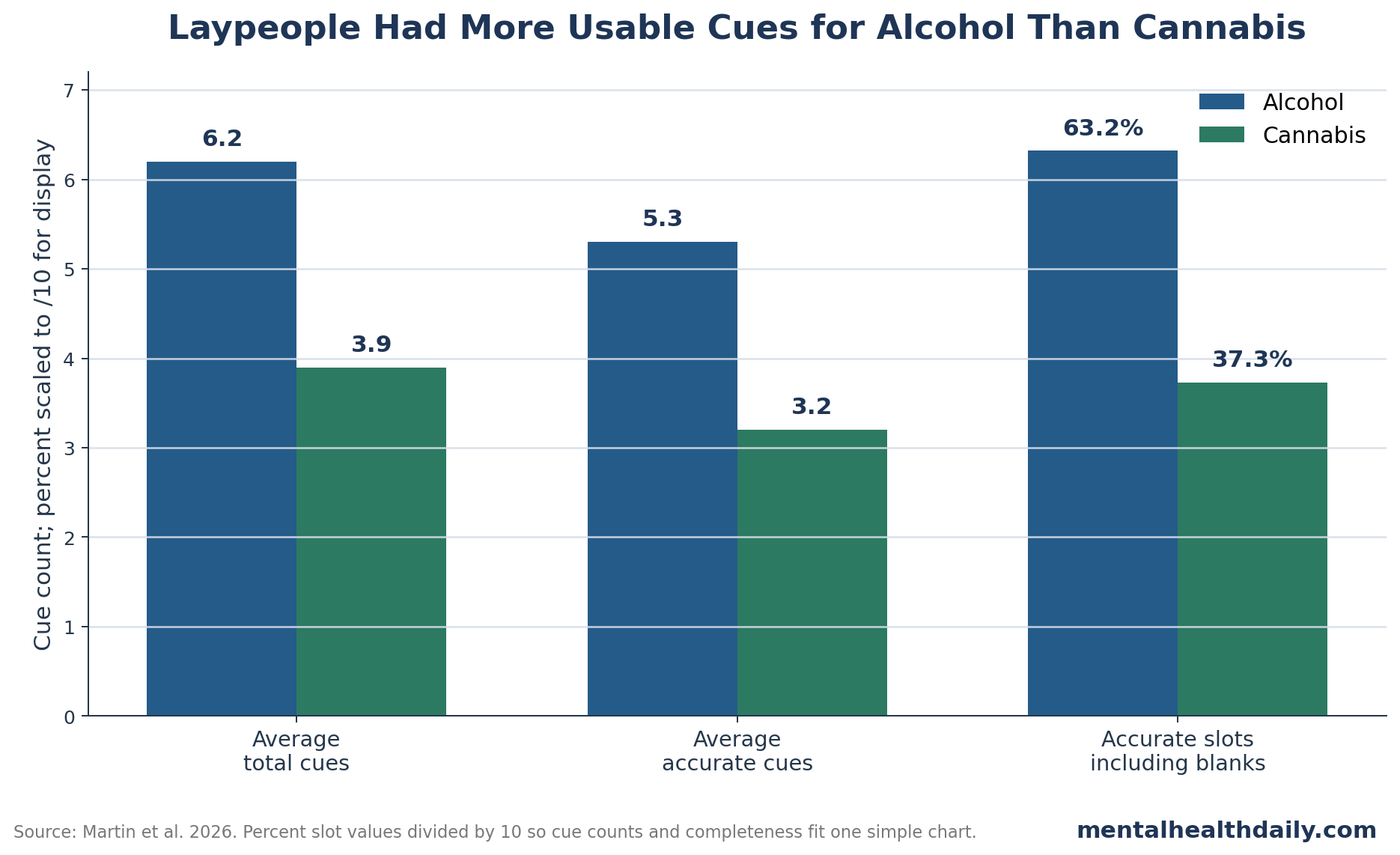
A 2026 survey of 467 University of Sydney undergraduate psychology students found that participants generated more and more accurate observable cues for alcohol intoxication than for cannabis intoxication.1 When unanswered cue fields were counted, accurate alcohol cues appeared in 63.2% of possible response slots, while accurate cannabis cues appeared in 37.3%.
Research Highlights
- Alcohol cues were easier to name: participants listed an average of 6.2 alcohol cues compared with 3.9 cannabis cues.
- Alcohol cue accuracy was higher: participants averaged 5.3 accurate alcohol cues compared with 3.2 accurate cannabis cues.
- Blank cannabis fields were common: 56.3% of cannabis cue fields were left unanswered, compared with 31.3% of alcohol cue fields.
- Cannabis experience had only a small link: less-than-monthly and monthly cannabis users provided slightly more accurate cannabis cues than never-users among 467 students.
- Evidence strength is perceptual: the 2026 study measured what students could report, not whether they could correctly classify intoxication in real-world encounters.
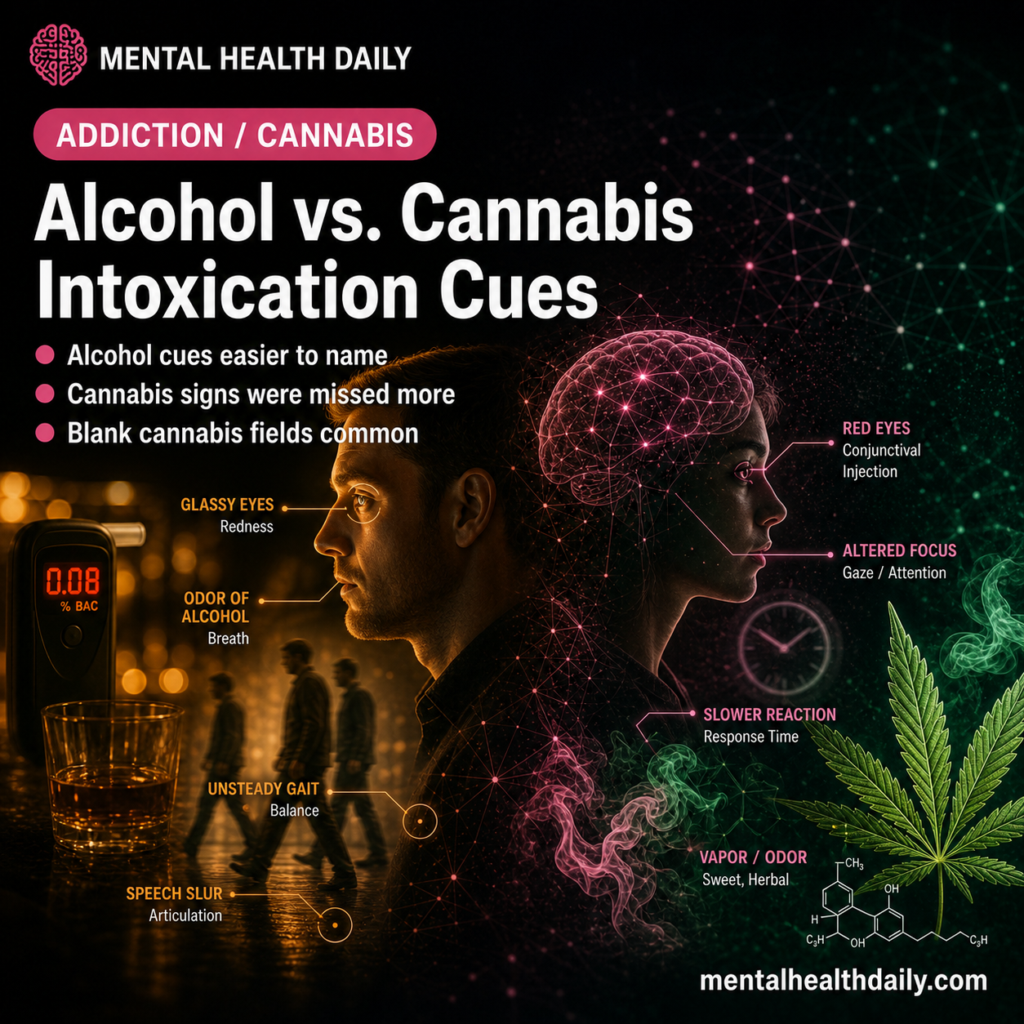
Observable intoxication cues are visible or audible signs that another person may be impaired. These cues guide decisions in law enforcement, responsible alcohol service, workplace safety, driving, and bystander judgment.
Examples include: slurred speech, balance problems, red eyes, odor, slowed reaction, unusual laughter, impaired coordination, and altered attention.
Martin et al. analyzed open-text survey responses from 467 undergraduate psychology students.1 Participants were not testing other people in a laboratory. They were asked to list cues a layperson might use to detect alcohol and cannabis intoxication, and the study team coded those cues for accuracy based on prior literature.
Participants Named More Alcohol Cues Than Cannabis Cues
The sample was mostly female, 77.7%, and the average age was 20.5 years. Most participants had limited cannabis experience: 381 students, or 81.6%, reported never consuming cannabis. Alcohol exposure was more common. Among students with enough Alcohol Use Disorders Identification Test-Consumption data, 252 of 380, or 66.3%, were above the hazardous-drinking cutoff.
The cue-generation difference was large. Participants produced an average of 6.2 alcohol cues, standard deviation 1.5, compared with 3.9 cannabis cues, standard deviation 1.9. The paired comparison was statistically strong, t(466) = 24.26, p < 0.001.
The unanswered fields make the gap easier to understand:
- Alcohol cue fields left blank: 31.3%.
- Cannabis cue fields left blank: 56.3%.
- Alcohol responses coded after exclusions: 2,557 cues.
- Cannabis responses coded after exclusions: 1,627 cues.
Alcohol intoxication has a thick public script. People are taught to notice slurred speech, stumbling, loudness, poor coordination, and odor. Cannabis intoxication can involve red eyes, delayed reaction, altered attention, relaxation, anxiety, unusual laughter, appetite change, and coordination problems, but those signs are less culturally standardized and may be easier to confuse with fatigue, personality, anxiety, or baseline behavior.
Accuracy Was Higher for Alcohol Than Cannabis
Among coded responses, 95.7% of alcohol cues were accurate, 3.8% were partially accurate, and 0.6% were inaccurate. Among coded cannabis responses, 91.6% were accurate, 5.8% were partially accurate, and 2.6% were inaccurate.
Those coded-response percentages can be misleading if read alone because they exclude blanks. Including non-responses, accurate alcohol cues appeared in 63.2% of all possible cue slots, while accurate cannabis cues appeared in 37.3%. That version captures both correctness and availability: participants had lower cannabis accuracy and often had no cannabis cue to offer.
- Accurate alcohol cues: mean 5.3, standard deviation 1.8.
- Accurate cannabis cues: mean 3.2, standard deviation 1.8.
- Alcohol vs. cannabis accuracy comparison: t(466) = 21.53, p < 0.001.
- Association between alcohol and cannabis accuracy: r = 0.35, p < 0.001.
Correlation r describes how strongly 2 measures move together, from −1 to +1. The r = 0.35 result means students who named accurate alcohol cues tended to name more accurate cannabis cues too, but the relationship was moderate rather than interchangeable.
Cannabis Experience Had a Small Association With Cannabis Cue Accuracy
Model size: The regression model for cannabis cue accuracy was statistically significant, F(5,461) = 4.68, p < 0.001, but explained only 5% of variance. Variance explained, or R², describes how much of the difference between participants the model accounted for. Here, R² = 0.05 means most differences in cannabis cue accuracy were left unexplained.
Cannabis experience: Participants who used cannabis less than monthly had a 0.17 higher proportion of accurate cannabis cues than never-users. Monthly users had a 0.13 higher proportion than never-users. The study had very few weekly or daily cannabis users, so it could not provide a stable estimate for heavy-use groups.
Perceived difficulty: Perceived difficulty was more interpretable. Participants who rated cannabis intoxication as extremely difficult to detect provided fewer accurate cannabis cues than participants who rated cannabis detection as somewhat difficult, neutral, somewhat easy, or extremely easy. The difficulty effect was significant, F(4,435) = 9.94, p < 0.001, eta² = 0.08. Eta squared is an effect-size measure; 0.08 indicates a moderate share of explainable group difference in this context.
Real-World Detection Requires More Than Cue Lists
Alcohol and cannabis impairment do not map perfectly onto visible signs. Tolerance, dose, route of administration, time since use, co-use with alcohol or sedatives, sleep deprivation, and individual baseline behavior can all change appearance.23
Public-safety implication: training that works for alcohol cannot simply be copied onto cannabis. Alcohol training often relies on visible motor and speech cues. Cannabis detection may need scenario-based training, delayed-reaction tasks, divided-attention observation, questions about recent use, and clear rules for when uncertainty should trigger a safer decision.
Police and server-training research has long shown that judging intoxication from appearance is imperfect.45 Drug-recognition programs use structured signs, but laypeople rarely have that training. The 2026 study shows the first step in the problem: even before real-time judgment, people have fewer cannabis signs available in memory.
Evidence strength: this was a convenience survey and secondary analysis of open-text responses from undergraduate students. It can show what cues participants could name and how researchers coded those cues. It cannot prove that participants would detect intoxication accurately in bars, workplaces, roadsides, clinics, classrooms, or homes.
Training implication: the study separates 2 tasks that are often blurred. Recognition means noticing signs that should raise concern. Confirmation means determining whether someone is actually impaired enough for a legal, safety, or clinical decision. Laypeople may be able to recognize some alcohol signs while still being poor at confirmation, especially at low or moderate blood alcohol levels.
Alcohol recognition: common cues such as slurred speech, odor, poor balance, loudness, and slowed reaction are easy to remember, but they can miss quiet intoxication or overcall people with disability, fatigue, anxiety, or speech differences.
Cannabis recognition: red eyes, altered attention, slowed reaction, unusual laughter, anxiety, or impaired coordination can appear after cannabis use, but those signs are less specific. A tired student, an anxious patient, or a sleep-deprived worker can resemble parts of the cannabis cue list.
Decision rule: when the consequence is safety-critical, uncertainty should shift behavior toward risk reduction. That may mean not driving, pausing work with machinery, calling a sober ride, using a formal workplace process, or requesting trained assessment rather than relying on a friend's visual judgment.
Legalization and medical access can make cannabis seem socially ordinary, but ordinary use does not make impairment easy to judge. A product can be legal for adults and still produce reaction-time, attention, or coordination changes that are hard for bystanders to classify.
That distinction is especially important for mixed alcohol-cannabis situations. Alcohol cues may dominate attention because they are louder and more familiar, while cannabis-related slowing, divided-attention problems, or unusual anxiety may be missed. A safer training message is not “spot marijuana by one sign.” It is to treat uncertain impairment as a task-specific risk when driving, serving alcohol, supervising machinery, or making consent-sensitive decisions.
Questions About Alcohol and Cannabis Intoxication Cues
Did participants actually test intoxicated people?
No. Participants listed cues they believed laypeople could use. The study team coded those written cues for accuracy using prior evidence.
Which intoxication type was easier for participants?
Alcohol intoxication was easier. Participants listed more total alcohol cues, more accurate alcohol cues, and left fewer alcohol cue fields blank.
Why might cannabis intoxication be harder to identify?
Cannabis signs can be less socially standardized and more easily confused with fatigue, anxiety, personality, sleep loss, or ordinary distraction. Some signs also vary by dose, tolerance, and product type.
Can visible cues prove impairment?
No. Visible cues can raise suspicion, but impairment depends on dose, timing, tolerance, task demands, and co-use with other substances. A cue list is not a substitute for a validated impairment assessment.
What is the clearest takeaway for bystanders?
Bystanders should treat cue lists as warning signals, not courtroom proof. If someone may be impaired and the next action involves driving, medical consent, machinery, childcare, or conflict, the safer move is to reduce the task risk first and argue about certainty later.
References
- What Cues Do Laypeople Use to Detect Alcohol and Cannabis Intoxication? Martin TL et al. Drug and Alcohol Review. 2026. doi:10.1111/dar.70156
- The Health and Social Effects of Nonmedical Cannabis Use. Peacock A et al. Addiction. 2018;113(7):1202-1212. doi:10.1111/add.14234
- Acute Alcohol Toxicity. Vonghia L et al. European Journal of Internal Medicine. 2008;19(8):561-567. doi:10.1016/j.ejim.2007.06.033
- Police Officers' Identification of Breath Alcohol Levels in Drivers. Brick J et al. Alcoholism: Clinical and Experimental Research. 2001;25(6):850-855. doi:10.1111/j.1530-0277.2001.tb02290.x
- Can Servers Recognize Intoxicated Patrons? Burns ED et al. Journal of Studies on Alcohol. 1995;56(1):74-80. doi:10.2190/8U4B-U3VV-WBDN-UKEH
- The Accuracy of Laypeople's Judgments of Alcohol Intoxication. Monds LA et al. Drug and Alcohol Review. 2021;40(2):280-289. doi:10.1111/dar.13241
- Observable Signs of Drug Use and Impairment. Shinar D et al. Accident Analysis & Prevention. 2006;38(2):317-329. doi:10.1016/j.aap.2005.04.002
- A Review of the Validity of the Drug Evaluation and Classification Program. Beirness DJ et al. Traffic Injury Prevention. 2007;8(4):368-376. doi:10.1080/15389580701525651