
A 35-person EEG study found that pain empathy did not collapse when live two-way video was replaced by prerecorded viewing: observer-target pain-rating correlations were nearly identical during video calls and recordings, r = 0.65 vs. r = 0.64, both p < 0.001.1 The calibrated read is narrow but useful: temporal immediacy was not required for basic empathy-for-pain accuracy in this controlled task.
Research Highlights
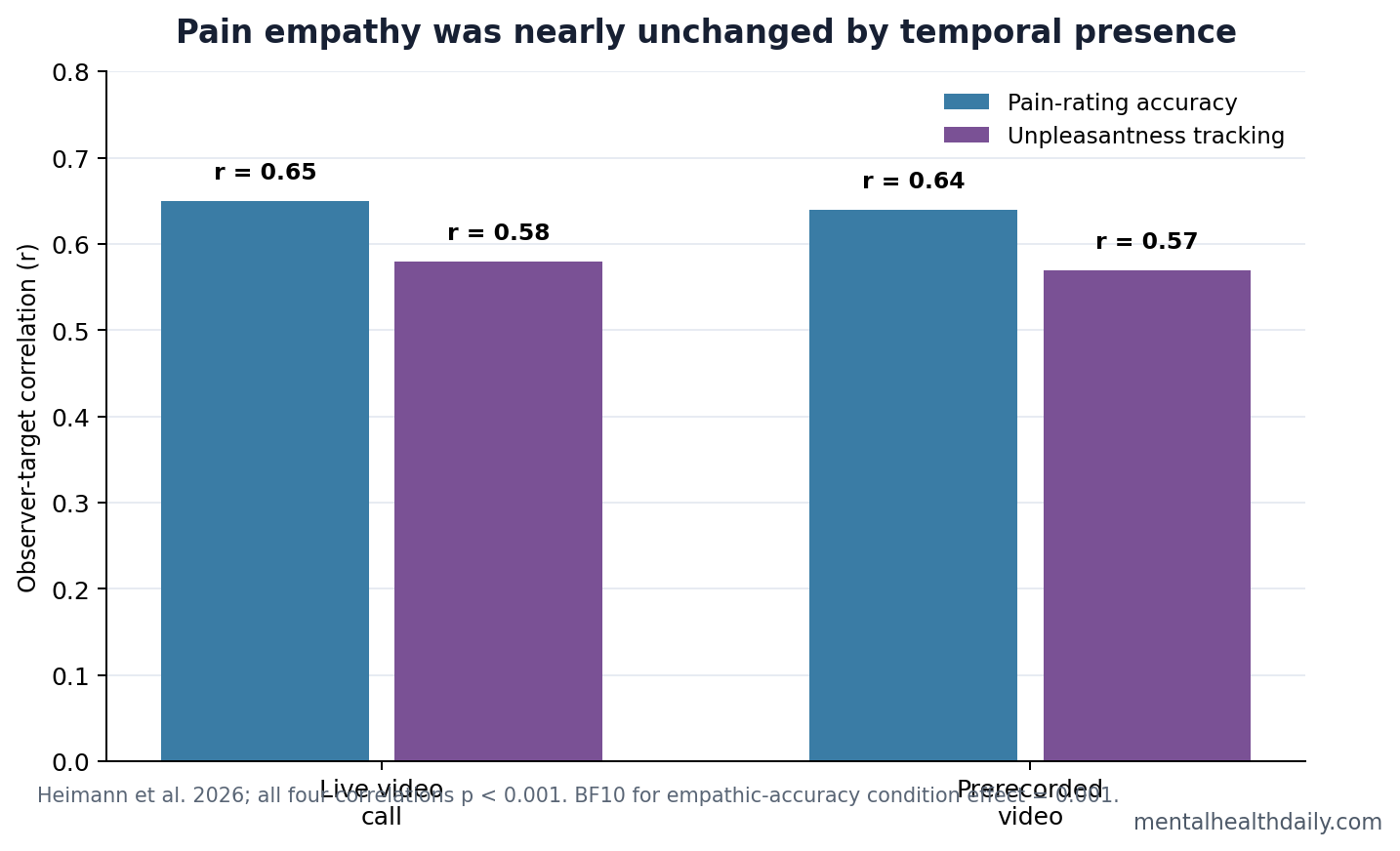
- Empathic accuracy was preserved: Observer and target pain ratings correlated at r = 0.65 during live video calls and r = 0.64 during prerecorded viewing, both p < 0.001.1
- The condition effect was essentially absent: A Bayes factor of BF10 = 0.001 gave extreme evidence for the empathic-accuracy model without video condition as a predictor.1
- Affective empathy also survived reduced immediacy: Unpleasantness ratings tracked target pain in video calls, r = 0.58, and prerecorded videos, r = 0.57, both p < 0.001.1
- Theta carried the pain signal: Observer midfrontal theta increased with the other person’s shock intensity, b = 0.12, p = 0.028, but temporal presence did not significantly modulate theta, mu, or beta power.1
- The task was narrow: The result applies to short 0-100 empathy-for-pain judgments in a 35-person healthy-adult experiment, not complex clinical rapport or long-term digital relationships.
Temporal presence means the immediacy of social information: a live video call has high temporal presence because both people can react in real time, while a prerecorded video has low temporal presence because the target cannot respond. Social-presence theories often predict that reduced immediacy should weaken social cognition.2
Empathy for pain is the ability to estimate and share another person’s pain while keeping self and other distinct. Heimann et al. separated a cognitive component, empathic accuracy, from an affective component, the observer’s own unpleasantness while watching someone else receive painful stimulation.1
31 Usable Observer Datasets Tested Live Video vs. Prerecorded Pain
Participants served as both target and observer across 2 laboratory sessions. Targets received calibrated electric shocks to the hand, while observers rated the target’s pain and their own unpleasantness on 0-100 visual analog scales. The main comparison was a live video-call condition vs. a prerecorded-video condition with the same pain task.1
- Behavioral data: 31 usable participants after exclusions and technical loss.
- EEG observation data: 31 usable participants for neural analyses.
- Skin conductance: 31 usable participants for electrodermal coupling.
- Heart-rate coupling: 32 usable participants for interbeat-interval analyses.
The pain calibration was comparable across the own-pain and video-call conditions. Upper calibration limits averaged 6.5 mA vs. 6.6 mA, t(33) = 0.38, p = 0.703, so the key comparison was not obviously driven by different shock intensity settings.1
Live Video Did Not Improve Pain-Reading Accuracy
Observer pain ratings were strongly predicted by target pain ratings. The video-call correlation was r = 0.65, and the prerecorded correlation was r = 0.64, both p < 0.001 after Bonferroni correction. Mean rating distance was also small on a 0-100 scale: 1.99 in the video-call condition and -1.57 in the prerecorded condition.1
Plain-English read: observers were similarly accurate whether the target was live and mutually visible or seen in a recording. The live condition may have felt more immediate, but it did not add measurable accuracy to this task.
Affective Empathy Was Also Similar Across Conditions
Observers’ unpleasantness ratings tracked target pain in both conditions, with correlations of r = 0.58 during video calls and r = 0.57 during prerecorded viewing. The main condition effect was statistically detectable in the model, p = 0.009, but the average difference was only 1.66 points on a 0-100 scale.1
Interpretation: live video may slightly raise the observer’s overall unpleasantness, but the effect was too small to carry much practical meaning in this experiment. The slope linking the target’s pain to the observer’s unpleasantness did not meaningfully depend on temporal presence.
The EEG Result Was a Theta Signal, Not a Live-Video Signal
Midfrontal theta is low-frequency electrical activity often linked to attention, salience, conflict, and pain-related monitoring. In Heimann et al., observer theta power increased with the target’s shock intensity, b = 0.12, p = 0.028.1
Mu rhythm is 8-12 Hz activity over sensorimotor cortex that is often discussed in action observation and pain-empathy work. Mu power did not show the expected pain-intensity modulation, and temporal presence did not significantly modulate mu, theta, or beta power. Bayes factors for the condition effect were extremely small: theta BF10 = 0.0005, mu BF10 = 0.0009, and beta BF10 = 0.0005.1
An exploratory timing result still mattered. Theta peaked earlier in the video-call condition, around 649 ms, than in the prerecorded condition, around 752 ms. That suggests temporal presence may shift timing even when it does not change overall empathic accuracy.
Pain-Empathy Studies Separate Accuracy From Social Immediacy
Singer et al. showed that observing another person in pain engages affective pain-related circuitry, helping establish empathy for pain as a measurable brain-and-behavior paradigm.3 Later reviews and meta-analyses emphasized that empathy for pain is not one process; it includes affective sharing, cognitive estimation, attention, and context.4
Petereit et al. previously tested physical presence in a related pain-empathy setup. Heimann et al. moved the question to temporal presence: whether live reciprocal timing matters when the social channel remains visual and video-mediated.2
Practical calibration: the study argues against a blanket claim that video or recorded observation makes people unable to read another person’s pain. It does not argue that all digital interaction is equivalent to in-person care, friendship, or therapy.
What the Study Can and Cannot Support
Supported: in healthy young adults, basic pain-empathy ratings and several EEG/physiology indices were largely independent of whether the target was seen live by video call or in a prerecorded clip.
Not supported: broad conclusions about remote psychotherapy, chronic pain caregiving, emotionally complex conversations, or empathy in people with social-cognitive disorders. The task was brief, controlled, and centered on visible pain reactions to calibrated electric stimulation.
Best next test: clinically relevant digital-empathy work should use richer interactions, patient populations, motivational outcomes, and longer time windows instead of assuming that pain-rating accuracy captures all of social connection.
The Bayesian result strengthens the narrow conclusion. A condition Bayes factor of BF10 = 0.001 meant the empathy-accuracy model gained extreme support without adding live-vs.-recorded condition as a predictor. In plain language, participants were reading visible pain intensity from the target, and live temporal reciprocity did not add detectable accuracy in this task.
The same result should not be stretched into a full telehealth verdict. Pain-rating accuracy is only one slice of empathy. Clinical encounters also depend on whether a patient trusts the listener, discloses relevant information, follows through with care, and feels understood over time. This experiment isolates a useful perceptual component: seeing another person’s pain response by video was enough for basic rating accuracy, even when the interaction was not live.
EEG interpretation: midfrontal theta tracked pain intensity, b = 0.12, p = 0.028, but the signal was not a live-video advantage. The brain response followed the observed pain cue more than the timing format.
For digital-care debates, this is a cleaner result than a vague “online empathy works” claim: visual pain information survived the shift from live to prerecorded video, while broader relational outcomes remain untested.
That distinction also matters for how the study should be used. The experiment supports remote observation for simple pain-reading accuracy, especially when facial and bodily reactions are visible.
It does not answer whether delayed, asynchronous, or low-bandwidth communication preserves empathy when the patient is describing invisible pain, fear, shame, or uncertainty. Those settings require language, trust, history, and visible nociceptive reactions.
Telehealth boundary: this experiment is most relevant to situations where a clinician, caregiver, or researcher can see pain behavior directly. It is less informative for chronic pain visits where facial expression may be muted, pain is described verbally, or the main clinical task is validating a symptom that has no visible signal.
The result still pushes against a lazy assumption that mediated contact automatically erases empathy. In this task, observers read another person’s pain about as accurately from recorded video as from live two-way video. The harder question is whether that perceptual accuracy turns into better care, comfort, or decisions in real clinical contexts.
Bottom line: temporal presence was not the active ingredient for this pain-rating task; visible pain behavior was.
Questions About Video Calls and Empathy
Does this mean prerecorded videos are as good as live interaction?
No. It means prerecorded viewing preserved pain-rating accuracy in this specific experiment. Live interaction can still matter for trust, reciprocity, disclosure, and motivation.
Why did the study measure EEG?
EEG gave millisecond-level timing information about neural responses while observers watched the target’s pain. That made it possible to test whether live video changed theta, mu, or beta activity during the pain event.
What did this mean for telehealth pain assessment?
The narrow takeaway is reassuring: a video-mediated format does not automatically erase a person’s ability to read visible pain. Telehealth quality still depends on the task, relationship, context, and clinical stakes.
References
- Heimann J, Petereit P, Perry A, Kramer UM. Empathy for pain persists across live two-way video interactions and viewing of prerecorded videos. Cognitive, Affective, & Behavioral Neuroscience. 2026. doi:10.3758/s13415-026-01442-0
- Petereit P, et al. Physical presence and empathy for pain. PubMed
- Singer T, Seymour B, O’Doherty J, Kaube H, Dolan RJ, Frith CD. Empathy for pain involves the affective but not sensory components of pain. Science. 2004. doi:10.1126/science.1093535
- Lamm C, Decety J, Singer T. Meta-analytic evidence for common and distinct neural networks associated with directly experienced pain and empathy for pain. PubMed
- Zaki J, Ochsner KN. The neuroscience of empathy: progress, pitfalls and promise. PubMed