A 913-person economic evaluation of the PReDicT antidepressant algorithm found nearly identical EQ-5D quality-of-life gains vs. treatment as usual (+0.139 vs. +0.140) and nearly identical societal cost reductions (−€2,589 vs. −€2,602), while cost-effectiveness probabilities were only 46% to 59% at trial level but exceeded 80% in the UK.1 The algorithm signal was country-specific and capability-weighted, not a clean QALY win.
Research Highlights
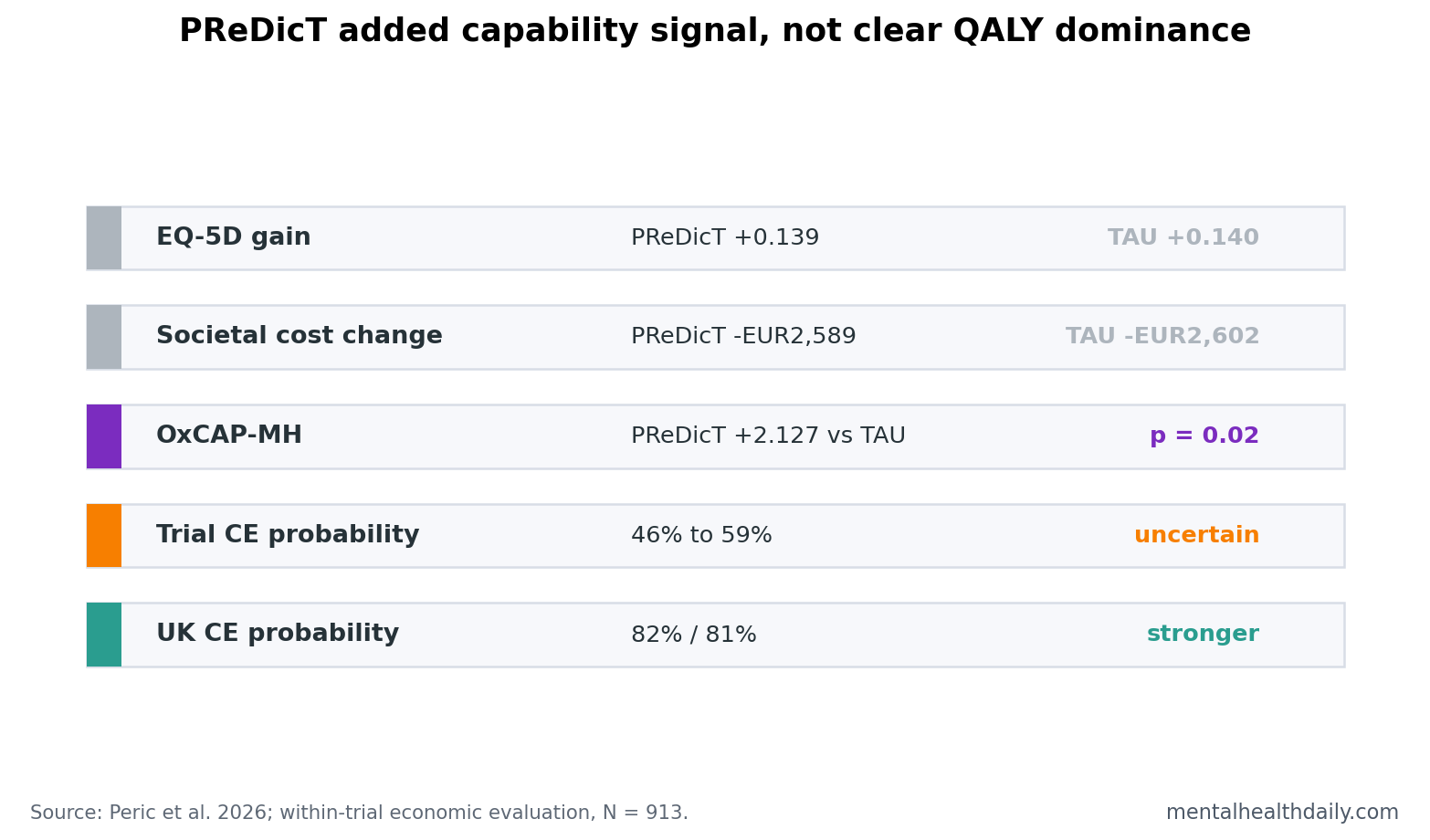
- Quality-of-life gains were nearly identical: EQ-5D-5L increased +0.139 in PReDicT and +0.140 in treatment as usual over 24 weeks.
- Societal costs fell in both arms: per-patient societal costs changed by −€2,589 with PReDicT and −€2,602 with usual care.
- Capability improved more in 2 countries: UK/Germany OxCAP-MH scores favored PReDicT by +2.127 points (95% CI 0.323 to 3.931; p = 0.02).
- Trial-level cost-effectiveness was uncertain: probabilities ranged from 46% to 59% depending on perspective and threshold.
- The UK subgroup exceeded trial-level probabilities: UK probabilities reached 82%, 81%, and 71% across healthcare, health/social care, and societal perspectives.
PReDicT is a digital antidepressant-treatment tool that uses early symptom change and affective-cognition testing to flag likely nonresponse after 1 week. The goal is to shorten the usual trial-and-error cycle by prompting earlier review, dose escalation, switching, or augmentation when early response looks poor.
QALYs, or quality-adjusted life-years, combine length of life and health-related quality of life into a single economic outcome. OxCAP-MH is a mental-health capability measure that captures broader functioning and well-being alongside health-state utility.
PReDicT Did Not Beat Usual Care on EQ-5D
The economic analysis was built alongside a multinational randomized trial in France, Germany, The Netherlands, Spain, and the UK.1 The health-economic sample included 460 people assigned to PReDicT and 453 assigned to usual care.
The main QALY finding is easy to overread unless the numbers are kept next to each other. EQ-5D-5L improved by +0.139 in the PReDicT group and +0.140 in the usual-care group. Both arms improved, and the algorithm did not create a visible EQ-5D separation.
That pattern fits the parent clinical trial. Browning et al. reported similar 8-week depression response rates, 55.9% with PReDicT vs. 51.8% with usual care, while anxiety and functioning favored PReDicT more clearly.2 The economic paper echoes that split: broad quality-of-life utility was flat between arms, but some secondary functioning signals moved.
Capability Gains Were the Strongest Positive Signal
The clearest added-benefit result came from OxCAP-MH, collected in the UK and Germany. PReDicT showed +2.127 points more capability improvement than usual care, with p = 0.02. The researchers described that as a 24% additional gain in the UK/Germany capability sample.
Capability well-being asks a different question than EQ-5D. It is closer to whether people can function, choose, participate, and live in ways they value. For depression treatment, that distinction can be meaningful because symptom reduction and life functioning do not always move together.
The economic interpretation remains mixed. A capability signal can be clinically relevant even when QALY separation is absent, but payers often make decisions around QALYs, thresholds, and budget impact. A result that looks stronger under OxCAP-MH than EQ-5D may be attractive for mental-health policy but harder to translate into standard reimbursement rules.
Cost-Effectiveness Split by Country and Perspective
At a tentative European willingness-to-pay threshold of €50,000 per QALY, PReDicT’s trial-level cost-effectiveness probability was 53% from the healthcare perspective, 53% from the health and social care perspective, and 59% from the societal perspective. Those are not strong decision probabilities.
The UK subgroup looked different. At a UK threshold of £30,000 per QALY, reported as €34,000, probabilities were 82%, 81%, and 71% across the same perspectives. That is the signal worth preserving: PReDicT looked more economically plausible in the UK than at the pooled trial level.
Why country matters: antidepressant costs, primary-care labor, follow-up pathways, thresholds, productivity valuation, and usual-care intensity all differ by health system. A prediction tool that barely changes costs in one country can look more favorable in another if usual care is expensive, monitoring is efficient, or productivity gains are valued differently.
Close Monitoring May Have Helped Both Arms
The comparator was not passive neglect. Participants in both groups received structured trial monitoring, repeated electronic outcome collection, and antidepressant care inside a research framework. That can improve usual care enough to reduce the incremental advantage of the algorithm.
Earlier economic modeling suggested that monitoring negative emotional bias could be cost-effective in primary care.3 The 2026 evaluation is more informative because it used trial data, but it also shows the usual problem with prediction tools: the algorithm’s apparent value depends on what “usual care” already includes.
STAR*D remains the background reason prediction is attractive. In sequential antidepressant treatment, remission becomes harder after failed steps, and delays accumulate.4 A tool that moves nonresponders faster could be useful even if a single 24-week economic evaluation does not deliver a universal cost-effectiveness answer.
Where the Algorithm Could Still Earn Its Place
The economic case for PReDicT may be strongest in settings where usual care is sparse and delayed switching is common. If primary care already monitors symptoms weekly and responds quickly to nonresponse, an algorithm has less room to improve outcomes. If usual care waits months before changing treatment, early nonresponse prediction becomes more valuable.
Implementation cost: the intervention cost averaged €93 per patient in the trial. That number could fall with automation and integration into routine electronic prescribing, or rise if practices need staff time, training, troubleshooting, and extra appointments.
Clinical action: the test did not prescribe a specific switch. It alerted clinicians to likely nonresponse, leaving dose escalation, switching, or augmentation to local guidelines. Economic value therefore depends on what clinicians actually do after the alert.
Patient fit: acceptability work on PReDicT suggested that some patients valued information, monitoring, and confidence in treatment. That softer mechanism may explain why capability and functioning can move even when EQ-5D barely separates groups.
The next useful trial would compare algorithm-guided care against a strong measurement-based-care comparator. That would answer whether PReDicT adds value beyond structured symptom monitoring and ordinary care that may be inconsistent across countries.
The Economic Verdict Depends on the Comparator
Antidepressant prediction tools are often sold as a way out of trial-and-error prescribing. That framing is partly fair, but it hides the key comparator. If the alternative is an unsupported patient left on an ineffective drug for months, early prediction has obvious appeal. If the alternative is high-quality measurement-based care with quick medication review, the incremental gain is harder to prove.
Measurement-based care means routine symptom scoring, side-effect tracking, adherence review, and timely treatment adjustment. PReDicT includes a specialized emotional-bias test, but some of its value may come from forcing early monitoring and clinical action. A future economic study needs to separate the algorithm-specific effect from the monitoring effect.
That distinction matters for payers. A health system may decide that structured PHQ-9 or QIDS-SR monitoring is cheaper and good enough, or it may decide that PReDicT’s early cognitive-emotional signal improves enough decisions to justify the added cost. The 2026 paper supports that debate; it does not end it.
For clinicians, the practical message is also narrower than “use the algorithm.” Early follow-up after starting antidepressants is valuable whether the signal comes from symptom scales, side effects, patient preference, or affective-cognition testing. PReDicT needs to show that its extra information changes enough decisions to outperform simpler structured monitoring.
For patients, the useful takeaway is to expect reassessment early in treatment. If symptoms, side effects, anxiety, functioning, or adherence are not improving, waiting passively for months is rarely the best version of antidepressant care.
Why QALY and capability results can disagree: EQ-5D is a generic quality-adjusted life-year instrument. It is deliberately broad, which helps payers compare depression care with hip surgery, diabetes drugs, or cancer screening. That breadth can make it blunt for changes patients notice first, such as emotional range, work functioning, social confidence, anxiety relief, or feeling able to make plans again.
OxCAP-MH asks a different question: whether mental-health care improves a person’s capabilities, meaning what they are able to do and be in daily life. In the PReDicT evaluation, that capability signal favored algorithm-guided care more clearly than EQ-5D. The result does not prove the algorithm is cost-effective, but it suggests the trial may have moved some outcomes that generic utility scoring underweights.
Country-level variation is not noise to ignore: the UK signal above 80% sits inside a multinational trial where prices, primary-care workflow, follow-up norms, antidepressant prescribing habits, and productivity costs differ. A test that is marginal in one system can become attractive in another if it prevents enough appointments, work loss, medication churn, or delayed switching. The economic result therefore has to be read by setting, not as one universal verdict.
The strict conclusion is that PReDicT did not deliver a clean trial-level QALY win. The practical conclusion is a little more interesting: prediction-guided care may be worth testing where usual care is weak, where early follow-up is hard to enforce, or where capability outcomes carry enough value to justify the extra monitoring cost.
Questions About PReDicT Cost-Effectiveness
Did PReDicT clearly save money?
No. Costs fell in both arms, and group differences were uncertain. The strongest economic signal was in UK subgroup probability, not pooled trial-level dominance.
Why did OxCAP-MH favor PReDicT when EQ-5D did not?
OxCAP-MH measures mental-health capability and broader functioning. EQ-5D is a generic health-utility measure, so it may be less sensitive to some depression-related functioning gains.
Should clinics use PReDicT based on this paper?
The study supports further jurisdiction-specific evaluation, especially where primary-care monitoring can be delivered cheaply. It does not prove universal cost-effectiveness.
References
- Peric N, Mayer S, Helter T, et al. The cost-effectiveness of predictive algorithm guided primary antidepressant treatment: economic evaluation of the multinational PReDicT randomised controlled trial. BJPsych Open. 2026;12:e107. https://doi.org/10.1192/bjo.2026.11021
- Browning M, et al. Prediction of antidepressant treatment response and early treatment switching in depression. Neuropsychopharmacology. 2021. https://doi.org/10.1038/s41386-021-00981-z
- Browning M, Kingslake J, Dourish CT, Goodwin GM, Harmer CJ, Dawson GR. Predicting treatment response to antidepressants with a computerized emotional bias test. Evidence-Based Mental Health. 2019. https://doi.org/10.1136/ebmental-2019-300089
- Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. American Journal of Psychiatry. 2006. https://doi.org/10.1176/appi.ajp.163.11.1905