
A 2026 laboratory study found no detectable acute-pain increase in frequent cannabis users after at least 12 hours of biochemically verified abstinence. Frequent users had higher THC exposure and higher plasma cannabinoid markers, but pain threshold, pain tolerance, and pain ratings did not differ from occasional users.1
Research Highlights
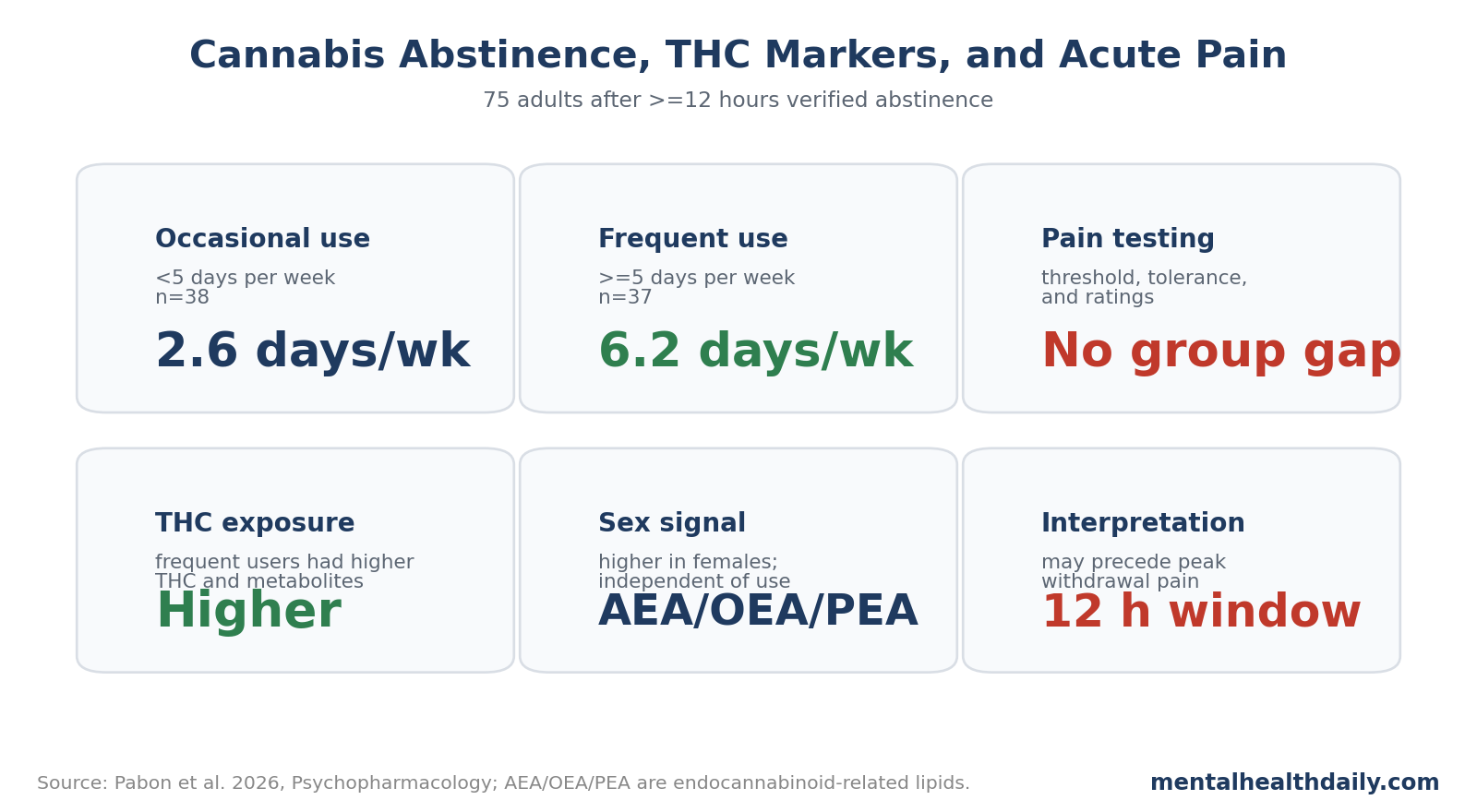
- 75 healthy adults were tested: Pabon et al. compared 38 occasional cannabis users with 37 frequent users after at least 12 hours of verified abstinence.1
- Frequent users had much higher THC exposure: use averaged 6.2 days per week versus 2.6 days per week, and estimated weekly THC exposure was 3,099.3 mg versus 439.7 mg.1
- Pain outcomes did not separate: cold-pressor pain threshold, pain tolerance, and subjective pain ratings did not differ by cannabis-use frequency, sex, weekly THC exposure, or plasma cannabinoid levels.1
- THC biology still separated the groups: frequent users had higher plasma THC, 11-hydroxy-THC, and 11-nor-9-carboxy-THC, confirming that exposure differences were measurable.1
- The abstinence window may be too short: cannabis withdrawal symptoms often emerge around 24 hours and peak near 72 hours, so this study mainly tests early abstinence, not full withdrawal.2
The useful interpretation is narrow but important: brief abstinence in otherwise healthy adult cannabis users did not produce cold-pressor hyperalgesia. Hyperalgesia means increased pain sensitivity; the study did not rule out withdrawal pain after longer abstinence, chronic-pain samples, or cannabis use disorder.
75 Adults Completed Pain Testing After 12-Hour Cannabis Abstinence
The study enrolled 75 healthy adults aged 21-55 years. Participants were cannabis users but not necessarily chronic-pain patients, and the experiment was designed to avoid acute intoxication while capturing early abstinence.1
The 2 groups were separated by recent use frequency:
- Occasional users: <5 days per week, n = 38.
- Frequent users: ≥5 days per week, n = 37.
- Average use days: 2.6 per week in occasional users versus 6.2 per week in frequent users.
- Average grams per occasion: 0.6 versus 2.0.
- Average estimated weekly THC exposure: 439.7 mg versus 3,099.3 mg.
Participants completed a cold pressor test. They first placed a hand in warm water, then transferred it to 4°C cold water. Researchers measured pain threshold, or time to first pain, and pain tolerance, or time to hand withdrawal. Participants also rated the pain using subjective scales.
This setup is a standard experimental pain model, but it is not the same as back pain, neuropathy, migraine, fibromyalgia, or postoperative pain. The result is strongest for acute cold-induced pain in a controlled lab setting.
Frequent Cannabis Use Raised THC Markers, Not Acute Pain
The exposure manipulation worked. Frequent users had higher plasma THC, 11-hydroxy-THC, and 11-nor-9-carboxy-THC than occasional users:
- THC: F(1,62) = 9.6, p = 0.003.
- 11-hydroxy-THC: F(1,51) = 5.7, p = 0.021.
- 11-nor-9-carboxy-THC: F(1,65) = 19.3, p < 0.001.
- Weekly THC exposure correlated with plasma THC, p = 0.010.
- Weekly THC exposure correlated with plasma 11-nor-9-carboxy-THC, p = 0.009.
The groups also differed in several use-pattern variables. Frequent users reported higher Cannabis Use Disorder Identification Test-Revised (CUDIT-R) scores, higher grams per occasion, and higher product THC concentration. CUDIT-R is a cannabis-problem screening scale, so the frequent-use group used cannabis on more days and also carried more cannabis-related risk markers.
The pain result went the other way: pain threshold, pain tolerance, and subjective pain ratings did not differ by use frequency or sex and were not associated with weekly THC exposure.
That is the main calibration. This was not a study where cannabis exposure failed to separate biologically. It did separate. The missing signal was pain sensitivity after a short abstinence window.
The absence of association with plasma cannabinoids is also useful. If higher circulating THC or metabolites directly increased acute cold pain during early abstinence, the study had a reasonable chance to see at least a directional relationship. Instead, the cannabinoid measures separated exposure groups while pain measures stayed flat.
That makes a simple dose-response story less likely for early abstinence in healthy adults. A later-withdrawal story, a chronic-pain-subgroup story, or a product-specific story remains possible.
Brief Abstinence Is Not the Same as Cannabis Withdrawal
The 12-hour abstinence window is the key limitation and the key design strength. It reduced acute intoxication effects, but it likely occurred before peak withdrawal physiology for many users.
Haney et al. showed that abstinence symptoms after smoked cannabis can emerge after cessation and peak later than the first half-day.2 Pabon et al. cited evidence that withdrawal symptoms often emerge around 24 hours and peak near 72 hours. That timing makes a null pain result at 12 hours unsurprising if withdrawal-related hyperalgesia needs a longer abstinence interval.
The study therefore answers 1 question better than another:
- Better answered: Do healthy frequent users show increased cold-pressor pain after brief verified abstinence? In this sample, no.
- Less answered: Do heavy users develop pain sensitivity during full withdrawal, after several days of abstinence, or in chronic-pain populations? That remains open.
This distinction also helps with clinical claims. Some cannabis users report pain worsening when they stop. That experience may be real for some people, but this experiment does not show a broad early-abstinence pain effect in healthy adults.
Frequent Use and Chronic Pain Are a Different Question
Medical cannabis is often used for chronic pain, but clinical evidence remains mixed and product composition varies widely. A 2022 systematic review found small to moderate short-term pain improvements for some cannabis-based products, along with increased dizziness and sedation, but the evidence base was limited by study quality and product heterogeneity.3
High-frequency use may also correlate with worse pain in chronic-pain samples. Boehnke et al. reported that high-frequency medical cannabis use was associated with worse pain among people with chronic pain.4 That does not prove cannabis caused worse pain, because sicker patients may use more cannabis, but it warns against assuming that more use always means better pain control.
Pabon et al. studied healthy users, not patients seeking analgesia. That difference is central:
- Healthy users may have normal baseline pain processing.
- Chronic-pain patients may have sensitized nervous systems before cannabis enters the picture.
- People with cannabis use disorder may have withdrawal dynamics different from recreational users.
- THC-dominant products may differ from balanced THC/CBD products.
It also matters that acute pain and chronic pain answer different biological questions. Cold-pressor pain is brief, externally triggered, and measured over minutes. Chronic pain is ongoing, emotionally loaded, sleep-disrupting, and shaped by avoidance, inflammation, central sensitization, and expectations.
That gap is why the study should not be used as a blanket reassurance for all cannabis-pain interactions. It is a clean negative result for one controlled pain model after early abstinence.
The lab finding should therefore be used to refine the hypothesis, not settle the medical cannabis pain debate.
Sex Differences Appeared in Endocannabinoid-Related Lipids
Pabon et al. also measured endogenous cannabinoid-related lipids. Females had higher circulating anandamide (AEA), oleoylethanolamide (OEA), and palmitoylethanolamide (PEA) than males, independent of cannabis-use frequency.1
Those molecules are not interchangeable with THC. Anandamide is an endogenous cannabinoid, while OEA and PEA are related lipid signaling molecules that can influence pain, inflammation, satiety, and stress biology.
The sex difference did not translate into a pain difference in this experiment. Still, it fits a broader literature showing sex-dependent cannabinoid effects and sex differences in experimental pain response.5,6
A stronger follow-up would test longer abstinence windows, women across menstrual-cycle phases, men and women separately, and participants with chronic pain. That design could distinguish 3 possibilities:
- No withdrawal-pain effect: pain sensitivity remains unchanged even after longer abstinence.
- Time-limited effect: pain sensitivity appears after 24-72 hours, then resolves.
- Subgroup effect: pain sensitivity appears mainly in chronic-pain patients, high-THC concentrate users, or people with cannabis use disorder.
Limitations of the Cannabis Pain Study
- Short abstinence period. At least 12 hours may be too early for withdrawal-related pain sensitivity.
- Healthy adult sample. Results may not generalize to chronic-pain patients or people using cannabis medically for analgesia.
- Cold pressor only. Cold-induced acute pain is useful but does not represent every pain pathway.
- Group confounding. Frequent and occasional users differed in BMI and ethnicity distribution, though demographic differences did not explain the main pain result.
- Product variability. Real-world cannabis differs by THC, CBD, route, terpene profile, and concentrate use.
Questions About Cannabis Abstinence and Pain
Did frequent cannabis users feel more acute pain after stopping?
Not in this study. After at least 12 hours of verified abstinence, frequent users did not differ from occasional users on pain threshold, tolerance, or ratings.
Does this disprove cannabis withdrawal pain?
No. The abstinence window was short. Withdrawal-related pain could require longer abstinence or appear mainly in clinical subgroups.
Were frequent users actually more exposed to THC?
Yes. They used cannabis more often, had higher estimated weekly THC exposure, and had higher plasma THC metabolites.
Should this change chronic-pain treatment decisions?
It should temper simple claims. Brief abstinence did not raise acute pain in healthy adults, but chronic-pain treatment decisions need evidence from chronic-pain populations, product-specific trials, and longer follow-up.
References
- Pabon E, et al. Cannabis use patterns and perception of acute pain after brief abstinence. Psychopharmacology. 2026. doi:10.1007/s00213-026-07063-2
- Haney M, Ward AS, Comer SD, Foltin RW, Fischman MW. Abstinence symptoms following smoked marijuana in humans. Psychopharmacology. 1999;141:395-404. doi:10.1007/s002130050849
- McDonagh MS, Morasco BJ, Wagner J, et al. Cannabis-based products for chronic pain: a systematic review. Annals of Internal Medicine. 2022;175:1143-1153. doi:10.7326/M21-4520
- Boehnke KF, Scott JR, Litinas E, Sisley S, Williams DA, Clauw DJ. High-frequency medical cannabis use is associated with worse pain among individuals with chronic pain. Journal of Pain. 2020;21:570-581. doi:10.1016/j.jpain.2019.09.006
- Cooper ZD, Craft RM. Sex-dependent effects of cannabis and cannabinoids. Neuropsychopharmacology. 2018;43:34-51. doi:10.1038/npp.2017.140
- Bartley EJ, Fillingim RB. Sex differences in pain: a brief review of clinical and experimental findings. British Journal of Anesthesia. 2013;111:52-58. doi:10.1093/bja/aet127