In 433 non-demented amyotrophic lateral sclerosis (ALS) patients, clinically significant anxiety was present in 18.2% for state anxiety and 13.9% for trait anxiety. The strongest predictor was not motor severity, cognition, or caregiver-rated behavior; it was depression, especially cognitive-affective depression symptoms.1
Research Highlights
- ALS anxiety was measurable but not universal: Aiello et al. found clinically significant state anxiety in 18.2% of ALS patients and trait anxiety in 13.9%.1
- Controls had lower anxiety rates: state anxiety above cut-off was 1.6% in healthy controls, and trait anxiety above cut-off was 7.0%.1
- Depression carried the prediction: Beck Depression Inventory cognitive-affective scores predicted both State-Trait Anxiety Inventory anxiety scores and above-cut-off anxiety classifications.1
- Depression outperformed motor and cognitive variables: disease duration, progression rate, Edinburgh Cognitive and Behavioral ALS Screen scores, and caregiver-rated behavioral scores did not survive the adjusted predictor threshold.1
- Clinical screening should pair anxiety and depression: the pattern supports combined psychological assessment because anxiety tracked mood burden more clearly than motor stage or frontotemporal-behavior markers.1
Amyotrophic lateral sclerosis is a progressive motor neuron disease, but psychiatric symptoms are part of ALS care. Anxiety can affect quality of life, caregiver burden, treatment planning, communication, sleep, and willingness to engage with respiratory or nutritional support.2,7
Aiello et al. Compared 433 ALS Patients With 313 Controls
The 2026 study analyzed 433 non-demented ALS patients referred to IRCCS Istituto Auxologico Italiano in Milan between 2016 and 2024. The comparison group included 313 healthy controls without neurological or psychiatric disorders, active psychotropic medication use, or severe uncompensated medical illness.1
The ALS sample was not limited to mild disease, but it excluded patients with comorbid frontotemporal dementia (FTD). That choice made the sample more homogeneous, but it also means the results should not be extended to ALS-FTD without caution.
- ALS sample size: 433 patients.
- Control sample size: 313 healthy controls.
- Mean ALS age: 63.4 years.
- Mean disease duration: 18.6 months.
- ALSFRS-R mean: 38.7 on the Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised (ALSFRS-R), where lower scores reflect worse motor function.
- Cognitive impairment: 31.2% were impaired on the Edinburgh Cognitive and Behavioral ALS Screen (ECAS).
Both patients and controls completed the State-Trait Anxiety Inventory Form Y (STAI-Y). STAI-Y1 measures state anxiety, meaning anxiety tied to the current situation. STAI-Y2 measures trait anxiety, meaning a more stable tendency toward anxiety.
State Anxiety Was 18.2%, Trait Anxiety Was 13.9%
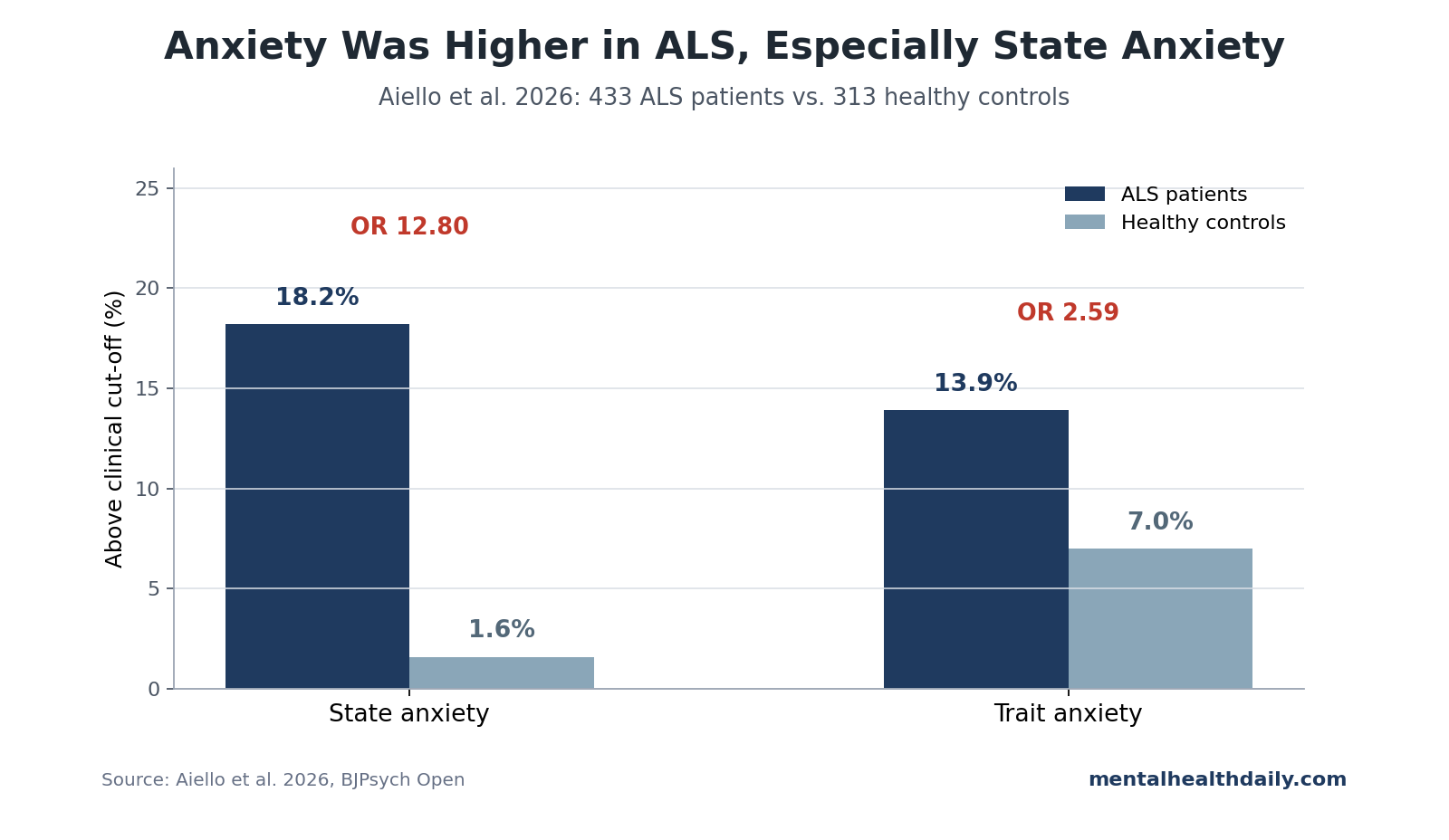
Age-stratified Italian cut-offs showed clinically significant state anxiety in 79 of 433 ALS patients and clinically significant trait anxiety in 60 of 433. Controls were lower on both classifications.
- State anxiety above cut-off: 18.2% in ALS vs. 1.6% in controls, p < 0.001.
- Trait anxiety above cut-off: 13.9% in ALS vs. 7.0% in controls, p = 0.003.
- Mean STAI-Y1 score: 51.7 in ALS vs. 41.9 in controls, p < 0.001.
- Mean STAI-Y2 score: 49.7 in ALS vs. 45.6 in controls, p < 0.001.
After adjustment for age, education, and gender, ALS patients had higher odds of abnormal anxiety classification than controls: odds ratio (OR) 12.80 for state anxiety and OR 2.59 for trait anxiety.1
Depression Was Also Much More Common in ALS
The anxiety result sits inside a broader mood pattern. Beck Depression Inventory (BDI) scores were higher in ALS patients than in controls, and depression classification differed sharply between groups.
- No depression: 36.4% of ALS patients vs. 77.6% of controls.
- Mild depression: 35.7% of ALS patients vs. 16.3% of controls.
- Moderate depression: 23.5% of ALS patients vs. 5.4% of controls.
- Severe depression: 4.5% of ALS patients vs. 0.6% of controls.
This helps explain why depression variables dominated the anxiety models. Anxiety clustered with cognitive-affective depressive symptoms, somatic depressive symptoms, or both.
Depression Explained Anxiety Better Than Motor Severity
The regression models tested motor, cognitive, behavioral, and depression predictors at the same time. That design is useful because ALS anxiety can be interpreted in several competing ways: emotional response to diagnosis, depression overlap, motor disability, cognitive impairment, or frontotemporal behavioral change.
The strongest result was the depression link:
- State anxiety scores: cognitive-affective Beck Depression Inventory (BDI-CA) scores predicted STAI-Y1, beta = 0.44, p < 0.001.
- State anxiety classification: each BDI-CA increase raised odds of above-cut-off state anxiety, OR 1.19, 95% CI 1.11-1.28, p < 0.001.
- Trait anxiety scores: BDI-CA predicted STAI-Y2, beta = 0.55, p < 0.001; BDI somatic-performance score also predicted STAI-Y2, beta = 0.17, p = 0.003.
- Trait anxiety classification: BDI-CA predicted above-cut-off trait anxiety, OR 1.17, 95% CI 1.08-1.28, p < 0.001.
Motor variables did not carry the main interpretation. Disease duration, progression rate, and most motor-status associations did not survive the adjusted threshold. ALSFRS-R had a marginal association with state anxiety, but the broader pattern did not support a simple “worse paralysis equals more anxiety” reading.
The ALSFRS-R detail is still worth preserving. The marginal positive association went in the counterintuitive direction: better motor status related to higher state anxiety. Aiello et al. suggested that earlier disease phases may involve acute emotional adjustment, when patients are still processing diagnosis and impending loss of function.1
That interpretation also fits prior longitudinal work showing anxiety can be high near diagnosis and then change over the disease trajectory.4 Anxiety in ALS may therefore be partly stage-dependent, but not reducible to a simple motor-disability score.
Cognition and Behavior Did Not Account for the Anxiety Pattern
ALS can overlap with frontotemporal cognitive and behavioral changes. That makes it tempting to treat anxiety as part of a frontotemporal-spectrum behavioral profile. The Aiello analysis did not support that interpretation for this non-demented sample.
ECAS subscales for language, fluency, executive function, memory, and visuospatial ability were not significant predictors of STAI-Y1 or STAI-Y2 after model adjustment. Caregiver-rated Frontal Behavioral Inventory negative and positive behavior scores also failed to explain anxiety classifications.1
That does not rule out psychiatric symptoms in ALS-FTD. It narrows this specific cohort: among non-demented ALS patients, anxiety tracked mood symptoms more clearly than cognition or caregiver-rated behavior.
The distinction is clinically useful because ALS clinics often have to sort several overlapping problems at once:
- Motor disability: weakness, respiratory decline, swallowing problems, and loss of independence.
- Cognitive change: executive dysfunction, language change, or broader ALS-frontotemporal-spectrum impairment.
- Behavioral change: apathy, disinhibition, irritability, or caregiver-reported dysexecutive behavior.
- Mood and anxiety: fear, worry, demoralization, panic, depression, and diagnosis-related distress.
Aiello et al. do not collapse these into one bucket. Their models suggest that anxiety screening should not be postponed until cognitive or behavioral change is obvious.
ALS Anxiety Screening Should Pair STAI and Depression Measures
The care implication is practical. If anxiety is strongly tied to depression, screening only for motor progression or cognitive status will miss part of the psychological burden.
A better clinical screen would include:
- Anxiety severity: a disease-appropriate anxiety measure such as STAI-Y or a validated ALS/motor-neuron-disease anxiety scale.
- Depression severity: a depression measure that separates cognitive-affective symptoms from somatic symptoms that may overlap with ALS disability.
- Adjustment and coping: questions about diagnosis shock, loss of independence, respiratory fears, communication changes, and caregiver stress.
- Referral thresholds: a pathway from screening to psychological evaluation, cognitive-behavioral therapy, mindfulness-based care, medication review, or palliative/supportive care consultation when needed.8
This is not an argument that every ALS patient has clinically significant anxiety. The study’s estimate is more calibrated: anxiety is elevated compared with controls, but most non-demented ALS patients did not cross the clinical cut-off at the measured time point.
That calibrated prevalence estimate guides intervention design. Universal high-intensity psychotherapy for every patient would overread the result, but routine screening with stepped referral fits the data. Patients with above-cut-off anxiety or depression can receive targeted support, and patients without clinical-range distress can still be monitored as disease demands change.
Psychological Treatment Evidence Is Still Developing
The treatment literature in motor neuron disease is smaller than the screening literature. A scoping review found psychological interventions for motor neuron disease, including cognitive-behavioral and mindfulness-oriented approaches, but the evidence base remains heterogeneous and not large enough to settle optimal protocol, timing, or patient selection.8
Still, the Aiello pattern supports a practical care sequence:
- Screen anxiety and depression together. Treating them as separate silos misses their overlap.
- Use ALS-aware scales when possible. Somatic symptoms can reflect neurological disease rather than depression alone.
- Ask about adjustment and coping. Diagnosis phase, respiratory fears, communication changes, and caregiver strain may shape anxiety.
- Refer when symptoms cross threshold. Psychological care, medication review, palliative support, or caregiver intervention may be appropriate depending on the presentation.
Limitations of the ALS Anxiety Analysis
- Retrospective clinical data. The dataset came from clinical assessments rather than a prospective anxiety study, so measurement timing and missingness matter.
- No ALS-FTD group. Excluding full frontotemporal dementia improved sample consistency, but it limits conclusions about anxiety in ALS-FTD.
- Depression scale overlap. The Beck Depression Inventory includes somatic items that can overlap with neurological disability, so ALS-specific depression tools may sharpen future analyses.
- Coping was not measured. Coping style, family support, respiratory fears, communication loss, and care context may explain anxiety beyond the variables tested here.
Questions About Anxiety in ALS
How common was clinically significant anxiety in this ALS cohort?
State anxiety appeared in 18.2% of patients, and trait anxiety appeared in 13.9%.
Was anxiety just a marker of worse motor function?
No. Motor severity and progression did not explain the main anxiety pattern. Depression, especially cognitive-affective depression symptoms, was the consistent predictor.
Did cognition explain anxiety?
No clear evidence for that appeared in this non-demented ALS sample. ECAS cognitive subscales did not survive the adjusted predictor threshold.
What should clinicians screen for?
Anxiety and depression should be assessed together. The study supports psychological screening that can distinguish cognitive-affective distress from motor disability and somatic symptoms.
References
- Aiello EN, De Luca G, Curti B, et al. Prevalence and determinants of anxiety in amyotrophic lateral sclerosis. BJPsych Open. 2026;12:e114. doi:10.1192/bjo.2026.11025
- Kurt A, Nijboer F, Matuz T, Kubler A. Depression and anxiety in individuals with amyotrophic lateral sclerosis: epidemiology and management. CNS Drugs. 2007;21:279-291. doi:10.2165/00023210-200721040-00003
- Siciliano M, Trojano L, Trojsi F, et al. Assessing anxiety and its correlates in amyotrophic lateral sclerosis: the State-Trait Anxiety Inventory. Muscle Nerve. 2019;60:47-55. doi:10.1002/mus.26475
- Larsson BJ, Nordin K, Nygren I. Symptoms of anxiety and depression in patients with amyotrophic lateral sclerosis and their relatives during the disease trajectory. Journal of the Neurological Sciences. 2023;455:122780. doi:10.1016/j.jns.2023.122780
- Carelli L, Solca F, Faini A, et al. The complex interplay between depression/anxiety and executive functioning: insights from the ECAS in a large ALS population. Frontiers in Psychology. 2018;9:450. doi:10.3389/fpsyg.2018.00450
- Faltracco V, Pain D, Dalla Bella E, et al. Mood disorders in patients with motor neuron disease and frontotemporal symptoms: validation of the Hospital Anxiety and Depression Scale for use in motor neuron disease. Journal of the Neurological Sciences. 2025;469:123378. doi:10.1016/j.jns.2024.123378
- Vignola A, Guzzo A, Calvo A, et al. Anxiety undermines quality of life in ALS patients and caregivers. European Journal of Neurology. 2008;15:1231-1236. doi:10.1111/j.1468-1331.2008.02303.x
- Zarotti N, Mayberry E, Ovaska-Stafford N, Eccles F, Simpson J. Psychological interventions for people with motor neuron disease: a scoping review. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration. 2021;22:1-11. doi:10.1080/21678421.2020.1788094