A 2026 preprint combining 2,189 university participants with 477 clinical patients with problematic sexual behavior found a gender-specific self-harm signal: women with problematic sexual behavior had higher non-suicidal self-injury risk, but clinical severity of problematic sexual behavior did not predict NSSI inside the patient cohort.1
Research Highlights
- Total sample was 2,666 people: Jiang et al. analyzed 2,189 university participants and 477 clinical patients with problematic sexual behavior.1
- Overall NSSI rates were similar: NSSI appeared in 7.1% of the university cohort and 5.7% of the clinical PSB cohort (p = 0.25).1
- Women’s subgroup carried the signal: women with PSB had 4.44 times higher odds of NSSI than men without PSB (OR = 4.44, p = 0.037), and women PSB patients had higher NSSI prevalence than university women (29.6% vs. 9.3%, p < 0.001).1
- Clinical severity was not the answer: within clinical PSB patients, PSB severity was not associated with NSSI (OR = 1.10, p = 0.25).1
- Preoccupation stood out: among university women, the preoccupation dimension was associated with NSSI (OR = 2.69, p < 0.001), while relationship disturbance, loss of control, and affect disturbance did not remain significant in the same model.1
Non-suicidal self-injury (NSSI) means deliberate self-injury without intent to die. It can serve emotion-regulation, anti-dissociation, self-punishment, interpersonal, or compulsive functions, so it should not be casually collapsed into suicide attempt or attention-seeking language.
Problematic sexual behavior (PSB) means sexual behavior marked by distress, impairment, loss of control, preoccupation, relationship disturbance, or repeated behavior despite harm. The difficult clinical question is whether PSB and NSSI sometimes share emotion-regulation or compulsive pathways without turning sexual behavior itself into a moralized label.
The study’s framing avoids 2 bad shortcuts. One shortcut is to treat sexual behavior as self-harm whenever shame or distress is present. The other is to keep sexual behavior and self-injury in separate clinical silos even when the same person is using both to manage distress.
Jiang et al. tested the middle question: whether NSSI clustered with PSB status, PSB severity, gender, trauma, and specific addictive dimensions.
The answer was not a broad “PSB equals self-harm” finding. The answer was narrower and more clinically actionable: women with PSB were the subgroup where NSSI risk rose, and preoccupation looked more relevant than overall clinical PSB severity.
Women With PSB Had the Clearest NSSI Signal
In the university cohort, NSSI was more common among people with PSB than among those without it: 13.1% vs. 6.3% (p < 0.001). But that aggregate result hid the key pattern. The difference was significant in women (24.3% vs. 7.7%, p < 0.001) and absent in men (2.8% vs. 2.2%, p = 0.68).1
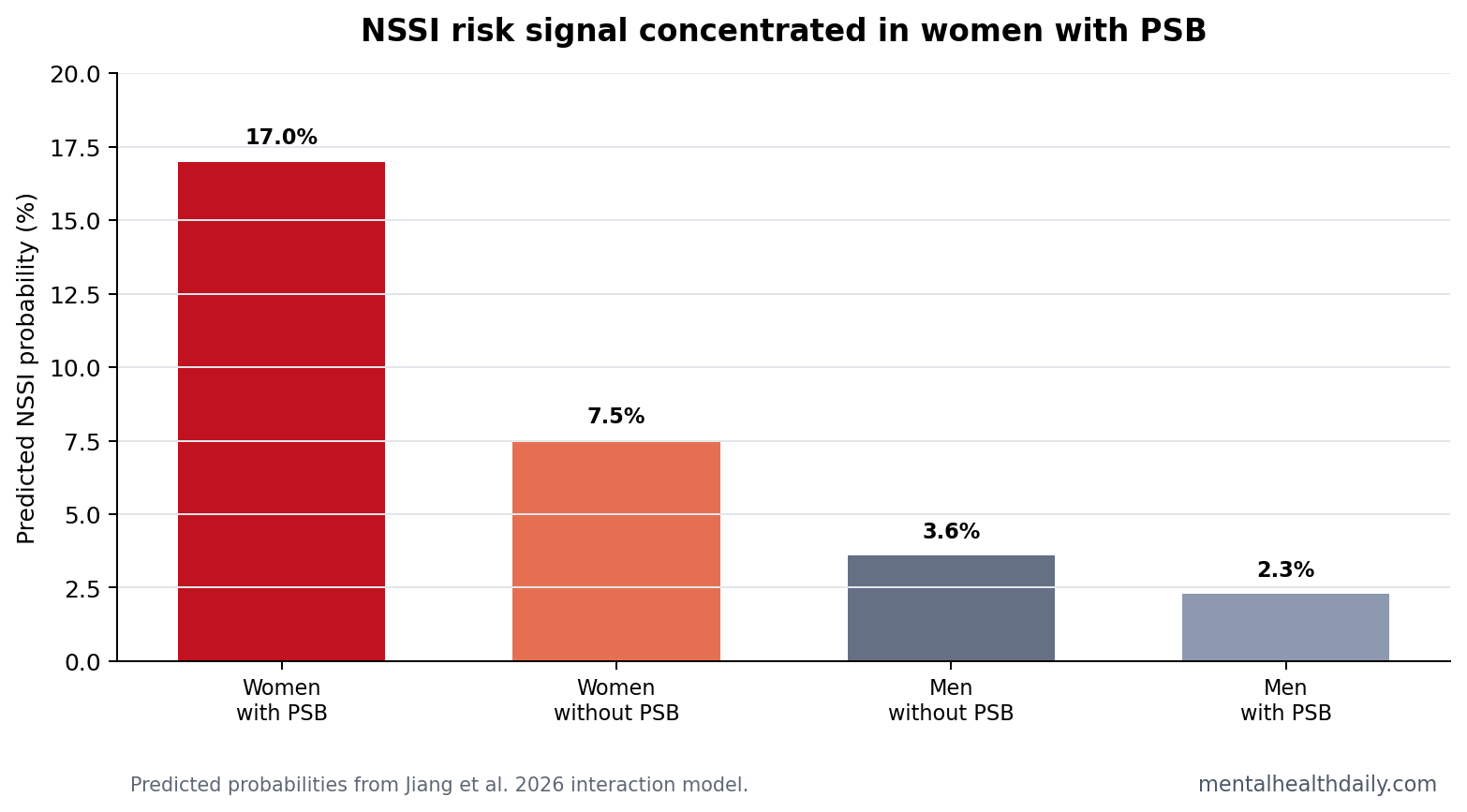
The interaction model made the same point more sharply. Women with PSB had 4.44 times higher odds of NSSI than men without PSB. Predicted probability was highest in women with PSB at 0.17, compared with 0.075 in women without PSB, 0.036 in men without PSB, and 0.023 in men with PSB.1
Those probabilities are easier to interpret than the odds ratio alone. In practical terms, the model estimated roughly 17 NSSI cases per 100 women with PSB, compared with about 8 per 100 women without PSB and 2-4 per 100 men. That is a subgroup signal, not a universal PSB signal.
PSB Severity Did Not Explain NSSI in Clinical Patients
The patient cohort prevented a simple severity story. Inside the 477-person clinical PSB cohort, younger age, female gender, and childhood trauma were associated with NSSI, but PSB severity was not (OR = 1.10, p = 0.25).1
That result is clinically useful because it separates 2 questions. One question is whether PSB status marks an NSSI risk subgroup in a broad young-adult population. The answer was yes, mainly among women. The other question is whether more severe PSB predicts NSSI among people already in PSB care. In this preprint, the answer was no.
Clinical severity may have failed because the patient cohort was already selected for PSB. Once everyone crosses a treatment threshold, incremental symptom severity may be less informative than trauma history, age, gender, shame, obsessive preoccupation, or emotion-regulation style. That is why the negative severity result should not be dismissed as a null footnote.
Preoccupation Looked More Relevant Than Loss of Control
The addictive-dimensions analysis pointed toward preoccupation. Among university women, all 4 PSB dimensions were higher in those with NSSI, but regression identified preoccupation as the dimension that remained associated with NSSI (OR = 2.69, p < 0.001).1
Preoccupation means intrusive or repetitive mental focus on sexual behavior, not high libido by itself. A preoccupation signal fits a model where repetitive thoughts, shame, distress, and emotion-regulation attempts become entangled. It does not prove that PSB causes self-injury.
The high-risk subgroup result was also not tidy: women who met the PSB threshold and had NSSI reported higher preoccupation scores but unexpectedly lower loss-of-control scores than women without NSSI. That pattern argues against treating every PSB-NSSI case as the same loss-of-control phenotype.
McKay and Andover made a related point when evaluating whether NSSI belongs in an obsessive-compulsive-related category: overlap with compulsive processes can exist without making NSSI the same disorder as obsessive-compulsive disorder.4 The same caution applies here. PSB and NSSI may share repetitive distress loops in some people, while other cases may be driven by trauma, dissociation, interpersonal conflict, impulsivity, or avoidance.
Childhood Trauma Stayed a Major Covariate
Childhood trauma remained strongly associated with NSSI in both main regression contexts: OR = 7.61 in the university model without the interaction term, OR = 7.76 after adding the gender-by-PSB interaction, and OR = 3.79 in the clinical PSB cohort.1
That trauma signal fits broader NSSI literature. Bresin and Schoenleber found gender differences in NSSI prevalence across a large meta-analysis, and Swannell et al. showed that nonclinical NSSI prevalence is highly sensitive to age, sample type, and measurement method.2,3 Jiang et al. add a PSB-specific layer, not a replacement for established trauma and developmental risk factors.
Assessment implication: trauma history should be asked about directly and carefully, not inferred from sexual behavior or self-injury. A trauma-informed assessment can ask what function the behavior serves, what emotions precede it, whether the person feels controlled by it, and whether shame or secrecy is worsening risk.
The Findings Should Not Stigmatize Sexual Behavior
Evidence-strength note: this was a cross-sectional preprint using self-reported sensitive behaviors. It cannot establish whether PSB increases NSSI, whether NSSI increases vulnerability to PSB, or whether both reflect shared trauma, affect regulation, compulsivity, shame, or other unmeasured psychiatric processes.
The best clinical use is targeted assessment. In women presenting with PSB, especially when preoccupation, trauma history, and distress are present, clinicians should ask about NSSI directly and nonjudgmentally. That is different from assuming sexual behavior is self-harm or treating PSB as a moral category.
Stigma is a real measurement problem in this topic. Underreporting is plausible for both NSSI and PSB, and the study relied on self-report for sensitive material. The finding is strong enough to justify better screening, but not strong enough to assign identity labels or causal explanations to individual patients.
A useful assessment therefore starts with function, timing, and current risk. Did self-injury reduce numbness, punish the self, stop intrusive thoughts, or communicate distress? Did sexual preoccupation rise before self-injury urges, or did both follow trauma reminders, rejection, intoxication, or isolation? Those answers separate acute safety planning from longer-term work on shame, compulsive loops, and emotion regulation.
Future studies need longitudinal timing. If PSB preoccupation rises before NSSI episodes, treatment might focus on intrusive sexual thoughts, shame, and coping alternatives. If NSSI precedes PSB escalation, the treatment target may be broader self-harm risk and emotion regulation. If both rise after trauma reminders or interpersonal stress, the shared trigger becomes the clinically useful signal.
Measurement also has to distinguish behavior, distress, and impairment. A high-frequency sexual behavior pattern without impairment is not the same as PSB. A history of NSSI without current urges is not the same as acute safety risk. Combining those distinctions with gender and trauma data would make the next model more clinically useful than a simple yes/no association.
For now, the actionable standard is screening without assumption: ask about NSSI when PSB is clinically significant, and ask about sexual preoccupation when NSSI appears tied to shame, compulsion, or interpersonal distress.
Questions About NSSI and Problematic Sexual Behavior
Did PSB raise NSSI risk in men?
Not in this study. Men with PSB and men without PSB had similar NSSI rates in the university cohort, and the model estimated the lowest predicted NSSI probability in men with PSB.
Was NSSI more common in clinical PSB patients overall?
No. Overall NSSI prevalence was 5.7% in clinical PSB patients and 7.1% in the university cohort. The difference appeared after stratifying by gender, especially among women.
What should clinicians screen for first?
Ask about NSSI, trauma history, intrusive sexual preoccupation, affect regulation, and current safety. Severity of PSB alone did not identify NSSI risk in the clinical cohort.
References
- Jiang S, et al. Exploring the relationship between non-suicidal self-injury and problematic sexual behavior. medRxiv. 2026. doi:10.64898/2026.04.17.26351044
- Bresin K, Schoenleber M. Gender differences in the prevalence of nonsuicidal self-injury: A meta-analysis. Clinical Psychology Review. 2015. https://doi.org/10.1016/j.cpr.2015.02.009
- Swannell SV, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: Systematic review, meta-analysis and meta-regression. Suicide and Life-Threatening Behavior. 2014. https://doi.org/10.1111/sltb.12070
- McKay D, Andover MS. Should nonsuicidal self-injury be a putative obsessive-compulsive-related condition? A critical appraisal. Behavior Modification. 2012. https://doi.org/10.1177/0145445511417707