A 2026 Saudi tertiary-hospital study estimated that adults treated for fibromyalgia — chronic widespread pain with fatigue, sleep disruption, cognitive symptoms, and overlapping mood or medical problems — generated SAR 9,601.2 (USD 2,560.3) in annual direct medical costs per patient, with specialist visits and diagnostic procedures accounting for 96.3% of recorded spending.1
Research Highlights
- Annual direct cost: 128 Saudi fibromyalgia patients averaged SAR 9,601.2 (USD 2,560.3) in healthcare-system costs over 1 year.1
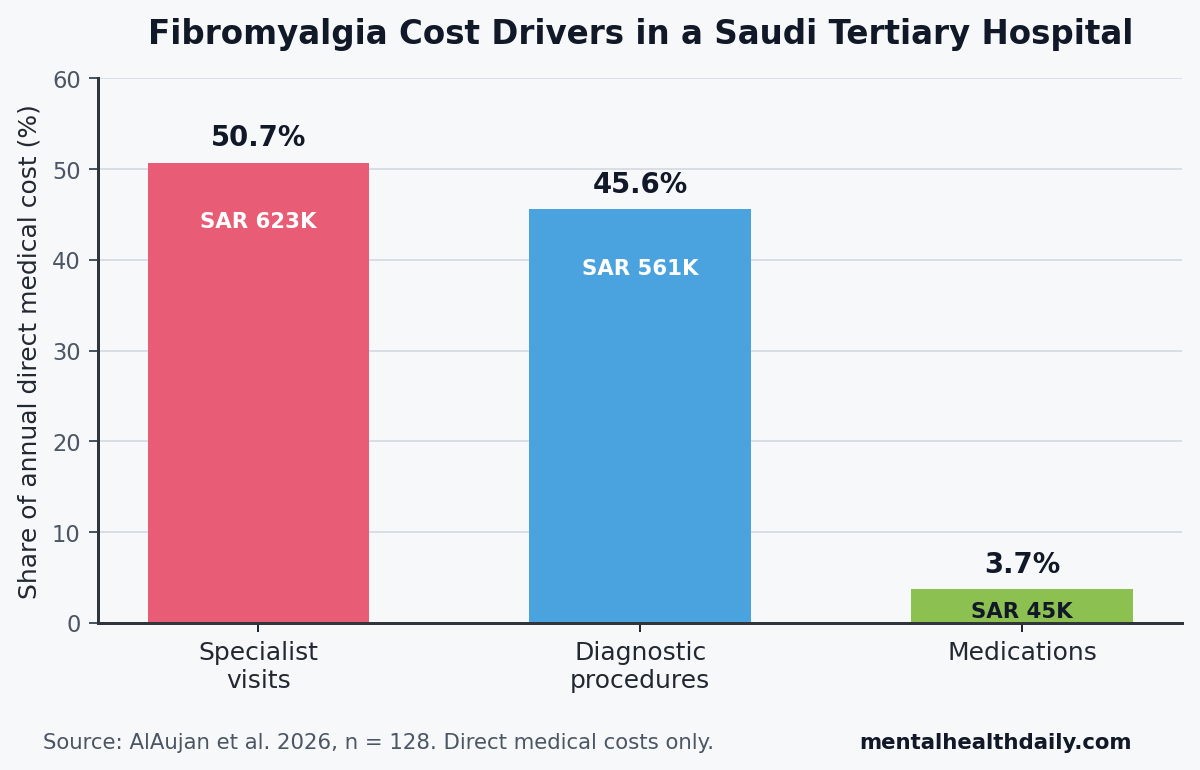
- Cost driver split: specialist visits made up 50.7% of direct costs, diagnostic procedures made up 45.6%, and medications made up only 3.7%.1
- Testing burden: 86.7% of patients had laboratory testing, with a mean of 142.2 lab tests per patient and SAR 3,268.5 in lab costs per patient.1
- Medication pattern: antidepressants were prescribed to 77.3% of patients, anti-epileptic drugs to 43.0%, and opioids to 25.8%, but drug spending stayed small compared with visits and testing.1
- Interpretation limit: the Saudi estimate captures direct hospital costs, not productivity loss, private-sector care, symptom severity, nonmedical spending, or the broader life burden that often dominates fibromyalgia economics.2
The number is useful because it is local: fibromyalgia cost estimates from North America and Europe do not automatically transfer to Saudi Arabia, where referral patterns, public-sector billing, medication procurement, and diagnostic workups differ.
At the same time, the study should not be read as a national total-cost estimate. It is a 1-year, medical-record-based view of direct medical spending inside 1 governmental tertiary hospital in Riyadh.
Specialist Visits and Diagnostic Procedures Drove 96.3% of Direct Costs
Direct medical cost means money spent by the healthcare system on recorded medical services: clinic visits, diagnostic procedures, medications, emergency care, and other billed care. It does not include lost work, travel, informal caregiving, pain-related quality-of-life loss, or private out-of-pocket spending.
AlAujan et al. analyzed 128 adults with confirmed fibromyalgia treated between February 2021 and February 2022 at King Fahad Medical City in Riyadh. The study used a bottom-up cost-of-illness method, meaning the researchers counted the healthcare resources used by each patient and multiplied those services by unit costs from the hospital billing system.1
The cost pattern was unusually clear. The total annual direct medical cost was SAR 1,228,955.3 (USD 327,721.4), or SAR 9,601.2 (USD 2,560.3) per patient. Specialist-care visits accounted for SAR 623,390.2, diagnostic procedures for SAR 560,734.2, and medications for SAR 44,830.9.
Testing was not a side category: 86.7% of patients had at least 1 laboratory test, and the mean laboratory count was 142.2 tests per patient. Laboratory tests alone averaged SAR 3,268.5 (USD 871.6) per patient, more than any specialist category and far more than drug spending.
Rheumatology was common but not the biggest per-patient cost: 52.3% of patients saw rheumatology, with a mean of 1.2 visits per patient per year. Endocrinology had a higher mean cost per patient at SAR 406.3, emergency medicine averaged SAR 379.7, and rheumatology averaged SAR 360.9.
Medication spending was small in this system: antidepressants were the most prescribed drug class, but antidepressant costs averaged SAR 84.4 per patient. Opioids averaged SAR 78.8 per patient. All medications together accounted for 3.7% of total direct medical costs.
High Comorbidity Load Explains Some of the Service Use
Fibromyalgia rarely behaves like a single-pain diagnosis in medical records. In this Saudi cohort, 56.3% of patients had 3 or more comorbidities, and only 9.4% had no recorded comorbidity.1
Medical comorbidity dominated the recorded profile. Endocrine and metabolic diseases appeared in 62.5% of patients, cardiovascular diseases in 52.3%, orthopedic disorders in 50.0%, urogenital conditions in 43.0%, and autoimmune diseases in 37.5%. Psychiatric disease was recorded in 28.9%.
That mix helps explain why fibromyalgia cost control requires more than choosing cheaper pain medication. The resource burden is spread across rheumatology, endocrinology, physical therapy, pain medicine, internal medicine, emergency medicine, psychiatry, imaging, and laboratory testing.
Clinical implication: a patient with fibromyalgia, obesity or metabolic disease, cardiovascular risk, autoimmune symptoms, and persistent pain can move through many services before the care pathway becomes coherent. Spending then accumulates through workup intensity, fragmented specialty contact, and chronic prescriptions.
Antidepressants Were Common, But Drugs Were Not the Main Cost
Antidepressant prescribing in fibromyalgia usually reflects 2 overlapping roles: some antidepressants are used for pain modulation, and depression or anxiety symptoms are common in chronic pain populations. In the Saudi cohort, 77.3% of patients received antidepressants, representing 560 medication packs in the year.1
Other drug categories showed a broad pain-management footprint: 63.3% of patients received nonsteroidal anti-inflammatory drugs (NSAIDs), 51.6% received acetaminophen, 43.0% received anti-epileptic medications such as gabapentinoid-type pain drugs, and 25.8% received opioids.
The prescribing pattern is clinically relevant even though medication costs were low. Opioid exposure in 1 in 4 patients deserves scrutiny for a chronic pain syndrome where guidelines generally emphasize exercise, sleep, psychological skills, and selected non-opioid drugs over long-term opioid escalation.
Cost interpretation: low medication spending can coexist with high medication burden. Saudi public procurement and hospital pricing can make the accounting cost of drugs look small while the clinical burden of adverse effects, polypharmacy, dependence risk, and treatment failure remains substantial.
The Saudi Estimate Sits in the Lower-Middle of Global Direct-Cost Ranges
D’Onghia et al. reviewed 36 fibromyalgia cost-of-illness studies and found wide variation across countries, data sources, and cost categories. AlAujan et al. cited healthcare-perspective studies with annual direct costs ranging from USD 858 to USD 6,558 per patient, which puts the Saudi tertiary-hospital estimate of USD 2,560.3 inside the reported international range.2
Country-to-country substitution would be misleading because cost-of-illness studies are highly sensitive to what they count.
- Data source: medical records, claims, and patient surveys capture different slices of utilization.
- Perspective: healthcare-system costs are narrower than societal costs that include productivity loss.
- Service structure: referral patterns and diagnostic habits can move costs from primary care to specialty care or from drugs to testing.
- Medication pricing: procurement systems can shrink the accounting share of drug costs even when prescribing is common.
Gharibpoor et al. found high fibromyalgia illness costs in Iran and reported diagnostic testing as a major cost contributor from a societal perspective, which lines up with the Saudi signal that testing can be a serious regional cost driver.3 Lachaine et al., using Canadian data, found a more medication-heavy cost profile, especially around pain medications and antidepressants, showing how system structure changes the cost map.4
Severity and Productivity Loss Are the Missing Cost Layers
The biggest limitation is the missing severity layer. The Saudi study did not stratify patients by fibromyalgia severity, symptom impact, or work impairment.
Winkelmann et al. showed why that matters: patients with severe fibromyalgia had higher annual costs than patients with moderate or mild fibromyalgia in France and Germany, with a statistically significant severity-cost gradient in Germany (p = 0.003).5 Without a Fibromyalgia Impact Questionnaire score or comparable severity measure, the Saudi analysis cannot tell whether the cost burden was concentrated in the sickest subgroup.
Productivity loss is another missing layer. D’Onghia et al. found that indirect costs often exceed direct medical costs in fibromyalgia, and Lee et al. reported that productivity-loss costs in Japan were about 2.4 times greater in fibromyalgia patients than controls.2,6
Evidence-strength note: the Saudi study supports a descriptive claim about recorded direct medical costs in 1 tertiary hospital. It cannot estimate national fibromyalgia burden, prove that testing was excessive, identify causal drivers of utilization, or rank treatment strategies by cost-effectiveness.
What Saudi Fibromyalgia Planning Should Take From This
The strongest planning signal is service design. If nearly all recorded direct cost sits in specialist visits and diagnostic procedures, the most plausible efficiency gains will come from coordinated pathways, cleaner diagnostic protocols, and medication stewardship together.
- Standardize diagnostic pathways: clear fibromyalgia workup protocols can reduce repeated low-yield testing while still protecting against missed inflammatory, endocrine, neurologic, or autoimmune disease.
- Coordinate comorbidity care: metabolic, cardiovascular, orthopedic, autoimmune, psychiatric, and sleep-related problems need a shared plan so patients do not cycle through disconnected appointments.
- Track severity and function: adding symptom-severity and work-function measures would show whether resources cluster in high-burden patients who need more intensive multidisciplinary care.
- Audit opioid exposure: 25.8% opioid use deserves local review because chronic fibromyalgia management usually needs non-opioid, function-centered care as the default.
For readers, the practical message is narrower than “fibromyalgia is expensive.” In this Saudi hospital sample, the recorded medical cost was moderate by international standards, but the spending pattern points to a system problem: fibromyalgia care becomes expensive when uncertainty, comorbidity, and specialty fragmentation turn chronic pain into a long chain of visits, tests, and chronic prescriptions.
Questions About Fibromyalgia Costs in Saudi Arabia
Does this study prove fibromyalgia costs Saudi Arabia $2,560 per patient nationally?
No. USD 2,560.3 was the mean annual direct medical cost per patient in 1 governmental tertiary hospital in Riyadh. A national estimate would need more hospitals, primary-care data, private-sector data, pharmacy data, nonmedical costs, and productivity-loss data.
Why did medications account for only 3.7% of direct costs if antidepressants were prescribed to 77.3% of patients?
The study measured hospital-billing costs in a Saudi public-sector setting, where centralized procurement can keep medication prices low. Prescribing frequency and accounting cost are different signals: antidepressants were common, but specialist visits and diagnostic procedures were much more expensive in the recorded cost ledger.
Is the high laboratory-testing cost proof that patients were overtested?
No. The study did not judge whether specific tests were appropriate. The safer conclusion is that diagnostic procedures, especially laboratory testing, were a major cost component and should be audited against a standardized fibromyalgia diagnostic pathway.
What would make the next Saudi fibromyalgia cost study stronger?
A stronger study would include multiple centers, private and public care, fibromyalgia severity scores, work productivity, out-of-pocket spending, nonpharmacological care, and follow-up beyond 1 year. That design would separate routine direct medical cost from the broader economic burden patients actually experience.
References
- AlAujan SS, AlMazrou SH, AlNahedh HA, AlFalih LA, AlQahtani AM. Healthcare resource utilization and the direct medical cost of fibromyalgia patients in a tertiary hospital in Saudi Arabia. ClinicoEconomics and Outcomes Research. 2026;18:1-10. doi:10.2147/CEOR.S578039
- D’Onghia M, Ciaffi J, Ruscitti P, et al. The economic burden of fibromyalgia: a systematic literature review. Seminars in Arthritis and Rheumatism. 2022;56:152060. doi:10.1016/j.semarthrit.2022.152060
- Gharibpoor F, Nasrollahzadeh E, Ghavidel-Parsa B, Ghaffari ME, Bidari A. High cost of illness in fibromyalgia patients in Iran, irrespective of disease severity: a prospective cost study. International Journal of Rheumatic Diseases. 2021;24(5):671-680. doi:10.1111/1756-185X.14094
- Lachaine J, Beauchemin C, Landry PA. Clinical and economic characteristics of patients with fibromyalgia syndrome. Clinical Journal of Pain. 2010;26(4):284-290. doi:10.1097/AJP.0b013e3181cf599f
- Winkelmann A, Perrot S, Schaefer C, et al. Impact of fibromyalgia severity on health economic costs: results from a European cross-sectional study. Applied Health Economics and Health Policy. 2011;9:125-136. doi:10.2165/11535250-000000000-00000
- Lee LK, Ebata N, Hlavacek P, DiBonaventura M, Cappelleri JC, Sadosky A. Humanistic and economic burden of fibromyalgia in Japan. Journal of Pain Research. 2016;9:967-978. doi:10.2147/JPR.S110707