
A 2026 national survey of Dutch emergency physicians found wide variation in first-line medication choices for extreme agitation: without intravenous access, 34.7% preferred midazolam, 23.1% preferred droperidol, 14.3% preferred droperidol plus midazolam, and 10.4% preferred esketamine.1 The result is a practice map, not an outcome trial, but it shows how emergency clinicians are balancing rapid sedation, respiratory risk, and local protocol habits.
Research Highlights
- Midazolam led first-line use without IV access: 34.7% of Dutch emergency physicians selected midazolam when intravenous access was unavailable.
- Droperidol remained central: 23.1% selected droperidol alone and 14.3% selected droperidol plus midazolam without IV access.
- Ketamine-type rescue was common: when initial sedation was insufficient, 32.7% selected esketamine and 27.5% selected propofol as rescue options.
- Protocol habits shaped care: 43.0% cited a national pocket card as a reason for their preferred sedative, while 37.8% cited perceived effectiveness.
- Evidence strength is descriptive: the 251-response survey describes physician preferences and perceived practice; it cannot determine whether midazolam, droperidol, combination therapy, esketamine, or propofol produced the safest or fastest real-world sedation.
Extreme agitation is a severe behavioral emergency in which a person's motor activity, confusion, aggression, intoxication, psychosis, delirium, or medical instability can create immediate risk to the patient and staff. Chemical sedation means using medication to reduce dangerous agitation quickly enough to allow assessment, monitoring, cooling, oxygen support, or diagnostic workup.
Ouwerkerk et al. surveyed board-certified emergency physicians in the Netherlands about medication choices for extreme agitation.1 The 2026 cross-sectional survey analyzed 251 complete responses from 679 eligible physicians, a 37.0% completed-response rate, and received at least 1 response from all 59 Dutch hospitals with emergency physician-staffed EDs.
Midazolam, Droperidol, and Combination Sedation Dominated First-Line Choices
Midazolam is a benzodiazepine, a medication class that increases gamma-aminobutyric acid signaling and can rapidly reduce anxiety, agitation, muscle activity, and seizure risk. Its main acute danger is respiratory depression, especially when combined with alcohol, opioids, or other sedatives.
Droperidol is a dopamine-blocking antipsychotic used for agitation, nausea, and other acute-care indications. Its advantages in agitation are rapid calming and less direct respiratory suppression than benzodiazepines. Its risks include oversedation, extrapyramidal symptoms, and QT interval prolongation, a heart-rhythm marker that can become relevant in susceptible patients.
Without IV access, emergency physicians chose:
- Midazolam: 34.7%.
- Droperidol: 23.1%.
- Droperidol plus midazolam: 14.3%.
- Esketamine: 10.4%.
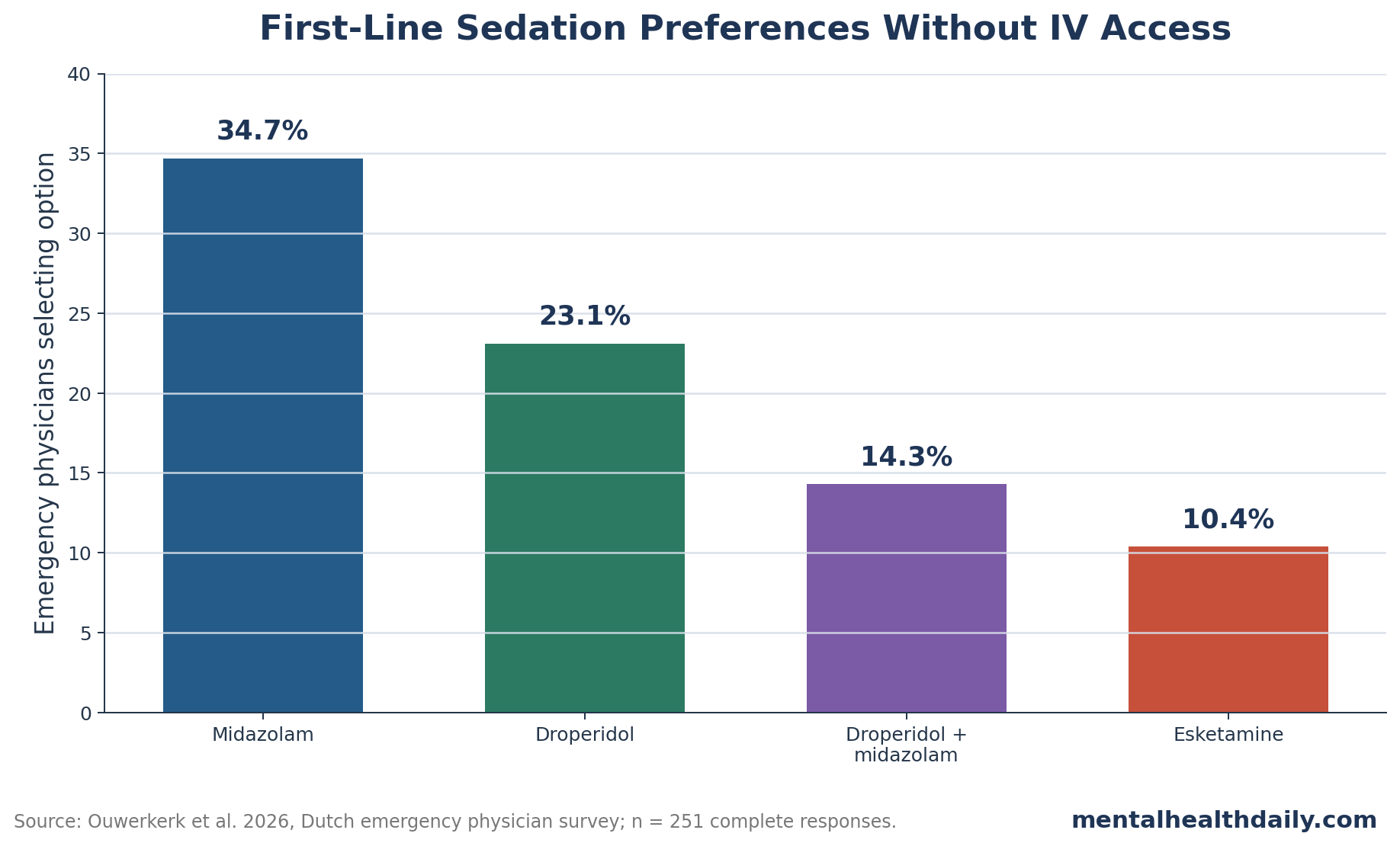
Intramuscular injection was the preferred route when IV access was unavailable. Median intramuscular doses were 10 mg for midazolam, 10 mg for droperidol, 5 mg plus 5 mg for droperidol-midazolam combination therapy, and 150 mg for esketamine.
Prehospital Midazolam Often Left an ED Decision Behind
The survey asked physicians how they perceived prehospital sedation before ED arrival. Among respondents, 39.0% reported that prehospital midazolam was often insufficient, 45.0% considered it sufficient, 9.6% considered it excessive, and 6.4% reported that no sedation had been given.
Clinical implication: the ED medication decision often begins after emergency medical services have already given a sedative. A patient who remains dangerously agitated after prehospital midazolam may need a different drug class, a higher cumulative dose, airway-aware monitoring, or treatment of a medical driver such as hypoxia, stimulant intoxication, head injury, infection, or hyperthermia.
Three influences shaped medication choice most often:
- Severity of agitation: 68.9% of physicians said severity affected sedative choice.
- Personal clinical experience: 58.2% reported that their own experience shaped the choice.
- Medication already given by emergency medical services: 53.4% considered the prehospital sedative when choosing the ED medication.
Medication sequence: droperidol and ketamine-type agents become relevant when benzodiazepine sedation is insufficient, risky, or already used before ED arrival.
Randomized and observational emergency-care studies have supported droperidol, midazolam-droperidol combinations, and ketamine pathways in different severe-agitation contexts, but studies differ in inclusion criteria, route, dose, rescue medication, and safety monitoring.234
Droperidol perception: respondents who used droperidol described it favorably. Among physicians who preferred droperidol, 87.2% cited effectiveness, 75.7% cited rapid onset, and 58.8% cited few side effects. Those are perceptions, not trial endpoints, but they fit the broader revival of droperidol after earlier concern about cardiac warnings made its use more cautious in some countries.
Protocol influence: the Dutch Society of Emergency Physicians pocket card was cited by 43.0% of respondents, while perceived effectiveness was cited by 37.8% and residency training by 30.3%. That mixture is realistic: emergency sedation practice is shaped by trial evidence, local availability, departmental culture, and what clinicians have seen work under pressure.
Rescue Sedation and Safety Planning Depend on Scenario
Rescue sequence: Most physicians, 85.7%, reported repeating the initial sedative up to a cumulative dose before switching medications. When switching was needed, 32.7% selected esketamine and 27.5% selected propofol.
Esketamine role: Esketamine is the S-enantiomer of ketamine, a dissociative anesthetic that blocks N-methyl-D-aspartate receptors and can rapidly separate consciousness from external stimulation. In severe agitation, ketamine-type agents can work quickly, but they require close monitoring because hypertension, hypersalivation, vomiting, laryngospasm, emergence reactions, and airway interventions can occur.
Propofol role: Propofol is an intravenous anesthetic that can produce deep sedation quickly. It is not a casual calming drug. It can cause hypotension and respiratory depression, so it belongs in monitored settings where airway support and resuscitation equipment are immediately available.
Evidence strength: Ouwerkerk et al. conducted a cross-sectional physician survey. The design can show what emergency physicians reported preferring, what protocols influenced practice, and where variation exists. It cannot compare patient-level time to sedation, intubation, oxygen desaturation, QT events, staff injury, need for redosing, or ED length of stay.
Implementation use: departments can compare their actual pathway against the distribution of national practice, then audit outcomes locally:
- time to calm enough for assessment
- respiratory events
- need for rescue sedation
- physical restraint duration
- staff injury
- whether patients received medical evaluation after sedation rather than being managed as a behavioral problem alone
Cause-specific risk: the survey result should not be read as a single national winner. Extreme agitation is a syndrome, not one disease. Alcohol intoxication, stimulant intoxication, psychosis, delirium, head trauma, hypoxia, sepsis, heat illness, serotonin toxicity, and withdrawal can all present with agitation, and those causes change medication risk.
Respiratory risk: benzodiazepines can be appropriate when seizure risk, stimulant toxicity, or withdrawal is plausible, but respiratory depression becomes more concerning when opioids, alcohol, or other sedatives are involved.
Cardiac risk: droperidol may be attractive when respiratory suppression is a major concern, but QT interval risk, electrolyte abnormalities, co-medications, and baseline cardiac disease can make monitoring more important.
Dissociation risk: ketamine or esketamine can be useful when immediate control is needed, but dissociation is a deeper sedation strategy. The airway, vomiting, blood pressure, and emergence-reaction plan needs to be ready before the injection, not improvised after the patient is calm.
Departmental pathways should force clinicians to name the likely cause, previous sedatives, route, monitoring level, rescue plan, and post-sedation medical evaluation. Medication choice without those details is an incomplete safety plan.
Monitoring implication: the medication is only one component of sedation quality. A pathway also needs vital-sign reassessment, oxygenation monitoring when feasible, temperature checks when stimulant toxicity or excited delirium-like presentations are possible, and a plan for glucose, trauma, infection, or withdrawal screening once the patient can be examined.
Documentation: recording the prehospital sedative, ED dose, route, time to adequate calming, adverse effects, and rescue medication lets departments learn from actual cases instead of relying only on preference surveys or memory of dramatic encounters.
Registry target: the next useful evidence layer would link medication sequence to patient-level outcomes. A national ED registry could capture initial cause category, prehospital sedation, route, redosing, oxygen or airway events, QT monitoring, restraint duration, staff injury, and whether occult medical illness was found after sedation. That would turn the survey's practice variation into a testable safety and effectiveness question.
After sedation, diagnosis still matters. A calm patient may have sepsis, hypoglycemia, trauma, serotonin toxicity, withdrawal, or intoxication that needs treatment beyond behavioral control.
The safety endpoint is complete medical care, beyond rapid calming alone.
Questions About Extreme Agitation Sedation
Which drug did Dutch emergency physicians choose most often without IV access?
Midazolam was the most common first-line choice without IV access, selected by 34.7% of respondents. Droperidol was second at 23.1%.
Does this prove midazolam is best?
No. The survey measured physician preference, not patient outcomes. A randomized trial or registry analysis would be needed to compare time to sedation and adverse events across medications.
Why combine droperidol and midazolam?
The combination uses 2 mechanisms: dopamine blockade from droperidol and gamma-aminobutyric acid enhancement from midazolam. The goal is faster or more reliable calming, with monitoring for oversedation and respiratory effects.
Why is esketamine usually treated differently?
Esketamine can produce rapid dissociative sedation, which can be useful in dangerous agitation. It also demands close monitoring because airway, cardiovascular, vomiting, and emergence-related complications can occur.
References
- National Survey of Dutch Emergency Physicians on Pharmacological Sedation Practices for Extreme Agitation. Ouwerkerk W et al. Toxicology Reports. 2026;14:102246. doi:10.1016/j.toxrep.2026.102246
- Improving the Management of Acutely Agitated Patients in the Emergency Department Through Implementation of Project BETA. Roppolo LP et al. JACEP Open. 2020;1(5):898-907. doi:10.1002/emp2.12138
- Pharmacological Treatment of Acute Agitation in the Emergency Department: A Network Meta-Analysis. deSouza IS et al. American Journal of Emergency Medicine. 2022;51:363-373. doi:10.1016/j.ajem.2021.11.011
- Randomized Controlled Trial of Intramuscular Droperidol Versus Midazolam for Violence and Acute Behavioral Disturbance. Isbister GK et al. Annals of Emergency Medicine. 2010;56(4):392-401. doi:10.1016/j.annemergmed.2010.05.037
- Midazolam and Droperidol for Acute Agitation in the Emergency Department. Knott JC et al. Annals of Emergency Medicine. 2006;47(1):61-67. doi:10.1016/j.annemergmed.2005.07.003
- Ketamine Versus Droperidol for Rapid Sedation of Agitated Patients in the Emergency Department. Taylor DM et al. Annals of Emergency Medicine. 2017;69(3):318-326. doi:10.1016/j.annemergmed.2016.07.033
- Ketamine as Rescue Treatment for Difficult-to-Sedate Severe Acute Behavioral Disturbance. Isoardi KZ et al. Emergency Medicine Australasia. 2021;33(6):987-992. doi:10.1111/1742-6723.13682