Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a disabling multisystem illness marked by post-exertional malaise, cognitive dysfunction, pain, sleep disruption, and autonomic symptoms; a 2026 PLOS One qualitative analysis of 505 memorial entries found that bereaved accounts repeatedly placed death inside 4 overlapping contexts: systemic neglect, clinical dismissal, social disconnection, and personal functional collapse.1
Research Highlights
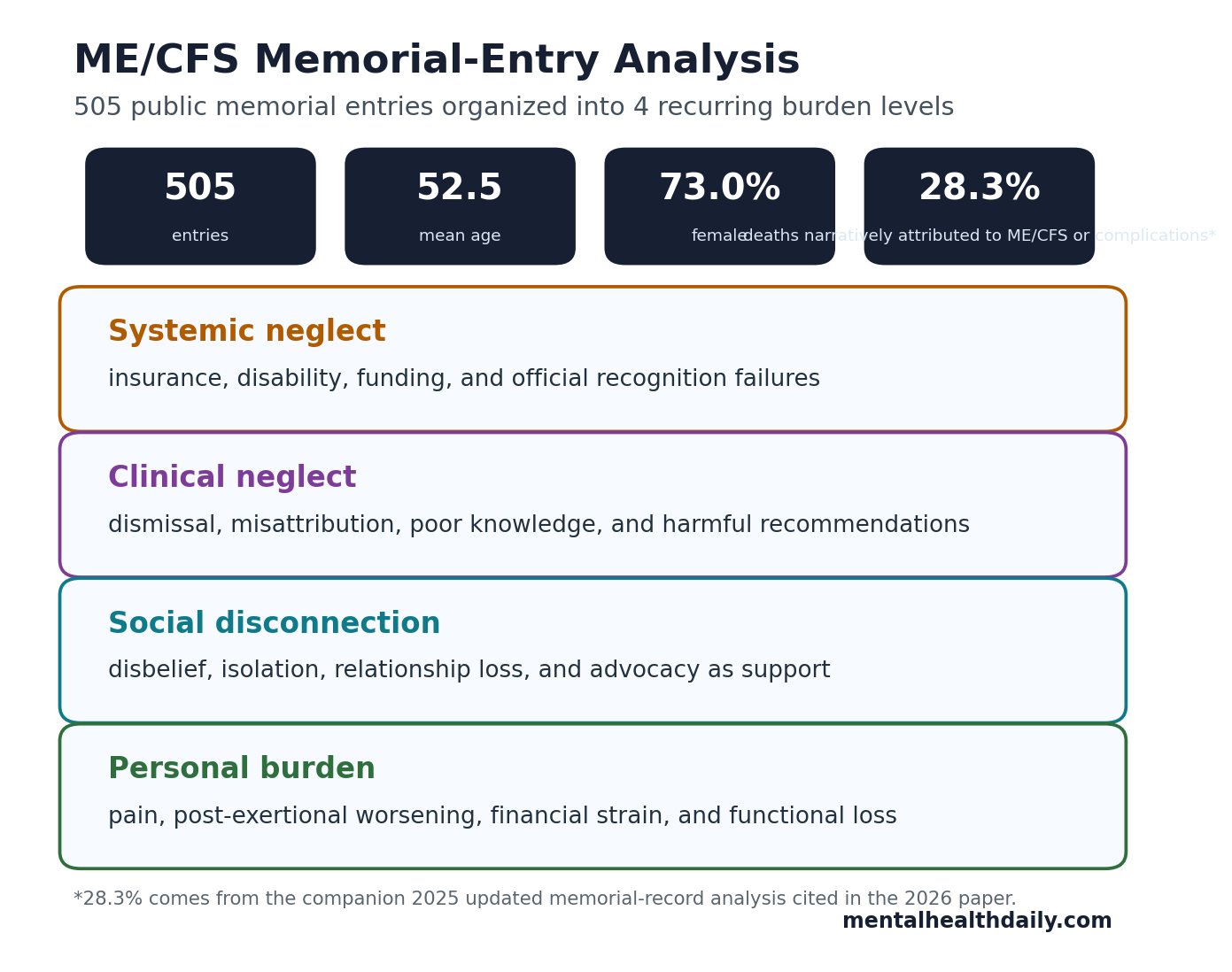
- 505 memorial entries were coded: Sirotiak et al. analyzed National CFIDS Foundation records downloaded in October 2024, with mean age at death of 52.5 years and an age range of 14 to 96 years.1
- 4 burden levels recurred: the main themes were systemic neglect, clinical neglect, social disconnection, and personal burden, not a single symptom-only account of illness.1
- Mortality framing changed: an updated companion analysis of the same 505-entry memorial corpus reported that 28.3% of deaths were narratively attributed to ME/CFS or its complications.2
- Functional loss was not abstract: the discussion cited prior ME/CFS literature estimating that up to 75% of affected people are unable to work and about 25% are consistently housebound or bedbound.1, 3
- Suicide risk needs direct screening: adjacent work on ME/CFS and chronic fatigue syndrome has treated suicide risk as a clinical safety issue with disease-specific drivers, including pain, disbelief, and functional loss.4, 5
Thematic analysis means researchers code narrative material for recurring meanings instead of reducing each entry to a single checkbox. In this case, 2 coders independently reviewed public memorial entries for people reported to have ME/CFS, developed a codebook, compared interpretations, and grouped the coded material into themes.
This design gives the paper a specific role: it cannot prove that ME/CFS caused an individual death, but it can show what bereaved relatives, friends, and acquaintances repeatedly described when they tried to explain the end of a life shaped by ME/CFS.
505 Memorial Entries Linked Death to More Than Symptoms
Sirotiak et al. analyzed 505 entries from the National CFIDS Foundation memorial list. The average age at death was 52.5 years (SD 16.7), 73.0% of entries described women, 68.9% were from North America, and 73.3% involved deaths in the 2000s or 2010s.1
Memorial entries are not medical charts: they are bereavement narratives. Some include age, sex, location, symptoms, functional status, cause of death, or clinical history; others emphasize anger, grief, advocacy, or unanswered questions. That makes the evidence emotionally dense but epidemiologically limited.
The strongest claim is pattern recognition: the same kinds of failures appeared across entries. People described disability and insurance battles, clinicians who dismissed symptoms as psychological, social relationships damaged by disbelief, and lives narrowed by pain, sensory intolerance, post-exertional worsening, financial stress, and loss of independence.
Systemic Neglect Was a Repeated Part of the Death Narrative
Systemic neglect means the failure sits above a single appointment: public agencies, disability systems, insurers, research funders, and diagnostic cultures fail to treat a condition as real, serious, and worthy of resources. In the memorial entries, this showed up as frustration with government recognition, insurance denial, disability fights, and underinvestment in ME/CFS research.1
That pattern fits earlier funding and disability literature. Mirin et al. had argued that ME/CFS disease burden was badly mismatched with US research funding, while disability-focused work has described how hard it can be to document ME/CFS impairment for benefits systems.6, 7
The 2026 paper adds a sharper mortality-context point: for some bereaved writers, institutional dismissal was not background frustration. It was part of how decline, isolation, and death were narrated.
Clinical Dismissal Can Become a Safety Problem
Clinical dismissal is more than a rude bedside interaction. In ME/CFS, it can mean missed diagnosis, delayed support, harmful advice, under-documentation of disability, and treatment recommendations that ignore post-exertional malaise, the symptom flare that follows physical, cognitive, or emotional exertion.
Sirotiak et al. found memorial entries describing misattribution of symptoms to psychological causes, clinicians who denied ME/CFS as a legitimate illness, death certificates that families questioned, and medical settings where staff appeared unfamiliar with severe ME/CFS.1
Adjacent healthcare-experience studies point in the same direction. McManimen et al. analyzed negative healthcare experiences in chronic illness and described dismissal as a recurring harm. Melby and Nair’s 2024 qualitative study of ME/CFS healthcare dissatisfaction also captured patients being left to manage an illness with few services and limited specialist knowledge.8, 9
- Diagnostic delay: people may spend years without a usable ME/CFS diagnosis, even while functioning declines.
- Wrong illness model: symptoms can be reframed as anxiety, depression, deconditioning, or personality rather than multisystem illness.
- Care avoidance: prior dismissal can make patients delay contact until pain, malnutrition, infection, or collapse becomes urgent.
- Safety blind spot: suicide risk can be missed when clinicians treat despair as a generic mood complaint instead of a response to pain, invalidation, disability loss, and lack of relief.
Social Disconnection Turned Illness Into Isolation
The memorial entries repeatedly described broken relationships, disbelief from family or friends, shrinking social contact, and reliance on support groups or advocacy spaces for validation.1 That is consistent with Boulazreg and Rokach’s review of loneliness, isolation, and alienation in ME/CFS, which framed social disconnection as part of the illness burden rather than a minor side effect.10
Stigma changes the risk environment: when relatives, clinicians, employers, or insurers do not believe the illness, the patient loses practical help and social confirmation at the same time. Severe symptoms then become harder to manage because basic pacing, disability documentation, home support, and emotional safety all depend on other people taking the disease seriously.
Advocacy appeared as a counterweight. Some entries described patients who educated clinicians, joined committees, built support groups, wrote online, donated money, or left their bodies for research. In the 2026 analysis, advocacy was not sentimental closure. It was often how people tried to make meaning inside a system that had not protected them.
Suicide Risk Should Be Asked About Directly in ME/CFS Care
The 2026 paper did not estimate suicide prevalence in the whole ME/CFS population, and it did not verify the cause of death for every memorial entry. Its value is narrower: suicide and possible suicide appeared in narratives that also mentioned pain, functional loss, hopelessness, social isolation, and medical dismissal.1
That pattern lines up with ME/CFS-specific suicide literature. Johnson et al. examined suicide risk factors in chronic fatigue syndrome, and Chu et al. argued that clinicians should identify and manage suicidality in ME/CFS as its own safety domain alongside comorbid depression.4, 5 Roberts et al.’s English clinical-record cohort also made suicide-specific mortality part of the ME/CFS safety discussion.11
Practical screening frame: suicide assessment in ME/CFS should ask about pain, post-exertional crashes, sleep loss, loss of work, food and hydration support, disability-benefit stress, disbelief at home, care refusal, and access to lethal means. A generic mood checklist can miss the disease-specific route by which risk builds.
This Evidence Is Powerful, But It Is Not Causal Mortality Proof
The design has built-in limits. The entries were public memorial narratives, usually written by acquaintances of the deceased. They are selected, retrospective, emotionally charged, and uneven in detail. A person appearing on the memorial list is not representative of all people with ME/CFS, and a family attribution cannot establish medical causality.1
What the study can support: bereaved accounts repeatedly described ME/CFS death through intertwined layers of illness, social disbelief, clinical dismissal, institutional neglect, pain, functional decline, and sometimes suicide.
What the study cannot support: a population-level suicide rate, an all-cause mortality rate, or a claim that ME/CFS directly caused every death described in the memorial corpus.
The calibrated read is still uncomfortable. If bereaved narratives keep describing the same failures around death, the right clinical response is not to dismiss the corpus because it is imperfect. The right response is to build care pathways that treat severe ME/CFS as a safety-relevant disability condition.
Questions About ME/CFS Memorial Entries and Suicide Risk
Do the 505 memorial entries prove ME/CFS causes early death?
No. The 2026 analysis was qualitative and based on public memorial entries, so it cannot estimate causal mortality risk. It shows that deaths were repeatedly narrated through ME/CFS-related disability, dismissal, social isolation, and systems failure.
Why include suicide in an ME/CFS article?
Because multiple ME/CFS studies and the 2026 memorial analysis put suicidality inside the illness burden. Pain, loss of function, disbelief, and lack of care can become direct safety concerns, even when depression is not the whole explanation.
What should clinicians do differently?
Clinicians should document functional impairment, ask about post-exertional malaise, avoid dismissive psychogenic explanations, screen directly for suicide risk, and ask whether the patient has food, hydration, caregiving, benefits, housing, and crisis support.
What should readers take from memorial-entry evidence?
Memorial entries are not neutral epidemiology, but they are not disposable anecdotes. They expose the social and clinical routes through which severe chronic illness can become dangerous.
References
- Sirotiak Z, Amro HJ. Investigating the ME/CFS experience through qualitative analysis of memorial entries. PLOS One. 2026;21(4):e0343374. https://doi.org/10.1371/journal.pone.0343374
- Sirotiak Z, Amro HJ. Mortality in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): an updated analysis of memorial records. Fatigue: Biomedicine, Health & Behavior. 2025;13(4):385-395. https://doi.org/10.1080/21641846.2025.2543201
- Bateman L, Bested AC, Bonilla HF, Chheda BV, Chu L, Curtin JM, et al. Myalgic encephalomyelitis/chronic fatigue syndrome: essentials of diagnosis and management. Mayo Clinic Proceedings. 2021;96(11):2861-2878. https://doi.org/10.1016/j.mayocp.2021.07.004
- Johnson ML, Cotler J, Terman JM, Jason LA. Risk factors for suicide in chronic fatigue syndrome. Death Studies. 2022;46(3):738-744. https://doi.org/10.1080/07481187.2020.1776789
- Chu L, Elliott M, Stein E, Jason LA. Identifying and managing suicidality in myalgic encephalomyelitis/chronic fatigue syndrome. Healthcare. 2021;9(6):629. https://doi.org/10.3390/healthcare9060629
- Mirin AA, Dimmock ME, Jason LA. Research update: the relation between ME/CFS disease burden and research funding in the USA. Work. 2020;66(2):277-282. https://doi.org/10.3233/WOR-203173
- Podell R, Dimmock ME, Comerford BB. Documenting disability in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Work. 2020;66(2):339-352. https://doi.org/10.3233/WOR-203178
- McManimen S, McClellan D, Stoothoff J, Gleason K, Jason LA. Dismissing chronic illness: a qualitative analysis of negative health care experiences. Health Care for Women International. 2019;40(3):241-258. https://doi.org/10.1080/07399332.2018.1521811
- Melby L, Nair RD. We have no services for you so you have to make the best out of it: a qualitative study of myalgic encephalomyelitis/chronic fatigue syndrome patients’ dissatisfaction with healthcare services. Health Expectations. 2024;27(1):e13900. https://doi.org/10.1111/hex.13900
- Boulazreg S, Rokach A. The lonely, isolating, and alienating implications of myalgic encephalomyelitis/chronic fatigue syndrome. Healthcare. 2020;8(4):413. https://doi.org/10.3390/healthcare8040413
- Roberts E, Wessely S, Chalder T, Chang CK, Hotopf M. Mortality of people with chronic fatigue syndrome: a retrospective cohort study in England and Wales from the South London and Maudsley NHS Foundation Trust Biomedical Research Centre. Lancet. 2016;387(10028):1638-1643. https://doi.org/10.1016/S0140-6736(15)01223-4