
A 2026 randomized trial in 63 adults with type 2 diabetes found that progressive muscle relaxation was linked to a large fatigue drop in the intervention group, from a Fatigue Severity Scale mean of 51.58 to 34.12, but adjusted between-group tests did not confirm a clear advantage over control for fatigue or sleep quality.1 The practical read is calibrated: relaxation practice looks like a reasonable low-risk fatigue support, not proof of a standalone sleep treatment for diabetes.
Research Highlights
- Fatigue dropped in the relaxation arm: 33 adults assigned to progressive muscle relaxation improved from 51.58 to 34.12 on the Fatigue Severity Scale (Z = −4.718; p = 0.000).1
- Control patients improved too: 30 adults in the control group improved from 44.50 to 30.60 on fatigue (Z = −4.396; p = 0.000), which weakens any simple “relaxation caused all improvement” claim.1
- Adjusted fatigue separation was not confirmed: after adjustment for baseline fatigue, posttest means were 33.18 vs. 31.64 and the between-group test was non-significant (F = 0.483; p = 0.490).1
- Sleep quality improved within groups: Pittsburgh Sleep Quality Index scores fell from 12.48 to 8.85 in the relaxation arm and from 9.67 to 6.67 in controls, but adjusted posttest sleep scores did not differ reliably (p = 0.621).1
- The best evidence target is fatigue support: prior diabetes and chronic-illness studies also point to fatigue or sleep benefits, but sample sizes and control conditions keep the evidence in an adjunct-care lane.2
Progressive muscle relaxation is a structured exercise in which a person deliberately tenses and then releases muscle groups, usually while slowing breathing and noticing the contrast between tension and release. The goal is not athletic conditioning; it is downshifting sympathetic arousal, the fight-or-flight physiology that can keep the body tense and sleep fragmented.
Symptom overlap: fatigue, poor sleep, glucose swings, depression, neuropathic symptoms, nocturia, medication effects, and stress all overlap in type 2 diabetes. A relaxation exercise can reduce tension and improve perceived rest, but it cannot by itself separate those mechanisms unless the trial design includes a strong comparator.
63 Insulin-Using Adults Tested 4 Weeks of Relaxation Practice
Vardar Inkaya et al. randomized adults with type 2 diabetes who were receiving outpatient endocrine care in Turkey. The trial assigned 33 people to progressive relaxation exercises and 30 to control care. Mean age was 57.97 years in the intervention arm and 58.47 years in the control arm.
The intervention was practical rather than technologically complex. Participants were shown how to do progressive relaxation exercises in clinic, then told to practice every night for 4 weeks with exercise videos. Control participants completed the same symptom measures and received the videos after the study period.
Two patient-reported outcomes carried the mental-health signal:
- Fatigue Severity Scale (FSS): a fatigue-impact measure where higher scores mean more severe fatigue.
- Pittsburgh Sleep Quality Index (PSQI): a sleep-quality measure where higher scores mean worse sleep; scores above 5 usually indicate poor sleep quality.
Baseline imbalance: the relaxation group started worse on both outcomes. Baseline PSQI was 12.48 in the relaxation group vs. 9.67 in controls (p = 0.002), and baseline fatigue was 51.58 vs. 44.50 (p = 0.034). That imbalance makes adjusted between-group results more important than simple before-after change.
Fatigue Improved, But the Control Group Also Moved
The strongest result was the within-group fatigue drop in the relaxation arm. FSS scores fell from 51.58 ± 9.08 to 34.12 ± 8.51 after 4 weeks. That is a large symptom movement in a small trial, and it matches the paper’s second hypothesis that relaxation exercises reduce fatigue.
Control participants also improved sharply, from 44.50 ± 13.34 to 30.60 ± 9.23. The authors discussed the Hawthorne effect, meaning behavior can change because participants know they are being observed. In diabetes, study contact can also make people monitor sleep, glucose, and self-care more carefully even without the active exercise.
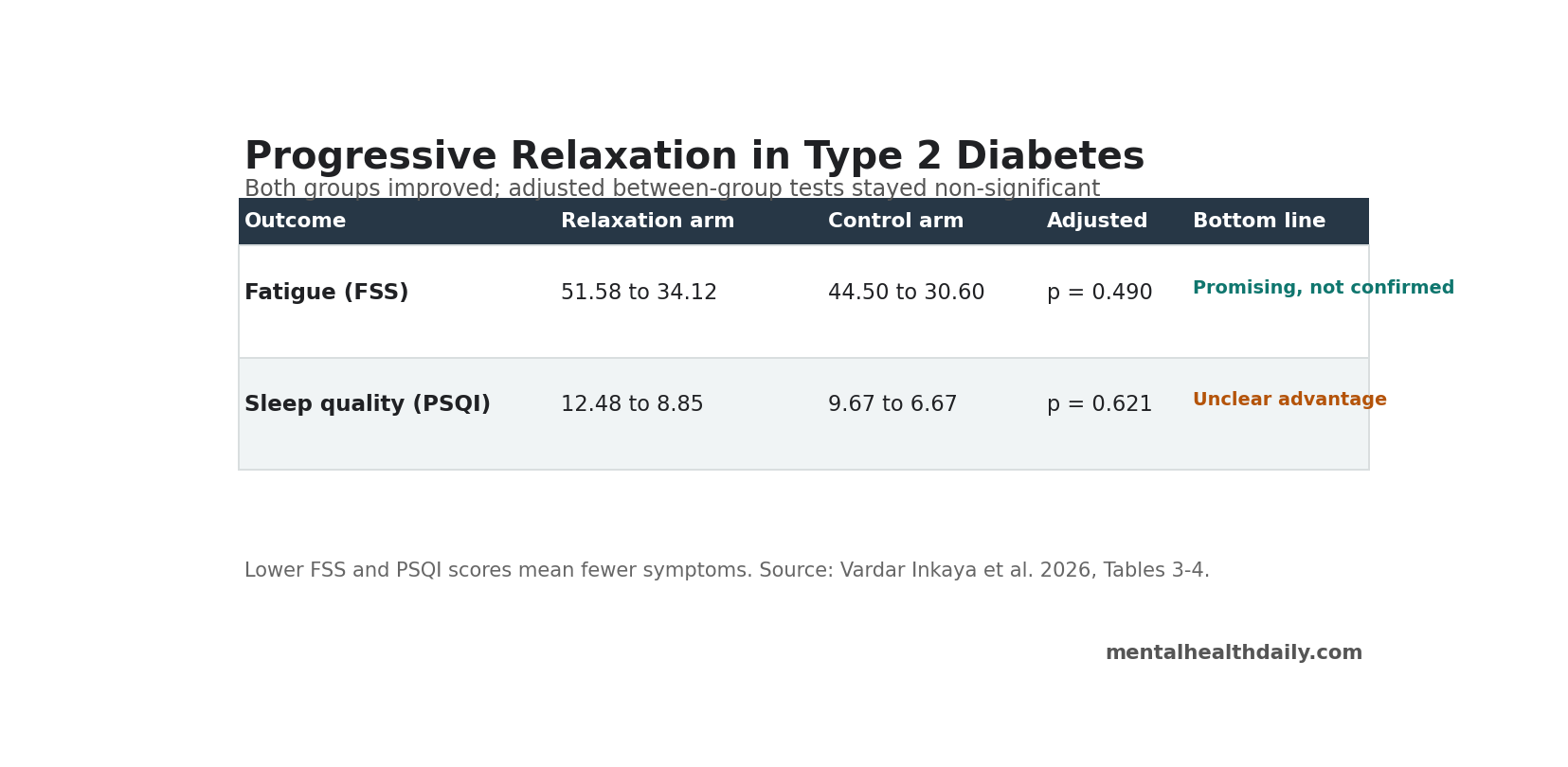
Adjusted comparison: after baseline fatigue was taken into account, adjusted posttest means were 33.18 for the relaxation arm and 31.64 for controls. The ANCOVA test was not statistically significant (F = 0.483; p = 0.490). That result does not erase the fatigue improvement, but it blocks a clean claim that relaxation clearly beat control care on fatigue in this study.
Sleep Quality Was the Weaker Claim
Sleep moved in the expected direction inside both arms. In the relaxation group, PSQI fell from 12.48 to 8.85 (Z = −4.593; p = 0.000). In the control group, PSQI fell from 9.67 to 6.67 (Z = −4.101; p = 0.000).
The between-group test did not confirm a sleep-quality advantage after baseline sleep quality was adjusted. Adjusted posttest means were 7.96 in the relaxation arm and 7.64 in controls (F = 0.247; p = 0.621). The paper’s own discussion states that the sleep-quality hypothesis was rejected.
Clinical interpretation: progressive relaxation may still help some patients sleep, especially when hyperarousal, muscle tension, worry, or bedtime stress are part of the problem. This trial just did not isolate a sleep effect beyond the control group’s improvement.
Prior Diabetes and COPD Trials Support Fatigue Plausibility
The diabetes-specific comparison is Izgu et al., a randomized clinical trial testing progressive muscle relaxation and mindfulness meditation in people with type 2 diabetes and neuropathic pain. That study reported fatigue improvement with progressive muscle relaxation, while mindfulness meditation did not show the same fatigue effect.2
Chronic respiratory disease trials point in a similar direction. Chegeni et al. reported that progressive muscle relaxation helped manage fatigue and sleep quality in chronic obstructive pulmonary disease (COPD), a condition where breathlessness, sleep disruption, and fatigue reinforce one another.3 Akgun and Dayapoglu also tested progressive relaxation in COPD and reported improvements in fatigue and sleep quality.4
Mechanism fit: Liu et al. tested progressive muscle relaxation in patients with COVID-19 and found benefits for anxiety and sleep quality.5 That evidence does not transfer perfectly to diabetes, but it supports a broader mechanism: relaxation training may be most useful when symptoms are partly maintained by arousal, threat monitoring, and poor restorative sleep.
Relaxation Is an Adjunct, Not a Diabetes Treatment
The trial also measured fasting glucose, postprandial glucose, and HbA1c. Both intervention and control groups improved on several glycemic measures, and the paper’s own tables show no clean posttest separation between groups for fasting glucose, postprandial glucose, or HbA1c.
Mechanism boundary: progressive muscle relaxation may reduce stress arousal, muscle tension, perceived fatigue, and bedtime activation. It should not be framed as a substitute for glucose monitoring, medication adjustment, nutrition, physical activity, neuropathy treatment, depression care, or sleep-apnea evaluation.
That distinction is especially important because diabetes fatigue can come from several sources:
- Metabolic instability: hyperglycemia, hypoglycemia, and glucose variability can produce exhaustion.
- Sleep disruption: nocturia, pain, restless legs, obstructive sleep apnea, and neuropathy can fragment sleep.
- Mood and stress load: depression, anxiety, and disease-management burden can amplify fatigue.
- Medication and comorbidity: polypharmacy, cardiovascular disease, kidney disease, and inflammation can all contribute.
A 4-week relaxation routine can sit inside that care plan, but it should not crowd out evaluation for treatable medical drivers of fatigue.
Small Trial, Baseline Imbalance, and No Attention Control Limit the Result
This was a randomized trial, which is a strength, but the evidence remains modest. The sample was small, single-center, and restricted to insulin-using adults who could perform the exercises. The trial was short, and durability after the 4-week practice period was not established.
Attention-control gap: control participants did not receive a matched nightly activity with the same contact, expectation, and self-monitoring structure. Without that comparator, it is hard to separate muscle relaxation from expectancy, observation, study participation, or general self-care attention.
Baseline imbalance: the relaxation group started with worse fatigue and worse sleep. Worse baseline scores can leave more room to improve, while regression to the mean can make large within-group changes appear even when between-group differences are weak.
Best use of the finding: progressive relaxation is a reasonable, cheap, low-risk add-on for diabetes fatigue when patients are interested and medically able to practice it. The stronger next trial would use a larger sample, an attention-control condition, sleep-apnea screening, depression measures, objective sleep tracking, and longer follow-up.
Questions About Progressive Muscle Relaxation and Diabetes Fatigue
Did progressive muscle relaxation reduce fatigue in this diabetes trial?
Fatigue fell substantially in the relaxation group over 4 weeks. The problem is that control participants also improved, and the adjusted between-group fatigue test was not significant. The fair conclusion is a promising fatigue-support signal, not definitive proof of superiority.
Did the trial prove a sleep-quality benefit?
No. PSQI scores improved inside both groups, but adjusted posttest sleep scores did not differ significantly. The study’s own conclusion treated the sleep hypothesis as rejected.
Who might reasonably try it?
Adults with type 2 diabetes who feel tense, stressed, wired at bedtime, or fatigued despite basic medical follow-up may reasonably try progressive muscle relaxation as an adjunct. It is not appropriate as a replacement for medical evaluation when fatigue is severe, new, worsening, or linked to glucose swings, shortness of breath, chest symptoms, depression, or sleep apnea.
How should it be practiced?
The tested intervention used nightly practice for 4 weeks after in-person instruction and video support. A practical version would use a guided audio or video routine, a consistent bedtime window, and symptom tracking so the patient can tell whether fatigue, sleep latency, or daytime functioning actually changes.
Why did controls improve too?
Study participation can change behavior. People may monitor their diabetes more carefully, pay more attention to rest, report symptoms differently, or improve because symptoms naturally fluctuate. That is why a matched attention-control group matters in future trials.
References
- The Effect of Progressive Relaxation Exercises Applied to Individuals With Type 2 Diabetes on Fatigue Level and Sleep Quality: A Randomised Controlled Study. Vardar Inkaya B et al. Scandinavian Journal of Caring Sciences. 2026;40:e70220. doi:10.1111/scs.70220
- Progressive Muscle Relaxation and Mindfulness Meditation on Neuropathic Pain, Fatigue, and Quality of Life in Patients With Type 2 Diabetes: A Randomized Clinical Trial. Izgu N et al. Journal of Nursing Scholarship. 2020;52:1-12. doi:10.1111/jnu.12580
- The Effect of Progressive Muscle Relaxation on the Management of Fatigue and Quality of Sleep in Patients With Chronic Obstructive Pulmonary Disease: A Randomized Controlled Clinical Trial. Chegeni PS et al. Complementary Therapies in Clinical Practice. 2018;31:64-70. doi:10.1016/j.ctcp.2018.01.010
- Effect of Progressive Relaxation Exercises on Fatigue and Sleep Quality in Patients With Chronic Obstructive Lung Disease (COPD). Akgun S and Dayapoglu NZ. Complementary Therapies in Clinical Practice. 2015;21(4):277-281. doi:10.1016/j.ctcp.2015.10.002
- Effects of Progressive Muscle Relaxation on Anxiety and Sleep Quality in Patients With COVID-19. Liu K et al. Complementary Therapies in Clinical Practice. 2020;39:101132. doi:10.1016/j.ctcp.2020.101132
- Relaxation Techniques as an Intervention for Chronic Pain: A Systematic Review of Randomized Controlled Trials. Vambheim SM et al. Heliyon. 2021;7(8):e07837. doi:10.1016/j.heliyon.2021.e07837