
A 2026 methylome-wide association study by Shen et al. found 48 CpG methylation sites tied to the quadratic CYP2C19 metabolizer-status term in 18,396 Generation Scotland participants, with 19 sites showing non-linear patterns and targeted replication in 1,238 older adults.1 That supports CYP2C19 as real biology beneath SSRI pharmacogenomics, but it does not prove universal antidepressant gene testing improves remission.
Research Highlights
- CYP2C19 methylation signals were genome-wide: Shen et al. tested 752,741 CpG sites, found 48 quadratic-term hits, and identified 19 non-linear CpGs where poor and ultra-rapid metabolizers diverged from normal metabolizers in related ways.1
- Drug-exposure effects are well-established. Jukic 2018, in 2,087 patients on escitalopram, found CYP2C19 poor metabolizers had roughly 3.3-fold higher serum concentrations than normal metabolizers, and ultra-rapid metabolizers had about 2-fold lower concentrations. Both extremes had elevated rates of treatment switching.3
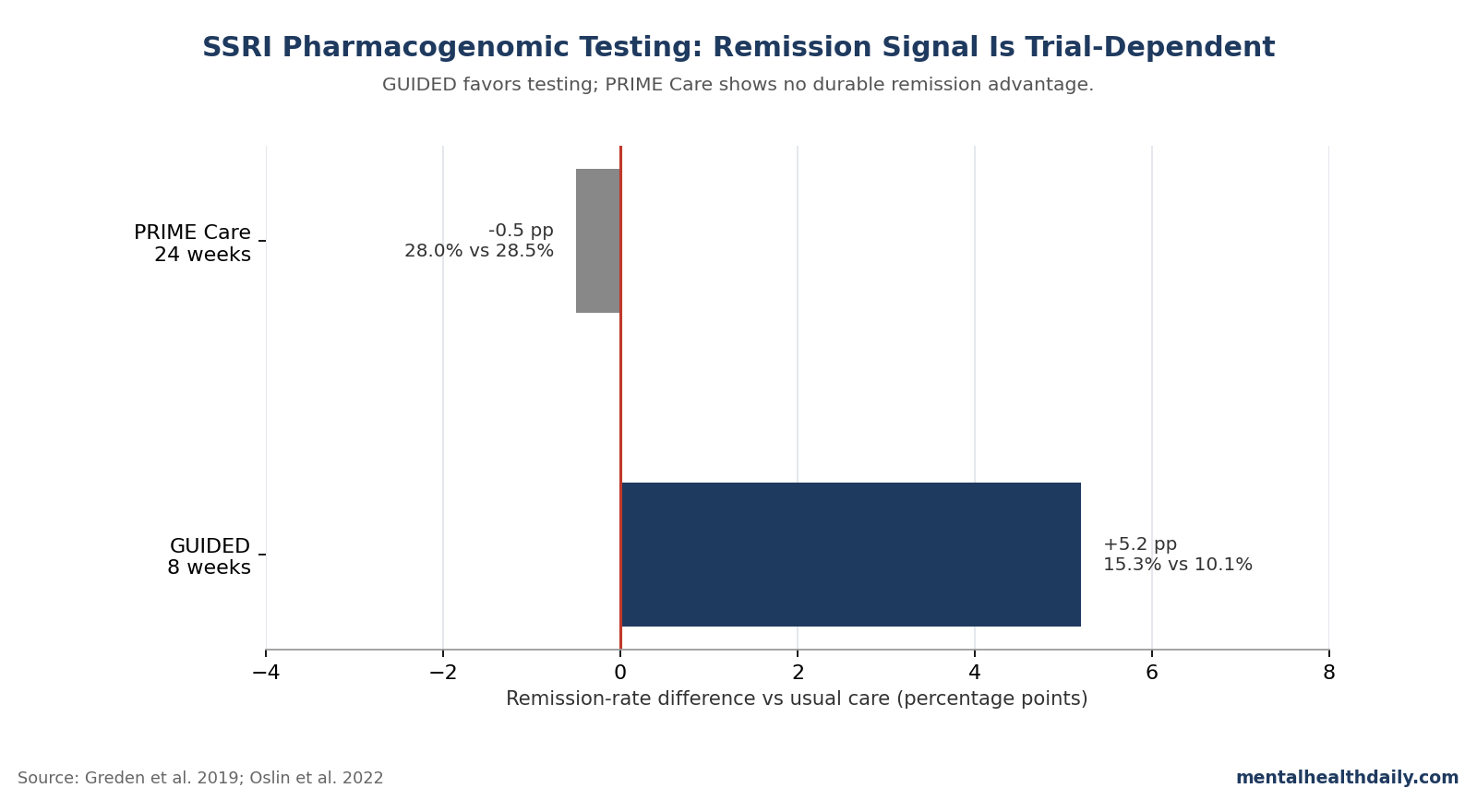
- The two flagship RCTs disagree. GUIDED (Greden 2019, n=1,167) reported 15.3% vs 10.1% remission at 8 weeks for testing-guided vs treatment-as-usual care — statistically significant on secondary endpoints but missing the primary endpoint. PRIME Care (Oslin 2022, VA, n=1,944) found no remission difference (28.0% vs 28.5%) at 24 weeks.4,5
- CPIC guidelines (Bousman 2023) recommend dose adjustments or alternative agents for known poor or ultra-rapid metabolizers on specific SSRIs, but stop short of recommending universal pre-prescription testing.6
- Clinical use is narrower than marketing: the strongest fit is a patient with 2 or more failed SSRIs or unusual side effects, not routine testing before a first prescription.
Commercial tests often collapse 2 claims into one: variants alter SSRI exposure, and testing improves depression outcomes. The first claim is strong; the second is trial-dependent.
Shen 2026 adds a third layer by showing that CYP2C19 metabolizer status also tracks with DNA methylation, including inflammation, lipid, and antidepressant-response loci, in ways that are not always linear.
What CYP2D6 and CYP2C19 Actually Do
Most antidepressants are processed in the liver by enzymes from the cytochrome P450 family. Two enzymes carry the bulk of the SSRI load: CYP2D6 handles paroxetine and fluoxetine, and CYP2C19 handles citalopram, escitalopram, and sertraline.2
Genetic variants change how much enzyme a person produces and how active it is. Five phenotype categories are standard:
- Poor metabolizers — two non-functional alleles, very low enzyme activity, drug clears slowly, plasma levels run high.
- Intermediate metabolizers — one non-functional and one decreased or normal allele, reduced activity.
- Normal metabolizers — the reference category, two functional alleles.
- Rapid metabolizers — one increased-activity allele.
- Ultra-rapid metabolizers — two increased-activity alleles, drug clears fast, plasma levels run low.
Population frequencies depend on ancestry. About 2–5% of European-ancestry populations are CYP2C19 poor metabolizers; East Asian populations are closer to 13–23%.
Ultra-rapid CYP2C19 metabolizers carrying CYP2C19*17 run roughly 4–5% in Europeans.2
Jukic 2018: Direct Evidence That Phenotype Maps to Plasma Levels
The clearest single-paper demonstration that CYP2C19 metabolizer status changes SSRI exposure comes from Jukic et al. in 2,087 escitalopram-treated patients in Norway.3
Compared with normal metabolizers, poor metabolizers had about 3.3-fold higher dose-adjusted escitalopram serum concentrations, and ultra-rapid metabolizers had roughly 2-fold lower concentrations. Both groups had elevated rates of treatment switching: poor metabolizers were more likely to switch because of side effects, ultra-rapid metabolizers because of inadequate response.
This is the part of the pharmacogenomics story that is genuinely settled. CYP2C19 genotype changes plasma levels of escitalopram and citalopram by clinically meaningful magnitudes, and the curve is roughly bidirectional — opposite directions of effect at the two extremes.
Less settled is whether translating that exposure information into a prescribing decision produces better outcomes than structured follow-up with dose adjustment or medication switching based on response.
GUIDED Was Modestly Positive; PRIME Care Was Not
Two large randomized trials tested whether pharmacogenomic-guided antidepressant selection improves depression outcomes. They reached different conclusions.
GUIDED (Greden 2019). A multi-site, raters-blinded RCT in 1,167 adults with major depressive disorder who had failed at least one prior antidepressant. Patients were randomized to receive treatment guided by GeneSight (a commercial combinatorial pharmacogenomic test combining variants in CYP2D6, CYP2C19, CYP1A2, SLC6A4, and HTR2A) or treatment as usual.
The pre-specified primary endpoint — symptom improvement at 8 weeks (HAM-D17) — was not met (27.2% vs 24.4%, not statistically significant). Two secondary endpoints did separate: response (50% symptom reduction) at 26.0% vs 19.9%, and remission at 15.3% vs 10.1%.4
The framing of GUIDED as “positive” depends on how much weight you give the secondary endpoints when the primary missed. In drug-trial regulatory framing this would be considered a failed trial; in clinical-utility framing the response and remission separations are real and roughly the size of a moderate antidepressant effect.
PRIME Care (Oslin 2022, JAMA). A larger pragmatic RCT in 1,944 Veterans Affairs patients starting a new antidepressant. Patients were randomized to clinicians having the pharmacogenomic test report at baseline or 24 weeks later.
The primary endpoint — remission at 24 weeks — showed essentially no difference (28.0% vs 28.5%). A small short-term reduction in prescription of agents flagged as “use with caution” was observed early but didn’t translate to outcome differences.5
PRIME Care is larger, longer, more pragmatic, and ran in a system where prescribers had real autonomy over how to act on test results. It’s the trial pharmacogenomic-testing advocates least like to discuss in marketing.
Why the Two Trials Diverge
Several structural differences plausibly explain the disagreement.
- Patient population. GUIDED enrolled patients who had already failed at least one antidepressant; PRIME Care enrolled patients starting a new antidepressant including many treatment-naive cases. Pharmacogenomic information may add more value in treatment-resistant cases where simple dose-titration has already been tried.
- Care setting. The VA system has integrated pharmacy, structured medication review, and standardized prescribing protocols. Routine VA care already does much of what pharmacogenomic testing is supposed to add — flagging high-dose risk, attending to drug interactions, encouraging follow-up — which compresses any incremental benefit from testing.
- Endpoint and follow-up. GUIDED’s 8-week endpoint catches early differential response; PRIME Care’s 24-week endpoint allows usual-care patients to switch agents based on observed response, which closes the outcome gap.
- Test composition. GUIDED used a multi-gene combinatorial algorithm (GeneSight) whose proprietary weighting of variants isn’t fully transparent; PRIME Care reported individual variants. Combinatorial outputs can suggest specific agents in ways that simple variant lists don’t.
The honest read is that neither trial cleanly settles the question. GUIDED suggests testing helps modestly in already-treated patients on shorter-term endpoints; PRIME Care suggests testing doesn’t change outcomes when usual care is reasonably good and follow-up is long enough for empirical adjustment. Both can be true.
Shen 2026: CYP2C19 Reshapes DNA Methylation Genome-Wide, Often Non-Linearly
The Shen 2026 paper isn’t a clinical trial. It’s a methylome-wide association study (MWAS) — a screen testing whether CYP2C19 metabolizer status (poor through ultra-rapid) is associated with DNA methylation levels at every measured CpG site across the genome.1
What MWAS does is ask whether a genetic factor leaves a fingerprint on the broader epigenome — on the chemical tags that control which genes get expressed in which tissues. If CYP2C19 only affected drug clearance, you’d expect methylation effects clustered tightly on chromosome 10 near the CYP2C19 gene itself.
If CYP2C19 activity has wider biological consequences, you’d expect methylation effects scattered across the genome at biologically meaningful sites.
The Shen findings:
- 48 CpG sites significantly associated with the quadratic (non-linear) term of metabolizer status (Bonferroni-corrected, P < 6.64 × 10−8).
- Of those, 19 sites showed a U-shaped or inverted-U-shaped pattern — methylation differed in the same direction at both poor and ultra-rapid extremes relative to normal metabolizers. These sites are annotated to genes including TBC1D12, PDLIM1, ACSM6, and CYP2C18.
- Replication in the Lothian Birth Cohorts (n=1,238) showed correlation r=0.92 for the quadratic term and r=0.89 for the linear term between discovery and replication effect sizes. 18 of 20 quadratic-term CpGs had directionally consistent effects in replication.
- Several non-linear CpGs are in pathways relevant to depression biology — CRP and inflammation, type 2 diabetes, lipid levels, and antidepressant response (genes GRIK2, LOC283867).
- The methylation effects were not driven by medication use. Interactions between metabolizer status and use of CYP2C19-metabolized drugs were non-significant after FDR correction. The methylation pattern reflects the metabolizer status itself, not the drugs the person happens to be on.
The clinical implication of the non-linearity is the part that complicates the simple testing pitch. If poor and ultra-rapid metabolizers both show altered methylation at inflammation- and antidepressant-related loci — even though their drug-exposure curves point in opposite directions — then the “match drug to metabolizer” logic isn’t capturing the full biology.
There may be shared downstream consequences of metabolizer-status extremes that aren’t predicted by exposure pharmacokinetics alone.
What CPIC Guidelines Actually Recommend
The Clinical Pharmacogenetics Implementation Consortium (CPIC) issues evidence-graded guidelines for pharmacogenomic-informed prescribing. The 2023 update for SSRIs (Bousman et al.) covers CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A.6
For known CYP2C19 poor metabolizers on citalopram or escitalopram, CPIC recommends a 50% dose reduction or selecting an alternative agent. For ultra-rapid metabolizers, CPIC recommends considering an alternative agent because of the risk of inadequate response at standard doses.
Similar phenotype-specific recommendations exist for CYP2D6-metabolized agents like paroxetine and fluvoxamine.
Critically, CPIC’s recommendations are conditional: if a genotype is known, here’s what to do. CPIC does NOT recommend universal pre-prescription pharmacogenomic testing for SSRIs.
The level-of-evidence grade for the dose-adjustment recommendations is generally moderate (B), based mostly on pharmacokinetic data rather than head-to-head outcome trials.
This is the meaningful distinction between “variants matter for exposure” (CPIC says yes, with evidence) and “testing changes outcomes” (CPIC declines to make a universal recommendation, because the evidence base is mixed).
Where Pharmacogenomic Testing Is Most and Least Useful
The calibrated read of the evidence has three parts.
- Best-fit patients: multiple prior SSRI failures or unexplained severe side effects. If a patient has tried two or more antidepressants without response, or had unusually severe side effects on a standard dose, a known poor- or ultra-rapid-metabolizer phenotype helps explain the pattern and constrains agent selection. CPIC dose-adjustment guidance has the most clinical traction in this scenario. The Campos 2022 Australian Genetics of Depression Study (n=9,500) found that CYP2C19 poor metabolizers had higher SSRI efficacy but greater intolerance, while rapid metabolizers had better tolerability — consistent with the exposure-mediated mechanism.7
- Mixed signal: first-line antidepressant selection in treatment-naive patients. The PRIME Care null result is most relevant here. If a treatment-naive patient is starting their first SSRI, the marginal benefit of pre-testing over standard care with structured follow-up is small in pragmatic settings. The empirical strategy — start a first-line agent, monitor response and side effects at 4–6 weeks, adjust based on what happens — works reasonably well.
- Least useful: as a marketing-driven add-on for patients already responding well. If a patient is doing well on their current antidepressant, retroactive genotyping is unlikely to change management. The test result will report variants the patient already has, but it can’t override the empirical evidence that the current drug is working at the current dose.
Limitations of the Current Pharmacogenomic-Testing Evidence
Trials of testing-guided care can’t fully blind clinicians. Once a clinician has a test report saying “use with caution” for an agent, they’re not blinded to the recommendation. This makes outcome differences hard to interpret cleanly — placebo-like effects of having structured guidance can drive part of the modest benefit seen in some trials.
Combinatorial commercial tests aren’t fully transparent. GeneSight, Genomind, and similar tests use proprietary algorithms to combine multiple variants into agent-by-agent recommendations. The exact weightings aren’t published.
This makes external replication difficult and means trials of one commercial test don’t necessarily generalize to another.
Most evidence is European-ancestry. The Shen MWAS, GUIDED, and most CPIC guideline-supporting studies enrolled predominantly European-ancestry participants. CYP2C19 and CYP2D6 allele frequencies vary substantially by ancestry, and the clinical effect of genotype on outcome may also differ.
Generalizability to non-European populations is genuinely unknown for most of the recommendations.
Outcome-vs-exposure conflation in marketing. Direct-to-consumer pharmacogenomic-testing marketing often cites pharmacokinetic studies (Jukic-style exposure differences) as evidence that testing improves outcomes, then cites outcome-trial data (GUIDED-style) at headline-only level. The honest scientific story requires both: variants affect exposure (well-established) and exposure differences don’t fully translate into outcome differences (the trials are mixed).
Testing economics distort the evidence base. Most of the larger pharmacogenomic-testing RCTs have been industry-sponsored or industry-supported. PRIME Care, run in the VA without industry sponsorship, is the largest fully independent trial, and it’s the most negative.
This pattern is worth weighing when reading meta-analyses dominated by sponsored trials.
Questions About SSRI Pharmacogenomic Testing
What does “CYP2C19 poor metabolizer” mean for an SSRI?
It means the person carries two low-function copies of CYP2C19. Drugs metabolized by that enzyme — especially citalopram and escitalopram — clear slowly, so standard doses can produce roughly 3-fold higher plasma levels than in normal metabolizers.3
Should testing happen before a first antidepressant?
Usually no. PRIME Care found no remission difference at 24 weeks, and testing has more potential value after 2 or more antidepressant failures, unexplained severe side effects, or a strong family pattern of non-response.5
Does GeneSight actually improve remission?
GUIDED missed its primary symptom-improvement endpoint but showed modest secondary remission and response gains at 8 weeks. That is reasonable evidence for a small benefit in treatment-experienced patients, not strong evidence for testing every depression patient before any prescription.4
Why did GUIDED and PRIME Care reach different conclusions?
GUIDED studied treatment-experienced patients over 8 weeks; PRIME Care studied a pragmatic VA population over 24 weeks. Shorter follow-up and prior antidepressant failure give testing more room to look useful, while longer structured usual care lets clinicians adjust empirically.
If I’m an ultra-rapid metabolizer, should I avoid SSRIs?
Not necessarily. CPIC recommends considering alternatives or dose adjustments for ultra-rapid CYP2C19 metabolizers on citalopram or escitalopram; the result informs agent selection rather than ruling out the whole SSRI class.6
Does the Shen methylation finding change prescribing now?
No immediate change follows from it. Shen 2026 shows that CYP2C19 metabolizer status is linked to genome-wide methylation patterns, including non-linear signals at the metabolizer extremes, but it does not test whether a different SSRI choice improves remission.1
References
- Shen C, Adams MJ, Davyson E, Iveson MH, Cox SR, Harris SE, McIntosh AM, Shen X. The non-linear and linear effects of CYP2C19 metaboliser status on DNA methylation: a methylome-wide association study. Clin Epigenet. 2026. doi:10.1186/s13148-026-02125-w
- Hicks JK, Bishop JR, Sangkuhl K, Müller DJ, Ji Y, Leckband SG, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin Pharmacol Ther. 2015;98(2):127–134. doi:10.1002/cpt.147
- Jukić MM, Haslemo T, Molden E, Ingelman-Sundberg M. Impact of CYP2C19 Genotype on Escitalopram Exposure and Therapeutic Failure: A Retrospective Study Based on 2,087 Patients. Am J Psychiatry. 2018;175(5):463–470. doi:10.1176/appi.ajp.2017.17050550
- Greden JF, Parikh SV, Rothschild AJ, Thase ME, Dunlop BW, DeBattista C, et al. Impact of pharmacogenomics on clinical outcomes in major depressive disorder in the GUIDED trial: a large, patient- and rater-blinded, randomized, controlled study. J Psychiatr Res. 2019;111:59–67. doi:10.1016/j.jpsychires.2019.01.003
- Oslin DW, Lynch KG, Shih MC, Ingram EP, Wray LO, Chapman SR, et al. Effect of Pharmacogenomic Testing for Drug-Gene Interactions on Medication Selection and Response in Patients With Depression: The PRIME Care Randomized Clinical Trial. JAMA. 2022;328(2):151–161. doi:10.1001/jama.2022.9805
- Bousman CA, Stevenson JM, Ramsey LB, Sangkuhl K, Hicks JK, Strawn JR, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A Genotypes and Serotonin Reuptake Inhibitor Antidepressants. Clin Pharmacol Ther. 2023;114(1):51–68. doi:10.1002/cpt.2903
- Campos AI, Byrne EM, Mitchell BL, Wray NR, Lind PA, Licinio J, et al. Impact of CYP2C19 metaboliser status on SSRI response: a retrospective study of 9500 participants of the Australian Genetics of Depression Study. Pharmacogenomics J. 2022;22(2):130–135. doi:10.1038/s41397-022-00269-5
- Cipriani A, Furukawa TA, Salanti G, Chaimani A, Atkinson LZ, Ogawa Y, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
- Brown LC, Stanton JD, Bharthi K, Maruf AA, Müller DJ, Bousman CA. Pharmacogenomic Testing and Depressive Symptom Remission: A Systematic Review and Meta-Analysis of Prospective, Controlled Clinical Trials. Clin Pharmacol Ther. 2022;112(6):1303–1317. doi:10.1002/cpt.2748