
A 2026 preprint involving 31 children and adolescents treated for medulloblastoma found that silent verb-generation fMRI separated pre- from post-radiotherapy scans with 80.7% leave-one-subject-out accuracy (p = 0.0149).1 The signal points to early cerebellar-cerebral language-network change, not yet to a proven long-term cognitive endpoint.
Research Highlights
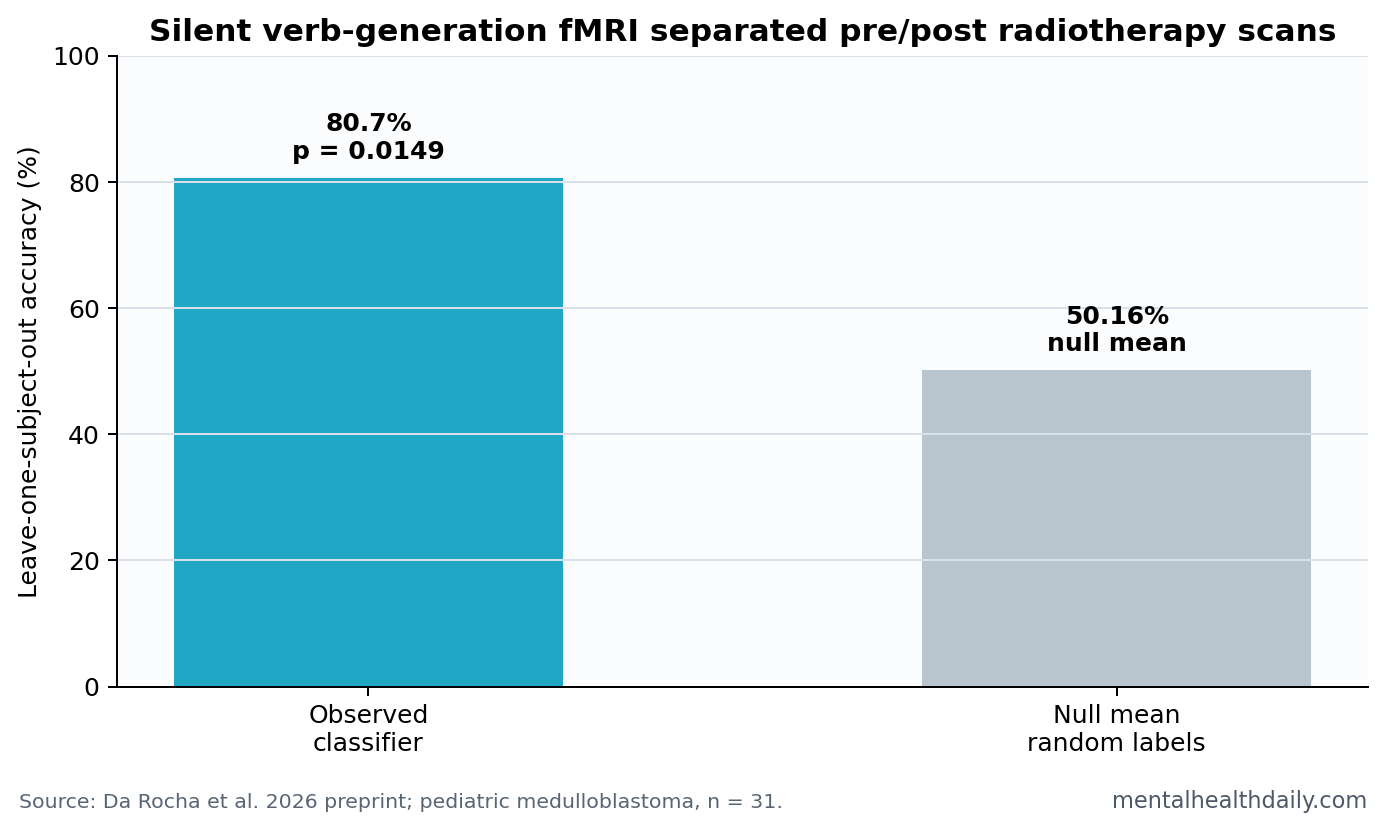
- Classifier performance was above chance: A linear support-vector machine separated pre- vs. post-radiotherapy fMRI scans with 80.7% accuracy, compared with a null mean of 50.16% (p = 0.0149).1
- Cerebellar-language circuits changed: Reduced activity appeared in Crus I/II and cerebellar lobules VI-VIII, regions increasingly tied to language and executive control.1
- Frontal and insular language regions decreased: Left inferior frontal gyrus, left insula, left putamen, anterior cingulate, and left middle temporal gyrus all contributed to the post-radiotherapy pattern.1
- Parietal recruitment increased: Left supramarginal and inferior parietal engagement rose, suggesting possible compensatory verbal-attention or phonological-rehearsal support.1
- Outcome proof is still missing: Only 8 participants had complete five-timepoint exploratory trajectories, and the paper measured early imaging change rather than long-term school or language outcomes.1
Silent verb generation is an fMRI task in which a person sees or hears a noun and silently thinks of a related verb. It activates language-production, working-memory, and cognitive-control circuits without requiring overt speech inside the scanner.
Da Rocha et al. used that task before and shortly after radiotherapy in children and adolescents with medulloblastoma, a pediatric brain tumor often treated with surgery, chemotherapy, and craniospinal irradiation.
31 Pediatric Medulloblastoma Patients Completed Pre/Post fMRI
The cohort included 31 children and adolescents, 18 of them male, with mean age 14.1 +/- 4.7 years. Participants completed visual and auditory noun-cued covert verb generation during fMRI before radiotherapy and within 6 weeks after radiotherapy.1
Medulloblastoma survivorship is clinically important because survival gains can come with neurocognitive costs. Language, processing speed, executive function, working memory, and school performance can all be vulnerable after treatment.
80.7% Accuracy Marked a Distributed Post-Radiotherapy Signature
The machine-learning result was the headline number. A linear support-vector machine classified pre- vs. post-radiotherapy scans with 80.7% leave-one-subject-out accuracy. Under randomized labels, mean null accuracy was 50.16%, with a 95% CI from 29.03% to 72.58%, and the observed result was significant at p = 0.0149.1
Leave-one-subject-out accuracy means the model repeatedly trained on all but one participant and tested the left-out participant. That design helps preserve within-person structure, but in a 31-person preprint it still needs replication.
The optimal feature-selection threshold was 70% sign consistency. Accuracy rose from 61% at a looser threshold to 80.7% at the 70% threshold, then dropped when the feature set became too restrictive.1
Cerebellar and Frontal Language Regions Lost Activation
Reduced post-radiotherapy activity appeared in bilateral cerebellar hemispheres, especially Crus I/II and lobules VI-VIII. Those regions support more than motor control. Modern language neuroscience increasingly treats them as parts of cerebellar-cerebral loops involved in sequencing, prediction, lexical retrieval, and executive control.23
Reduced activity also appeared in left inferior frontal gyrus and anterior insula, regions involved in lexical retrieval and articulatory planning, plus left putamen, anterior cingulate, and left middle temporal gyrus.1
Clinical interpretation: lower fMRI activation does not automatically mean permanent damage. It shows that the task-evoked network changed after radiotherapy in a way a classifier could detect.
Left Supramarginal and Inferior Parietal Activity Increased
The opposite-direction signal came from parietal regions. Left supramarginal and inferior parietal activation increased after radiotherapy.1 Those regions support phonological buffering, attentional control, and covert speech rehearsal.
One plausible reading is compensation: when core cerebellar, frontal, insular, and cingulate components show reduced task response, parietal working-memory support may increase. That interpretation is plausible, not proven, because the study did not show that increased parietal activity protected language outcomes.
The auditory and visual task design also matters. Children generated verbs from spoken nouns and visually presented nouns, which means the signature was not tied to one sensory format. A network that changes across both cue types is more likely to reflect language-control circuitry than a simple visual or auditory processing artifact.
Patient-level use: the paper’s classifier was built to separate scan timepoints, not to make an individual prognosis. A future clinical tool would need to predict which child develops language, reading, working-memory, or classroom problems and which support reduces that risk.
The most actionable targets are concrete: lexical retrieval therapy, phonological rehearsal support, working-memory scaffolding, and school accommodations that reduce language-processing load during treatment recovery. Those interventions still need outcome-linked testing.
Age also complicates interpretation. A 14-year-old brain is still developing language, executive-control, and academic skills. Radiotherapy may interact with normal developmental change, chemotherapy, fatigue, missed school, hearing changes, and emotional stress after cancer treatment. fMRI can point to network disruption, but survivorship care has to measure cognition in daily life.
Measurement timing: the scan window was early, within 6 weeks after radiotherapy, so the result should be read as a treatment-timing marker rather than a final late-effects measurement. Some early activation changes may recover, some may persist, and some may predict later difficulty only when paired with dose exposure, chemotherapy intensity, baseline cognition, and school functioning.
That distinction protects the useful signal from being oversold.
Outcome bridge: the next step is pairing the same fMRI signature with neuropsychological testing. If children with larger cerebellar-frontal decreases later show worse verbal fluency, reading, working memory, or classroom accommodations needs, the imaging result becomes clinically sharper.
The Preprint Should Inform Monitoring, Not Overrule Outcomes
Imaging can detect neural change before a child has obvious classroom difficulty. That is the appeal of this line of work. Early fMRI shifts could eventually help target language therapy, working-memory supports, school accommodations, or treatment-planning adjustments.
Dose mapping: if reduced activation clusters align with higher radiation dose to cerebellar, frontal, temporal, or white-matter pathways, treatment planning could become more protective. If the same patterns appear regardless of dose, systemic illness, chemotherapy, inflammation, fatigue, or developmental timing may explain more of the signal.
Evidence-strength note: this was a preprint in a small disease-specific cohort. It measured early post-radiotherapy fMRI change, not long-term language, reading, school, or quality-of-life outcomes. Only 8 participants had complete five-timepoint exploratory trajectories, and only 2 of those received Cogmed training.1
The preprint status matters because methods and interpretation can change after peer review. That is especially relevant for machine-learning fMRI, where feature selection, cross-validation, preprocessing choices, and threshold decisions can strongly influence accuracy estimates in small samples.
Still, the anatomy is plausible. The signature included left inferior frontal and insular language-control regions, cerebellar territories linked to language sequencing, and parietal regions that can support phonological rehearsal. The pattern fits a real neurocognitive question rather than a black-box classifier detached from brain function.
Why Language Networks Matter After Pediatric Brain-Tumor Treatment
Language difficulty after pediatric brain-tumor treatment can look subtle at first. A child may speak fluently but struggle with word retrieval, classroom speed, working-memory load, or complex verbal instructions. Those problems can accumulate across school years.
Silent verb-generation fMRI is useful because it stresses several of those systems at once. The task requires hearing or seeing a noun, retrieving a related verb, holding the response internally, and suppressing overt speech. That combination makes it a reasonable probe for treatment-sensitive language-control circuits.
The study’s most useful clinical direction is early support. If future work links this fMRI signature to later school difficulty, survivorship clinics could intervene before a child has already fallen behind.
That future work should include parents, teachers, neuropsychologists, and scanner data together. A scan can detect a network change, but families need to know whether the child needs speech-language therapy, reduced verbal load, testing accommodations, memory supports, or school coordination.
Medulloblastoma care already involves tradeoffs between tumor control and late effects. A validated language-network marker could eventually make those tradeoffs more visible, especially when the child looks clinically stable but the brain network is already adapting.
The practical endpoint is not a prettier brain map. It is earlier recognition of children whose word retrieval, classroom pace, verbal working memory, or reading load may deteriorate after therapy. A scan signature becomes useful only if it changes follow-up intensity, therapy referral, school accommodations, or treatment-planning conversations.
The present classifier is an early version of that idea. It detected treatment timing, not disability. Turning it into a survivorship tool requires larger cohorts, harmonized scanner protocols, and outcomes that families recognize in school, daily communication problems, and practical rehabilitation planning.
For now, the best use is hypothesis generation: cerebellar-cerebral language networks deserve close follow-up in pediatric medulloblastoma survivorship.
Questions About Medulloblastoma Radiotherapy and Language fMRI
Did the fMRI classifier diagnose cognitive impairment?
No. It classified scan timing before vs. after radiotherapy. It did not diagnose a child’s language impairment.
Why does the cerebellum matter for language?
Cerebellar regions help coordinate sequencing, prediction, timing, and executive aspects of language. Damage or reduced activation there can affect language-related cognition even when speech muscles work.
Should fMRI be routine after radiotherapy?
The paper supports further monitoring research. It does not yet prove that routine fMRI surveillance improves outcomes.
References
- Da Rocha AJ, et al. Silent Verb Generation during fMRI Reveals Post-Radiotherapy Alterations in Cerebellar-Cerebral Language Regions in Patients Treated for Medulloblastoma. Research Square. 2026. https://doi.org/10.21203/rs.3.rs-9372156/v1
- Wood AG, et al. Language cortex activation in normal children. Neurology. 2004. PubMed search
- Vias C, Dick AS. Cerebellar contributions to language in typical and atypical development. Brain and Language. 2017. PubMed search
- De Smet HJ, Paquier P, Verhoeven J, Marien P. The cerebellum: its role in language and related cognitive and affective functions. Brain and Language. 2013. PubMed search