Mental-health AI agents are software systems that use artificial intelligence to screen, coach, triage, document, or coordinate care across mental-health workflows. A 2026 systematic review and meta-analysis of systems published from 2023 to 2025 found strong offline diagnostic metrics, but the evidence still leans much more heavily on chatbot demos and benchmark tasks than on prospective patient outcomes.1
Research Highlights
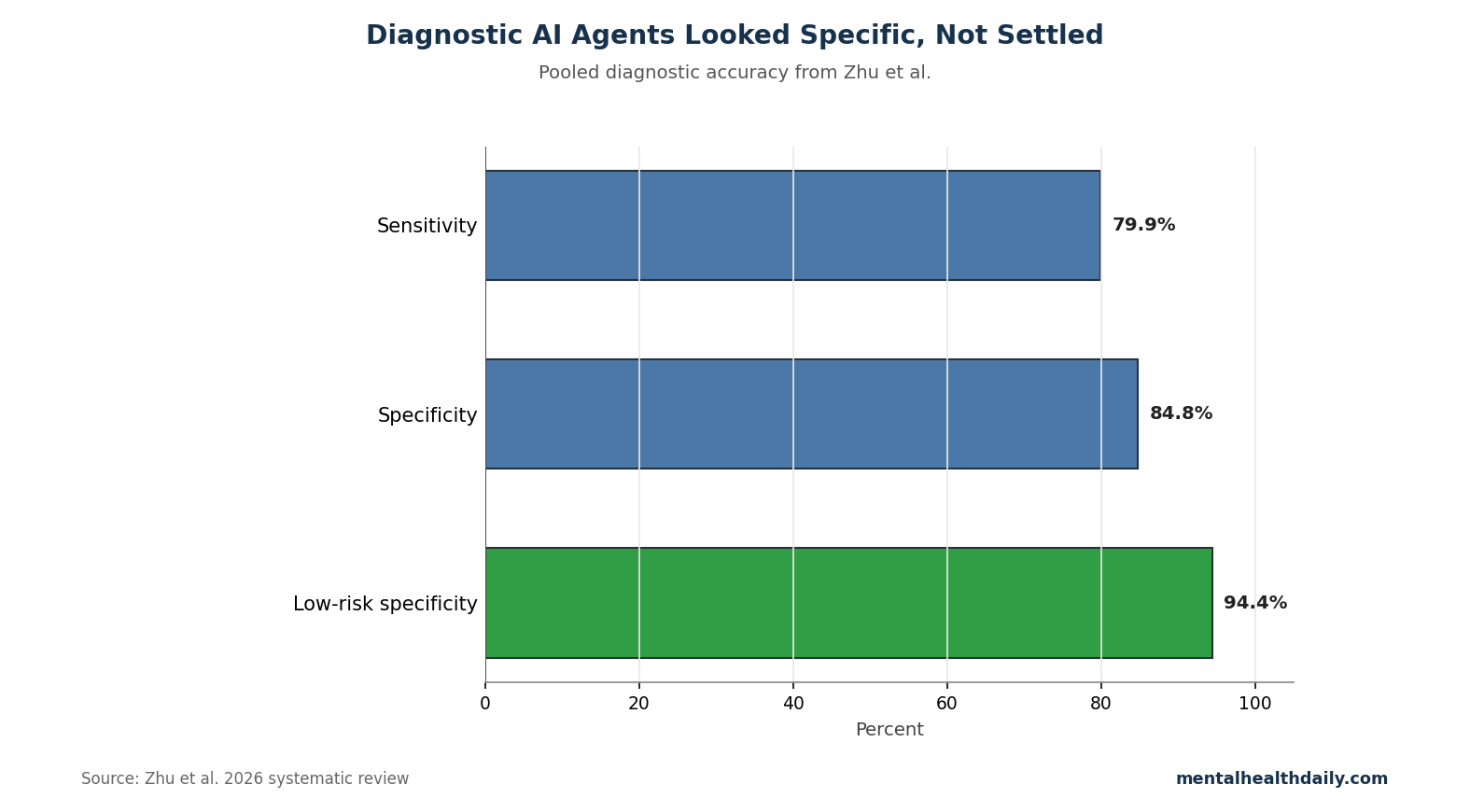
- Diagnostic performance looked decent: Across 11 diagnostic-agent records, Zhu et al. estimated pooled sensitivity of 0.799 and pooled specificity of 0.848, with a diagnostic odds ratio of 39.7.1
- Heterogeneity was severe: Sensitivity heterogeneity was I² = 97.4% and specificity heterogeneity was I² = 99.5%, meaning the pooled estimate mixes very different disorders, datasets, standards, and model architectures.1
- Most tools still looked like chatbots: The review found that around 91.74% of studies used chat interfaces, with far fewer systems embedded into clinician-supervised workflows, records, sensor streams, or longitudinal monitoring.1
- Coverage was narrow: Systems clustered around depression, anxiety, and suicidality; severe mental illness, neurocognitive disorders, substance use, older adults, and complex comorbidity were less developed.1
- Human oversight remains central: Patient-facing work on conversational agents found interest in AI support, but a preference for humans in the loop when the task becomes clinical or high-risk.2
The calibrated read is straightforward: AI agents may become useful mental-health infrastructure, but current evidence supports supervised screening and workflow assistance more strongly than autonomous therapy, diagnosis, or crisis management.
Pooled Diagnostic Metrics Came From 11 Different Agent Studies
Sensitivity is the proportion of true cases a test catches; specificity is the proportion of non-cases it correctly leaves alone. In the Zhu review, the pooled diagnostic-agent estimate was 0.799 sensitivity and 0.848 specificity across 11 records.1
Those numbers sound cleaner than the underlying evidence. The review pooled tools for depression, obsessive-compulsive disorder, suicide-risk stratification, audio-based depression screening, anxiety-depression classification, and simulated diagnostic interviews. Reference standards ranged from clinician consensus to scale cutoffs and published vignettes.
- Rule-in use is more plausible than rule-out use: A specificity-heavy tool can help prioritize people for human review, especially when services are overloaded.
- False reassurance is the danger: A tool with uneven sensitivity can miss high-risk people if it is used as a gatekeeper rather than a queueing aid.
- Benchmark accuracy is not clinical safety: A model can classify vignettes well and still fail when a real person is intoxicated, dissociated, ashamed, ambivalent, or intentionally evasive.
The low-risk subset in Zhu et al. raised specificity to 0.944 and diagnostic odds ratio to 362.2, but that result came from only 3 lower-bias records with a combined sample of 142,358. Method quality clearly changed the apparent performance; it did not prove general-purpose clinical reliability.1
91.74% of Mental-Health Agent Studies Used Chat Interfaces
The review separated true agentic properties from ordinary chatbot presentation. A basic chatbot answers or asks questions. An agentic workflow can plan steps, retrieve outside information, call tools, hand off to specialized subagents, monitor risk, or coordinate documentation.
Zhu et al. found a field still dominated by visible conversation. Around 91.74% of included studies used chat interfaces, which makes sense for screening, psychoeducation, and low-intensity support. Chat is accessible, cheap, and emotionally legible to users.1
Clinical bottleneck: the same interface concentrates the highest-risk failures. The chatbot becomes the face of the system when a user expresses suicidal intent, psychosis, domestic violence, medication confusion, or abuse. A warm response is not enough unless the system also knows when to escalate, what local resources exist, and how to preserve a record for human review.
Human Review Remains the Near-Term Safety Layer
The strongest near-term design is not a single model pretending to be a therapist. It is a divided workflow:
- Screening agent: gathers symptoms using validated instruments such as PHQ-9 or GAD-7 and writes structured summaries.
- Retrieval agent: pulls local protocols, crisis resources, medication lists, and prior notes instead of inventing advice from memory.
- Safety auditor: reviews the interaction for self-harm, violence, psychosis, abuse, medical emergency, or medication-risk language.
- Human reviewer: accepts, edits, overrides, or escalates the output when clinical stakes exceed self-management.
This architecture reduces the fantasy that a model has clinical judgment. It treats the AI as a fast intake and documentation layer whose outputs become safer when constrained, logged, and reviewed.
Current Evidence Is Mostly Offline, Not Patient-Outcome Data
Zhu et al. is a preprint systematic review, and many included systems were evaluated with offline metrics, simulated sessions, expert ratings, or short user studies. That design can support claims about feasibility, benchmark performance, and design gaps. It cannot prove that autonomous mental-health AI improves suicide attempts, hospitalization, remission, adherence, or long-term functioning.
Adjacent work reaches the same boundary. Patients often see potential in conversational agents but prefer human oversight for clinical decisions.2 General medical large language models can encode impressive clinical knowledge, yet knowledge benchmarks do not settle safety, equity, privacy, or liability in mental-health care.3
Evidence ladder: mental-health AI needs to move from classification benchmarks to workflow studies, safety audits, and patient outcomes.
For mental-health software, a real evidence ladder has several rungs. Offline classification comes first: the system receives labeled examples and its predictions are scored against a reference. Usability testing comes next: users and clinicians can operate the interface without obvious confusion or harm. Prospective workflow testing asks whether the tool changes intake time, documentation quality, escalation speed, or missed-risk rates in real care.
Outcome testing is stricter. A mental-health agent would need to improve something patients actually care about: symptom remission, treatment adherence, emergency response, relapse detection, quality of life, reduced wait time, fewer abandoned referrals, or safer crisis routing. Zhu et al. found much more evidence at the first 2 rungs than at the last 2.1
- Screening endpoint: Does the tool catch high-risk symptoms earlier than ordinary intake?
- Workflow endpoint: Does it reduce clinician burden without lowering note quality or escalation accuracy?
- Safety endpoint: Does it handle suicidal ideation, abuse, psychosis, intoxication, and medical emergencies with pre-specified routing?
- Equity endpoint: Does performance hold across age, sex, language, culture, disability, socioeconomic status, and diagnosis?
Privacy Rules Need Data Retention, Model Access, and Audit Trails
Mental-health data are unusually sensitive because they include sexuality, trauma, suicidality, family violence, substance use, legal exposure, and stigmatized symptoms. A mental-health agent that stores long conversations, uses third-party model calls, or combines chat logs with electronic health records can create a privacy surface larger than ordinary telehealth.
- Data retention: how long conversation logs are stored and who can read them.
- Model access: whether prompts leave the health system or stay inside a controlled environment.
- Audit trail: which human reviewed high-risk outputs and when escalation occurred.
Accountability chain: the safer system names who owns each decision. The AI can suggest, summarize, flag, and draft. A clinician, crisis worker, or service protocol should own diagnosis, involuntary-risk decisions, medication changes, emergency escalation, and decisions to close a case. Without that chain, the interface may feel supportive while the responsibility structure stays vague.
The next generation of studies should publish prompt rules, model version, escalation rules, human-review rate, override rate, adverse events, and demographic error analysis. A black-box chatbot with a pleasant tone is not enough evidence for clinical use.
Safest current use: a depression-screening assistant can ask a validated item set, summarize severity, flag self-harm language, and route the record to a human queue. A documentation agent can convert a clinician’s note into structured fields. A retrieval agent can pull clinic policies and local crisis contacts. Each task is bounded, reviewable, and easier to audit than an open-ended therapy bot.
Procurement test: services should ask vendors for error logs, escalation examples, demographic performance, data-retention rules, model-update policy, and human-review workflow before buying. A demo conversation with smooth empathy is a weak test because it avoids rare high-stakes failures.
Governance benchmark: Stade et al. argued that behavioral-health large language models need staged deployment, explicit risk categories, interdisciplinary review, and measurement before expansion.4 That framework fits Zhu et al.’s review because the safest agent roles are narrow and observable: intake summaries, triage flags, retrieval, and documentation support. The more autonomous the system becomes, the stronger the audit burden should become.
Questions About Mental-Health AI Agents
Can an AI agent diagnose depression or anxiety?
It can screen for symptoms and flag risk. Diagnosis still requires a clinical context: duration, impairment, differential diagnosis, substance use, medical causes, medication effects, safety risk, and longitudinal course.
Where did the 2026 review point AI agents first?
Structured intake, symptom tracking, psychoeducation, documentation support, and triage queues are safer than autonomous treatment or crisis counseling.
Why is severe heterogeneity a problem?
I² values near 100% mean studies disagree so much that the pooled average can mislead. A tool that works for vignette-based obsessive-compulsive disorder classification may say little about live suicide triage or psychosis screening.
Should patients use AI chatbots for therapy?
They may help with journaling, skills practice, and low-risk reflection. They should not replace human care for suicidality, mania, psychosis, trauma crises, eating-disorder medical risk, medication decisions, or diagnostic uncertainty.
References
- Artificial Intelligence Agents in Mental Health: A Systematic Review and Meta Analysis. Zhu L, Wang W, Liang Z, et al. medRxiv. 2026. doi:10.64898/2026.04.21.26351365
- Artificial intelligence conversational agents in mental health: Patients see potential, but prefer humans in the loop. Lee H, Wright C, Ferranto J, et al. Frontiers in Psychiatry. 2025;15. doi:10.3389/fpsyt.2024.1505024
- Large language models encode clinical knowledge. Singhal K, Azizi S, Tu T, et al. Nature. 2023;620:172–180. doi:10.1038/s41586-023-06291-2
- Stade EC, Stirman SW, Ungar LH, et al. Large language models could change the future of behavioral healthcare: a proposal for responsible development and evaluation. npj Mental Health Research. 2024;3:12. doi:10.1038/s44184-024-00056-z