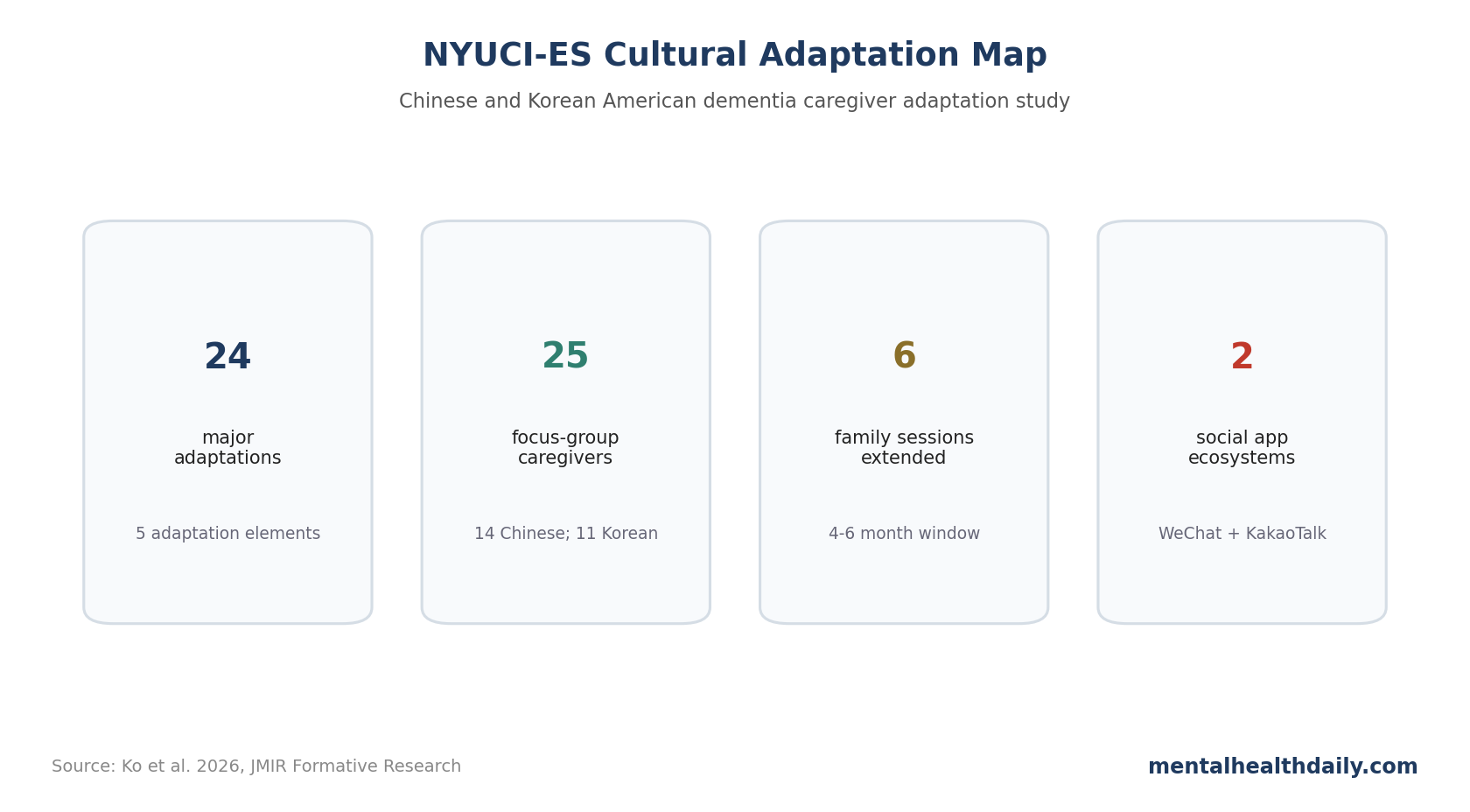
A 2026 descriptive study documented 24 major cultural adaptations to the New York University Caregiver Intervention-Enhanced Support (NYUCI-ES) for Chinese and Korean American dementia caregivers. The work is not an outcomes report yet; it is a careful map of how an evidence-based caregiver intervention had to change before it could plausibly fit East Asian immigrant family caregiving contexts.1
Research Highlights
- 24 adaptations were identified: the research categorized changes across content, context, relationship fidelity/core elements, engagement, and cultural competence.1
- Language changes went beyond translation: materials were translated into simplified Chinese, traditional Chinese, and Korean, while terms such as memory loss, support, education, and meeting were used to reduce stigma.1
- Family counseling was broadened: participants could include fictive kin, overseas relatives, friends, neighbors, and community staff when those people functioned as real caregiving supports.1
- Digital communication matched community habits: WeChat, KakaoTalk, online sessions, and culturally matched staff were used to reduce participation friction.1
- Outcomes still need the parent trial: the adaptation process is valuable, but caregiver depression, burden, placement delay, and service-use effects require completed randomized data from NCT05461495.
Dementia caregiving interventions often fail when they treat culture as a translation problem. Ko et al. show a more practical pattern: preserve the intervention’s core counseling logic, then adapt language, family membership, staff matching, engagement, and stigma-sensitive communication.
NYUCI-ES Preserved Counseling Core While Changing Delivery
The original New York University Caregiver Intervention (NYUCI) used individual and family counseling, support groups, and ad hoc counseling to reduce caregiver distress and delay nursing home placement. Earlier NYUCI trials reported lower caregiver depressive symptoms and stress, better self-rated physical health, and delayed placement by a median of 557 days in one major analysis.1
NYUCI-ES adapted that model for Chinese and Korean American dementia caregivers. The parent randomized trial will report participant outcomes separately, so this paper should be read as an implementation and adaptation paper.
- Frameworks: the team used cultural adaptation elements and the Framework for Reporting Adaptations and Modifications-Enhanced (FRAME).
- Rigor tool: the Template for Intervention Description and Replication (TIDieR) checklist guided reporting.
- Community input: 25 caregivers participated in focus groups, including 14 Chinese and 11 Korean caregivers.
- Trial registration: the parent study is registered as NCT05461495.
Translation, Dementia Stigma, and Family Obligation Shaped Content
The content adaptations included translated consent forms, flyers, questionnaires, and other study materials. During implementation, traditional Chinese materials were added for participants from places such as Hong Kong or Taiwan who did not use simplified Chinese.1
The wording changes were clinically meaningful. Dementia stigma often overlaps with mental-illness stigma in East Asian contexts, and dementia may be misread as normal aging or fate. Softer terms such as memory loss, support, consulting, meeting, and education were used to reduce threat and make counseling feel less alien.
The researchers also added culturally specific questionnaires on familism, affiliated stigma against dementia, and acculturation. These are not decorative constructs. They capture pressures that can shape whether a caregiver asks for help, includes family members, or suppresses personal strain.
Fictive Kin and Social Apps Made Family Counseling More Realistic
A strict biological-family definition would have missed how some caregivers actually receive support. Ko et al. allowed fictive kin into family counseling: close friends, neighbors, overseas relatives, community organization staff, or other trusted people who functioned as family support in practice.1
Communication channels also changed. Counseling could occur in person or online, and participant communication used familiar apps such as WeChat for many Chinese participants and KakaoTalk for Korean participants.
Those changes affect who can use the intervention. If an intervention requires unfamiliar platforms, stigmatizing terms, or a narrow family definition, it can select for the least isolated caregivers and miss the people most likely to need support.
Culturally Matched Staff Were Part of the Intervention Infrastructure
NYUCI-ES used bilingual social workers and research assistants fluent in Chinese or Korean, with knowledge of the relevant cultures. Social workers also received training in caregiving approaches specific to Chinese and Korean populations.1
The adaptation process also used community organization partnerships, community advisory input, weekly meetings with the original intervention developer, and clinical supervision to preserve fidelity while adapting delivery.
Access infrastructure: trust, language, stigma, and family structure determine whether a caregiver intervention can be accessed and completed.
Outcome Evaluation Should Track Access, Completion, and Family Conflict
The parent trial should not judge success only by caregiver depression scores. Cultural adaptation is supposed to improve access, fit, retention, and usefulness; those process outcomes deserve formal measurement too.
Key access metrics include referral source, language preference, time from first contact to enrollment, reasons for declining, number of outreach attempts, and whether the caregiver joined through community organization contact, social media, or clinical referral.
Reach matters because adaptation is the intervention test: if the adapted program enrolls only caregivers who already trust clinics, speak English comfortably, and have family members willing to attend counseling, the cultural work has not solved the access problem it was designed to address.
Completion metrics need the same attention as symptom outcomes. The adapted model extended the timing of family counseling sessions from 4 months to 4-6 months. The trial should show whether that extra flexibility improves session completion, family attendance, and intervention dose.
Family-conflict measurement is central in East Asian dementia caregiving. Filial piety and familism can motivate care, but they can also intensify guilt, silence, and role strain. An adapted family intervention should measure whether conversations become easier alongside whether the caregiver feels less burdened.
The best test of adaptation is whether the core intervention reaches people who would otherwise avoid it. If culturally matched staff, softer language, and familiar communication tools improve participation without diluting counseling fidelity, that is a meaningful implementation result.
Stigma-Sensitive Language Can Improve Reach Without Hiding Dementia
Softer terms such as memory loss or support can function as an entry point for clear dementia education. The first contact may need to reduce fear before direct education can land.
Caregivers may already be managing shame, family disagreement, immigration stress, language barriers, and distrust of unfamiliar services. If the recruitment language sounds stigmatizing or too psychiatric, the intervention can fail before counseling begins.
The adapted approach can introduce dementia facts gradually while preserving respect. A family may enter through memory support, then learn about behavioral symptoms, caregiver stress, safety planning, and future care needs once trust exists.
Clinical framing can become more direct as rapport builds: the caregiver enters through acceptable language, then receives clearer education about symptoms, planning, and support.
Adaptation Should Avoid Treating Asian American Caregivers as One Group
Ko et al. focused on Chinese and Korean American caregivers, not a single undifferentiated Asian American group. Language, migration history, religion, family structure, health-system trust, and dementia beliefs differ across communities, so a single pan-Asian adaptation can miss the families it is supposed to reach.
Even within Chinese and Korean groups, the intervention had to account for simplified vs. traditional Chinese materials, Mandarin and Cantonese, overseas family members, community organizations, and different comfort levels with counseling. A culturally adapted intervention still needs individual tailoring.
Fidelity Means Keeping the Active Ingredient Visible
Cultural adaptation can fail in 2 opposite ways. One failure is under-adaptation: the intervention stays faithful on paper but unusable in practice. The other is over-adaptation: the intervention becomes acceptable but loses the active ingredients that made it evidence-based.
Ko et al. addressed that tension by keeping weekly meetings, supervision, developer involvement, and focus on core counseling elements. That fidelity scaffolding is what makes the adaptation scientifically useful rather than a loose community program with the NYUCI name attached.
Community Partnerships Build Caregiver Trust
Community organizations can lend trust that universities and hospitals do not automatically have. For dementia caregiving, that trust may determine whether families disclose conflict, stigma, financial strain, or fear about future placement.
Partnerships can also keep the intervention honest. Community advisors can identify when language is off, when scheduling is unrealistic, when a platform is unfamiliar, or when a proposed adaptation looks good academically but fails in daily caregiving life.
Trial reporting should show which partnership routes actually produced enrollment, attendance, and retention. A culturally adapted intervention is stronger when the access pathway is measurable in addition to described.
Outcome tables should also separate Chinese and Korean participants when sample size allows, because pooled averages can hide different barriers, preferences, and response patterns.
Questions About Dementia Caregiver Adaptation
Does this prove NYUCI-ES improves caregiver outcomes?
No. This paper documents adaptation strategy. The randomized trial outcomes are needed for caregiver depression, burden, family conflict, and placement endpoints.
Why is translation alone too thin for this intervention?
Translation changes words. Cultural adaptation changes the delivery environment: who counts as family, which terms feel stigmatizing, which apps people use, who delivers counseling, and how trust is built.
Is this only relevant to Chinese and Korean caregivers?
The specific adaptations are population-specific. The broader method applies elsewhere: preserve core elements, adapt access barriers, and document every change clearly enough that others can replicate or test it.
References
- Exploring the Cultural Adaptation of an Ongoing Evidence-Based Intervention for Chinese and Korean American Dementia Caregivers. Ko et al. doi:10.2196/86499
- Better reporting of interventions: Template for Intervention Description and Replication checklist and guide. Hoffmann et al. doi:10.1136/bmj.g1687
- FRAME: an expanded framework for reporting adaptations and modifications to evidence-based interventions. Stirman et al. doi:10.1186/s13012-019-0898-y
- New York University Caregiver Intervention studies. PubMed search. PubMed search