A 2026 case series of 10 adults with refractory postherpetic neuralgia found: 3 of 8 patients responded to a spinal cord stimulation trial, 2 kept meaningful 24-month relief after implantation, and 3 dorsal root entry zone lesioning cases reported 60-90% pain relief at 24 months.1 The data are too small to rank the procedures, but they support reversible stimulation first when the dorsal column pathway still works.
Research Highlights
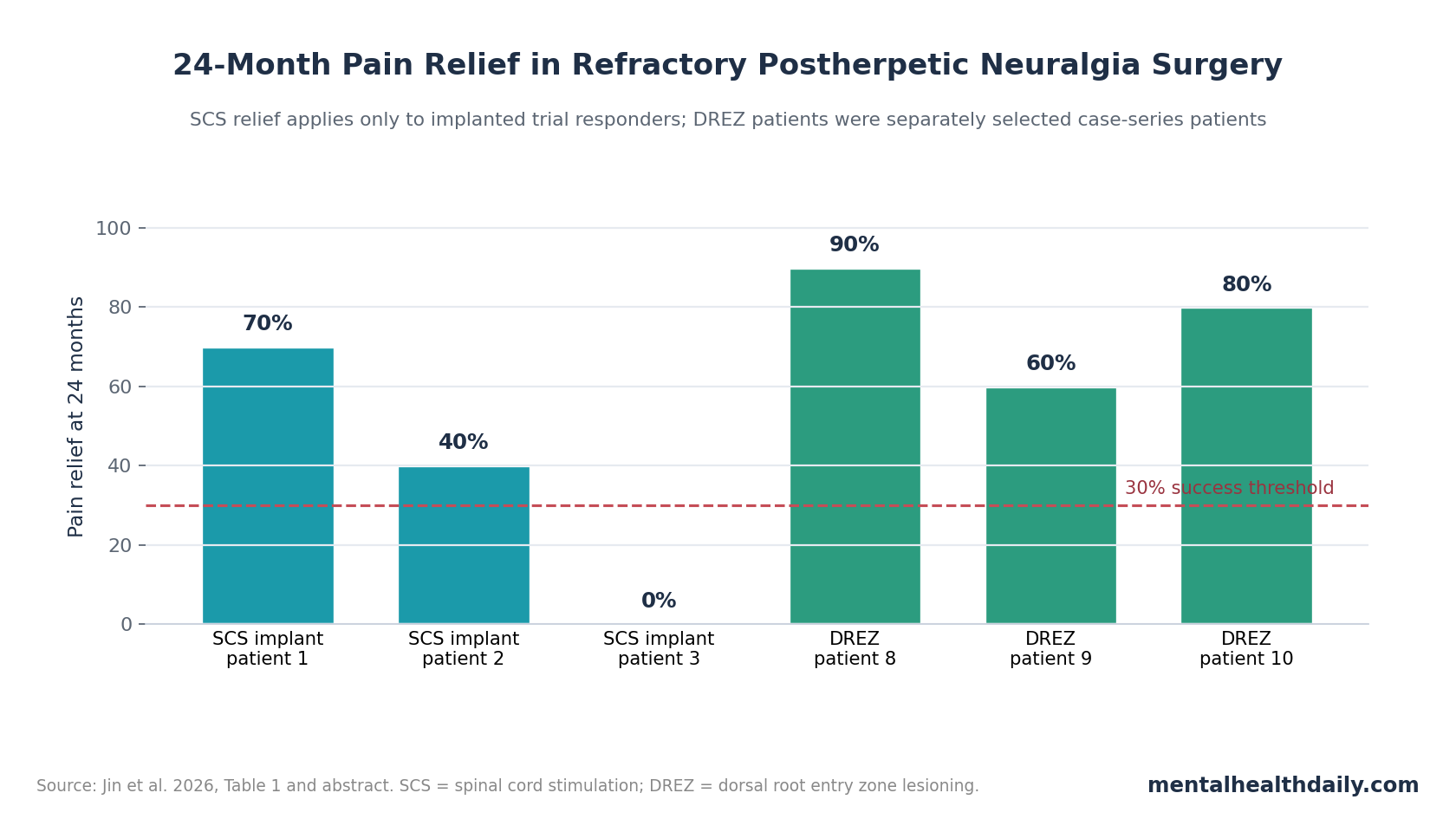
- SCS helped a minority: 3 of 8 patients achieved the trial threshold of ≥30% Numeric Rating Scale pain reduction, and 2 of the 3 implanted patients kept substantial relief at 24 months.1
- DREZ relief exceeded implanted-SCS relief: The 3 dorsal root entry zone lesioning cases reported 90%, 80%, and 60% pain relief at 24 months, with 1 mild sensory-loss complication and no motor deficit.1
- Baseline severity was extreme: The 10-person cohort entered surgery with mean NRS pain 9.8 ± 0.6 and mean Pain Disability Index 55.2 ± 4.5 after failed medications, nerve blocks, or other procedures.1
- Costs split the decision: Mean surgical cost was CNY 133,700 for SCS vs. CNY 56,100 for DREZ in this Chinese center, but SCS remained reversible and less destructive.1
- Evidence quality stays weak: Prior PHN intervention reviews found mostly small, heterogeneous studies, so this 2026 series should guide hypothesis and selection logic rather than establish superiority.2,3
Spinal cord stimulation (SCS) uses implanted electrodes to stimulate the dorsal columns of the spinal cord, aiming to dampen pain signaling through segmental and descending inhibitory pathways. Dorsal root entry zone lesioning (DREZ lesioning) is different: it deliberately creates small lesions where sensory roots enter the spinal cord to interrupt hyperactive pain neurons in the dorsal horn.
Mechanism-based selection: these procedures fit different versions of severe postherpetic neuralgia. If painful input can still be modulated through intact dorsal-column circuits, SCS has the advantage of a trial phase and reversibility.
If herpes zoster has produced severe deafferentation, dorsal-root atrophy, or dorsal-horn pathology, stimulation coverage may fail and an ablative procedure may become more plausible.
3 of 8 SCS Trials Met the ≥30% Pain-Reduction Threshold
Jin et al. reviewed 10 adults treated at Xuanwu Hospital from 2011 to 2023. All had neuropathic pain lasting more than 6 months after herpes zoster and had failed optimized medical care, including drug treatment and interventional pain procedures. Pain was thoracic in every case, and 8 of 10 patients had pain across 2 or more dermatomes, meaning more than 1 spinal sensory band was involved.1
The SCS pathway began with a temporary trial. A positive trial required ≥30% reduction on the Numeric Rating Scale (NRS), a 0-10 pain scale where 10 means worst imaginable pain. The threshold was not arbitrary: chronic-pain trial guidance often treats about 30% pain reduction as a clinically meaningful improvement.8
Trial results separated the cohort quickly:
- 3 of 8 trial patients responded: these patients proceeded to permanent implantable pulse generator placement.
- 2 of 3 implanted patients kept benefit: final 24-month relief was 70% and 40% in 2 patients.
- 1 implanted patient lost efficacy: initial relief faded within 2 months, final relief was 0%, and the patient requested device removal.
- 5 trial patients did not respond enough: their trial electrodes were removed; 1 later underwent DREZ lesioning.
The SCS signal therefore looks real but selective. Mean NRS among implanted patients improved from 10.0 before surgery to 4.0 at 1 month, then drifted to 6.3 at 24 months. That pattern matches the clinical reason SCS trials exist: the device is valuable when the trial predicts durable coverage, but a good early response can still fade.
DREZ Lesioning Produced 60-90% Relief in 3 Selected Patients
DREZ lesioning was used in 3 patients: 1 after failed SCS trial and 2 as the initial surgical intervention after declining SCS. Their final NRS scores were 1, 4, and 2 after baseline scores of 10 in all 3 cases. Pain Disability Index scores also dropped from 65 to 16, 58 to 22, and 55 to 14, giving a mean improvement from 59.3 ± 5.1 to 17.3 ± 4.1.1
Selection is the core issue: DREZ lesioning is not a cleaner version of SCS. It is an ablative operation aimed at dorsal-horn pain generators, so the risk-benefit threshold is higher. In this series, 1 patient developed mild segmental sensory loss at the lesioned levels, but no patient had motor weakness, cerebrospinal fluid leakage, wound infection, or a severe neurological complication.
Patient 8 supplied the clearest anatomical clue: preoperative MRI showed a focal T2 hyperintense signal in spinal cord segments matching the painful dermatomes, and surgery revealed atrophic, yellowish dorsal roots.
That combination suggests a pain state with visible dorsal-root or dorsal-horn injury layered onto peripheral nerve irritation. In that setting, poor SCS response is expected because stimulation needs usable pathways to modulate.
SCS and DREZ Answer Different PHN Surgery Questions
Persistent pain biology: postherpetic neuralgia begins after varicella-zoster virus injures sensory pathways. Pain can persist because peripheral nerves, dorsal root ganglia, spinal dorsal horn neurons, glia, and descending pain-control systems stay sensitized after the rash resolves.
Burning, stabbing, electric pain, allodynia, sleep disruption, and disability can continue for years.
Intervention choice depends on where the dominant pain generator appears to sit:
- SCS fits modifiable transmission: stimulation can be tested before permanent implantation, and a failed trial can be removed without committing the patient to a destructive procedure.
- DREZ fits severe deafferentation: lesioning is more biologically plausible when imaging, intraoperative appearance, or failed stimulation suggests hyperactive dorsal-horn neurons and damaged roots.
- DRG stimulation may fit focal dermatomal pain: dorsal root ganglion stimulation targets the sensory nerve-cell cluster for a specific dermatome, but PHN evidence remains early and device access varies by setting.6
A 2019 systematic review of interventional treatments for postherpetic neuralgia reached the same cautious destination: procedures may help selected patients, but the evidence base is too uneven for a universal algorithm.2 A neurosurgical review the same year described an armamentarium rather than a settled hierarchy, reflecting the same problem: refractory PHN is uncommon enough, heterogeneous enough, and invasive enough that large comparative trials are scarce.3
The Cost Difference Was Large, but It Was Not the Whole Decision
Jin et al. reported a mean hospital stay of 18.4 days for SCS and 13.7 days for DREZ lesioning. Mean surgical cost, including operation, device, and anesthesia, was about CNY 133,700 for SCS vs. CNY 56,100 for DREZ. The implantable pulse generator drove much of the SCS cost.1
Cost does not erase reversibility: the cheaper procedure is not automatically the better first procedure. SCS has a trial phase, lower surgical destructiveness, adjustability, and reversibility. DREZ has no equivalent undo button.
If SCS works, the higher upfront device cost may buy a safer therapeutic path. If SCS fails and DREZ is needed later, the cumulative pathway becomes more expensive than choosing DREZ first in a patient who had obvious dorsal-root or dorsal-horn pathology.
Practical cost read: the economic result argues for better selection, not for skipping SCS. Imaging evidence of dorsal horn injury, inability to obtain paresthesia coverage, profound sensory loss, or failed trial stimulation may shift the balance toward DREZ. A patient with preserved sensory pathways and good trial coverage still belongs in the reversible lane first.
Case-Series Evidence Cannot Prove Surgical Superiority
Evidence-strength note: this was a retrospective 10-patient case series, not a randomized trial. It can show that carefully selected patients improved, document complications, and generate a treatment-sequencing hypothesis. It cannot prove that DREZ is superior to SCS, that either procedure beats continued medical care in comparable patients, or that the same cost pattern would hold outside this hospital.
Several limits are especially important:
- Selection bias: patients did not enter SCS or DREZ randomly, so the treatment groups started with different clinical clues.
- Small numbers: 3 DREZ cases and 3 SCS implants are enough for case detail, not stable effect estimates.
- Long treatment window: patients were treated across 2011-2023, when devices, technique, and clinical practice may have changed.
- Local costs: CNY 2023 institutional costs do not translate directly to US, European, or other Asian systems.
Prior SCS reports, including early herpes-zoster-associated pain series and newer long-term observations, support the idea that neuromodulation can help PHN in selected patients.4,5
Imaging work also supports the idea that dorsal-horn injury can separate PHN subgroups, including a 2025 case-control study describing T2 high-signal zones in the spinal cord dorsal horn among patients treated with SCS for herpes-zoster-associated pain.7 The 2026 series is most useful when read inside that framework: anatomy may tell clinicians when stimulation is likely to fail.
Questions About SCS and DREZ for Postherpetic Neuralgia
Does this case series mean DREZ lesioning is better than spinal cord stimulation?
No. The DREZ cases had larger 24-month pain-relief percentages, but the groups were tiny and clinically selected. DREZ may look best in patients whose pain is driven by dorsal-root or dorsal-horn injury, while SCS remains the safer first surgical test when stimulation coverage is plausible.
Why use SCS first if DREZ relief looked stronger?
SCS is adjustable, trialable, and reversible. DREZ lesioning deliberately damages a small sensory-entry zone to interrupt pain signaling, so it requires stronger evidence that the pain generator is central and segmental.
What would make a patient a stronger DREZ candidate?
Failed SCS trial, severe dermatomal sensory loss, imaging evidence of dorsal horn involvement, intraoperative dorsal-root pathology, and pain that remains tightly mapped to damaged segments would all make the DREZ rationale stronger. Those clues still need prospective validation.
What study is needed next?
A multicenter prospective registry or trial should capture baseline sensory testing, spinal MRI, dermatomal mapping, SCS trial coverage, NRS pain, Pain Disability Index, medication use, adverse events, and costs before assigning or comparing procedures.
References
- Jin W, Yang D, Li J, et al. Spinal cord stimulation and DREZ lesioning for refractory postherpetic neuralgia: an exploratory case series. Journal of Pain Research. 2026;19:583921. doi:10.2147/JPR.S583921
- Lin CS. Interventional treatments for postherpetic neuralgia: a systematic review. Pain Physician. 2019;22(3):209-228. doi:10.36076/ppj/2019.22.209
- Texakalidis P, Tora MS, Boulis NM. Neurosurgeons’ armamentarium for the management of refractory postherpetic neuralgia: a systematic literature review. Stereotactic and Functional Neurosurgery. 2019;97(1):55-65. doi:10.1159/000499476
- Harke H, Gretenkort P, Ladleif HU, Koester P, Rahman S. Spinal cord stimulation in postherpetic neuralgia and in acute herpes zoster pain. Anesthesia and Analgesia. 2002;94(3):694-700. doi:10.1097/00000539-200203000-00040
- Anisimov ED, Andrushkevich OM, Dzhafarov VM, Amelina EV, Rzaev JA, Slavin KV. Long-term effects of spinal cord stimulation on pain in postherpetic neuralgia. Stereotactic and Functional Neurosurgery. 2024. doi:10.1159/000542138
- Dorner A, Dascalu I, Osborn J, Varshney V. Dorsal root ganglion stimulation for postherpetic neuralgia: a pilot scoping review of the current evidence. Cureus. 2025. doi:10.7759/cureus.93664
- Arakawa K, Nakagawa M, Abe Y, Morimatsu H. T2 high-signal-intensity zone of the spinal cord dorsal horn in patients treated with spinal cord stimulation for herpes zoster-associated pain: a retrospective case-control study. Journal of Anesthesia. 2025;39(2):273-281. doi:10.1007/s00540-025-03458-1
- Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149-158. doi:10.1016/S0304-3959(01)00349-9