A longitudinal MIDUS analysis involving 840 adults found that loneliness scores higher than a person's objective social-isolation score were linked to later cognitive impairment mainly through chronic disease burden, while the allostatic-load pathway was weaker than the chronic-disease pathway and not statistically confirmed for the main cognitive outcomes.1
Research Highlights
- Loneliness was separated from isolation: researchers modeled social asymmetry, meaning loneliness that remained after accounting for objective contact and isolation measures.1
- Chronic disease carried the signal: as social asymmetry scores increased, chronic disease burden increased (β = 0.59, p < .001), and chronic disease burden predicted poorer later episodic memory (β = −0.04, p = .016).1
- Allostatic load was less convincing: social asymmetry was not significantly associated with allostatic load in the main model (β = 0.08, p = .062), and allostatic-load indirect effects were not significant.1
- Model fit was strong: the structural model had CFI = 0.98, SRMR = 0.02, and RMSEA = 0.069, which supports the tested pathway structure.1
- Causal timing remains limited: the 840-person longitudinal design adjusted for baseline cognition and covariates, but it cannot prove that loneliness mismatch caused chronic disease or cognitive decline.
Social asymmetry means a mismatch between felt loneliness and measured social isolation. A person can have frequent contact and still feel emotionally alone, or have limited contact without feeling lonely. This analysis focused on the loneliness surplus after objective isolation was already modeled.
840 MIDUS Adults Were Followed From Social Experience to Cognition
Cintron et al. used data from the Midlife in the United States Biomarker Project, a U.S. longitudinal study that collects psychosocial measures, clinical biomarkers, health conditions, and cognitive testing. The main analytic sample included 840 adults with a mean age of 53.86 years, ranging from 34 to 81 years; 57% were female, and 92% were White.1
- Social exposure: loneliness and objective social isolation were combined into a residualized mismatch score.
- Health pathway 1: chronic disease burden counted physician-diagnosed conditions, with a mean of 2.18 conditions and a range of 0–16.
- Health pathway 2: allostatic load summarized multisystem biological wear, with a mean of 2.30.
- Cognitive endpoints: later episodic memory and executive function measured memory retrieval and higher-order control processes.
Allostatic load is a composite index of stress-related physiological strain across systems such as inflammation, metabolism, cardiovascular function, and neuroendocrine regulation. It tries to capture accumulated biological wear rather than a single disease diagnosis.
Chronic Disease Burden Explained More Than Stress Biomarkers
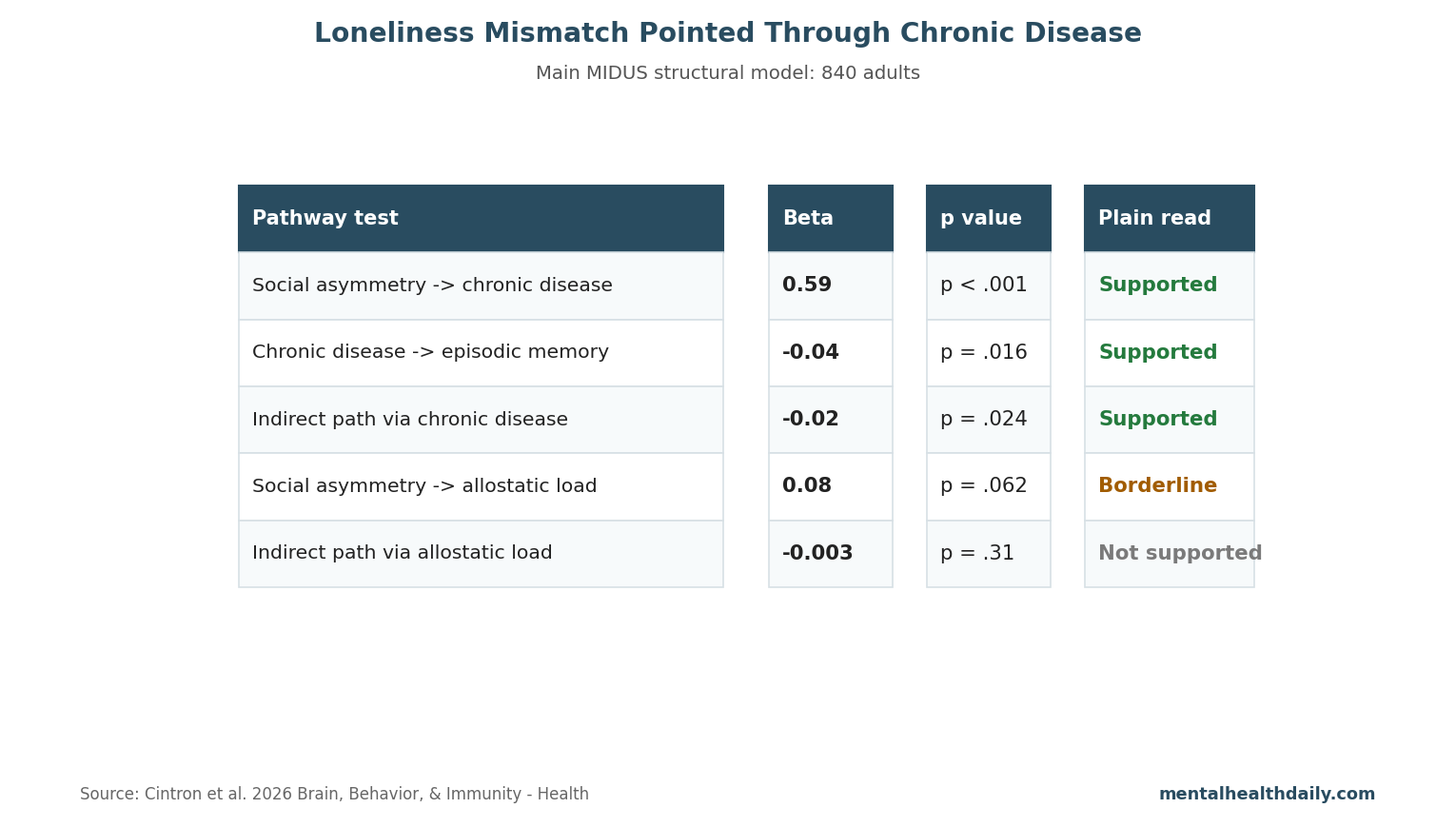
Main pathway: social asymmetry had a strong positive association with chronic disease burden, with standardized β = 0.59 and p < .001. Higher chronic disease burden then predicted poorer episodic memory at Wave 3, with standardized β = −0.04 and p = .016.1
Indirect effect: the pathway from social asymmetry to episodic memory through chronic disease burden was statistically significant, with β = −0.02 and p = .024. In plain language, the model linked loneliness mismatch to later memory partly because people with higher mismatch also carried more chronic disease.
Allostatic load did not carry the same main pathway. Social asymmetry was only borderline associated with allostatic load, and indirect effects through allostatic load were nonsignificant for episodic memory (β = −0.003, p = .31) and executive function (β = −0.002, p = .35).1
A Larger Sensitivity Sample Replicated the Chronic-Disease Pattern
Replication sample: a broader sensitivity analysis included 4,515 people. Social asymmetry again predicted chronic disease burden, with β = 0.58 and p < .001. Chronic disease burden predicted both episodic memory (β = −0.02, p = .011) and executive function (β = −0.01, p = .029).1
Replication detail: indirect chronic-disease pathways were significant for episodic memory (β = −0.01, p = .012) and executive function (β = −0.01, p = .030). Allostatic-load indirect pathways again were not significant.
This pattern points away from a generic “stress gets under the skin” explanation as the main measured route in these data. The more concrete route was multimorbidity: accumulated chronic illness burden that can affect vascular risk, inflammation, sleep, pain, medication load, mobility, and cognitive reserve.
Adjacent Evidence Links Social Connection, Disease, and Dementia Risk
Pathway context: earlier work by Cacioppo and Hawkley described perceived social isolation as a risk factor for cognitive and health outcomes through sleep disruption, vascular pathways, inflammation, and behavior change.2 Meta-analytic evidence has also linked weaker social relationships to dementia risk, although studies vary in how they measure loneliness, isolation, depression, and baseline cognition.3
Mismatch matters: McHugh et al. showed that loneliness and objective isolation do not collapse into one construct in later life.4 A person's perceived belonging can diverge from network size, and that divergence may identify a different risk profile than simple contact counts.
- Clinical route: loneliness may reduce sleep quality, medication adherence, activity, and preventive care.
- Disease route: chronic illness can restrict social participation and increase perceived loneliness.
- Bidirectional route: cognitive decline can make social interaction harder, which can worsen loneliness.
Evidence-Strength Note for This Longitudinal Analysis
What the design supports: this analysis can support temporal association because social measures, health burden, and later cognition were modeled across waves with covariate adjustment. It also tested specific mediators rather than treating loneliness as a vague exposure.
Causal limits: observational modeling cannot prove the direction of causation. Chronic disease could increase loneliness mismatch, loneliness mismatch could worsen disease management, or a third factor such as depression, poverty, pain, sleep apnea, or early cognitive change could influence both.
Generalizability also needs care. The main biomarker sample was mostly White, middle-aged to older, and healthier than many clinical populations. Screening implications may differ in racially diverse, immigrant, rural, disabled, or lower-income groups where social access and chronic disease management are shaped by different constraints.
What Screening Should Do With a Loneliness Mismatch
A loneliness mismatch should not be treated as a stand-alone cognitive screening result. It works better as a prompt to check the ordinary but powerful risk pathways: untreated hypertension, diabetes, sleep apnea, chronic pain, depression, hearing loss, social barriers, medication burden, and missed preventive care.
Practical use: when a patient reports loneliness despite regular contact, clinicians should ask whether the person feels emotionally understood, whether chronic illness limits participation, and whether medical symptoms are shrinking the person's world. The cognitive implication comes through those pathways, not through loneliness as a mystical exposure.
Chronic Disease Gives the Finding a Concrete Intervention Surface
Loneliness is hard to prescribe against when the problem is a person's subjective experience of connection. Chronic disease burden gives the signal a more actionable surface. Blood pressure control, diabetes care, sleep-apnea evaluation, hearing support, pain treatment, mobility support, depression treatment, and medication simplification are ordinary clinical levers that can reduce cognitive risk and make social life easier to sustain.
Care-planning implication: a patient who feels lonely despite regular contact may need more than a social referral. The stronger pathway in this analysis points toward medical complexity: multimorbidity, fatigue, pain, sleep disruption, and functional limits that can make existing relationships feel thin or hard to use.
- For primary care: loneliness mismatch can flag chronic disease review and cognitive-risk counseling.
- For mental health care: loneliness should be separated from depression, anxiety, trauma avoidance, and grief rather than treated as one mood symptom.
- For aging services: social programs may work better when paired with transportation, hearing, mobility, and disease-management support.
Cognitive endpoint caution: episodic memory and executive function are useful early signals, but they are not dementia diagnoses. A small average memory association can still matter if it identifies a pathway that accumulates across years: more chronic illness, more medication burden, less activity, poorer sleep, and fewer cognitively demanding social roles.
Screening should therefore move in 2 directions at once. Ask about felt connection in ordinary language, then check the medical conditions that may be narrowing the person's ability to participate. The combination is more informative than counting phone calls or assuming that network size captures support quality.
Program design: a social-prescribing referral is more likely to work when the person can physically and cognitively use it. Transportation help, hearing support, pain control, sleep treatment, medication simplification, and chronic-disease follow-up may determine whether a group visit, volunteer call, or community activity actually becomes meaningful connection.
That makes intervention matching essential. A lonely person with uncontrolled pain needs a different plan than a socially isolated person with no transportation or a bereaved person with intact health.
The mismatch points to assessment before referral.
That keeps support targeted.
Specificity matters.
Questions About Loneliness, Isolation, and Cognition
Is loneliness the same thing as social isolation?
No. Loneliness is the subjective feeling of being disconnected. Social isolation is more objective: fewer contacts, roles, or interactions.
What did this study add?
It modeled the loneliness surplus after objective isolation was considered, then tested whether chronic disease burden or allostatic load helped explain later cognitive scores.
Does lowering loneliness prevent dementia?
This analysis cannot prove prevention. It supports checking chronic disease pathways when loneliness and objective social contact do not line up.
References
- Discrepancies in loneliness and social isolation predict cognitive impairment through chronic disease burden. Cintron DW, Narvaez Linares NF, Surachman A, et al. Brain, Behavior, & Immunity – Health. 2026;48:101232. doi:10.1016/j.bbih.2026.101232
- Perceived social isolation and cognition. Cacioppo JT, Hawkley LC. Trends in Cognitive Sciences. 2009;13:447–454. doi:10.1016/j.tics.2009.06.005
- Social relationships and risk of dementia: a systematic review and meta-analysis of longitudinal cohort studies. Kuiper JS, Zuidersma M, Oude Voshaar RC, et al. Ageing Research Reviews. 2015;22:39–57. doi:10.1016/j.arr.2015.04.006
- Social isolation, perceived isolation and health among older adults. McHugh Power JE, Hannigan C, Hyland P, et al. International Journal of Geriatric Psychiatry. 2017;32:135–144. doi:10.1002/gps.4509