A 2026 Shanghai study of 1,589 preschoolers found that children sleeping ≤9 hours at night had higher parent-rated anxiety scores than children sleeping >10 hours. The effect sizes were small, but the pattern appeared across total anxiety, physical injury fears, social phobia, obsessive-compulsive symptoms, and generalized anxiety symptoms.1
Research Highlights
- 1,589 preschoolers were analyzed: Zhang et al. collected sleep and anxiety questionnaires from 2 public kindergartens in Shanghai; mean age was 4.58 years and 52.2% were male.1
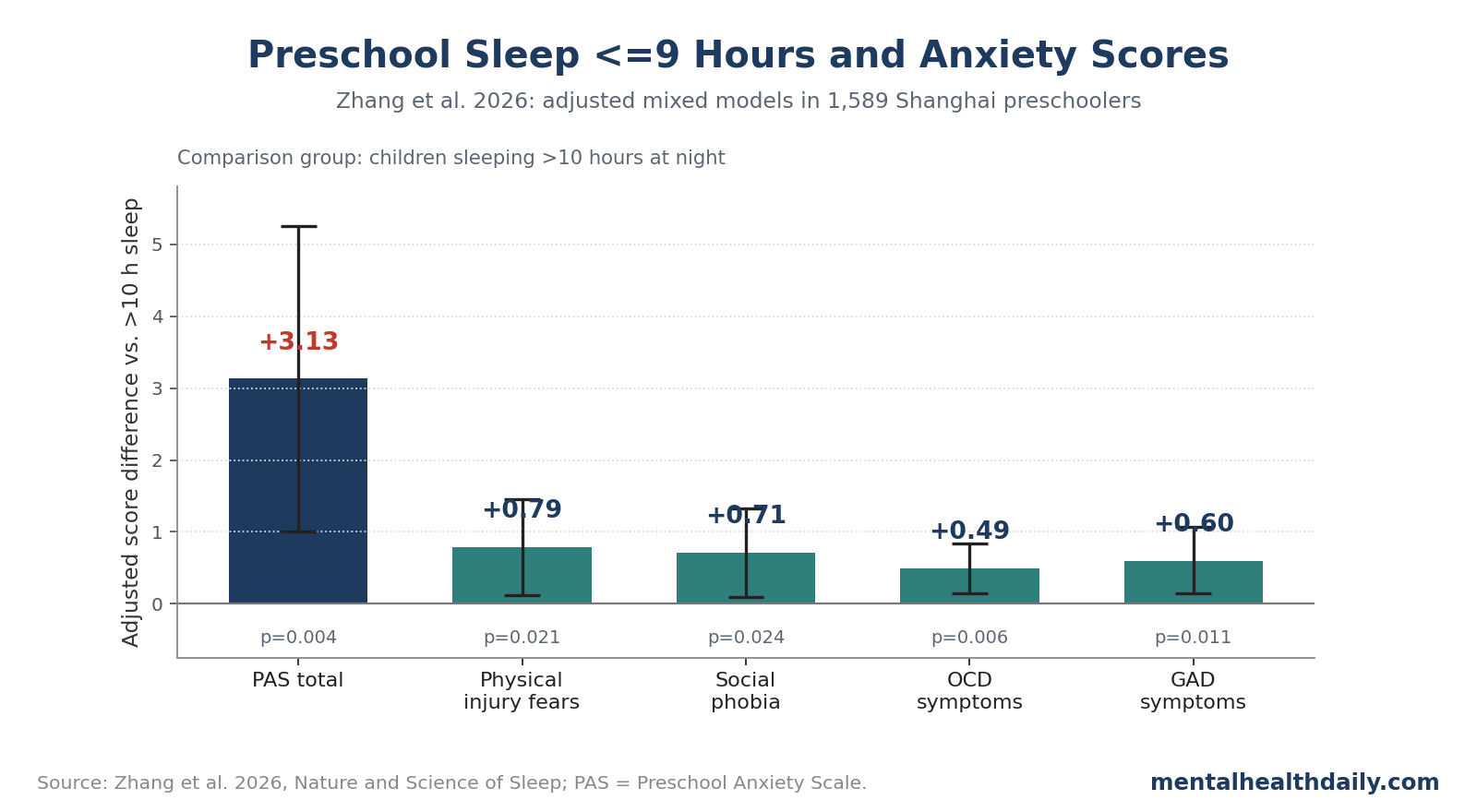
- ≤9 hours of nighttime sleep tracked higher anxiety: compared with >10 hours, the adjusted Preschool Anxiety Scale total score was 3.13 points higher (95% CI 1.01-5.25, p = 0.004).1
- Several subdomains moved in the same direction: physical injury fears, social phobia, obsessive-compulsive symptoms, and generalized anxiety symptoms were all higher in the ≤9-hour group.1
- The study was cross-sectional: it cannot prove that short sleep caused anxiety; anxious children may also sleep less, and family routines can affect both sleep and anxiety ratings.1
- Night sleep may not be replaceable by naps: the association persisted in weekday-only analyses despite China's kindergarten nap policy, suggesting that daytime napping may not fully offset short nighttime sleep.1
Preschool anxiety has a child-specific clinical shape. It can appear as physical fears, separation distress, social avoidance, repetitive worries, irritability, and bedtime resistance, which makes sleep-anxiety interpretation especially tricky.2
Zhang et al. Compared 3 Nighttime Sleep Groups
The study used parent-reported sleep duration from the Children's Sleep Habits Questionnaire (CSHQ) and anxiety symptoms from the Preschool Anxiety Scale (PAS). PAS is a parent-rated scale that includes separation anxiety, physical injury fears, social phobia, obsessive-compulsive symptoms, and generalized anxiety symptoms.1
The final sample had 1,589 children after excluding incomplete questionnaires. Average nighttime sleep was 9.37 hours, and the prevalence of significant anxiety symptoms was 2.14%.
The sleep groups were:
- ≤9 hours per night: 423 children.
- >9 to ≤10 hours per night: 976 children.
- >10 hours per night: 190 children.
The sample also had useful demographic detail. Mean age was 4.58 years, 48.96% were only children, and parents were the main caregiver for 67.09% of participants. Average CSHQ total score was 47.10, suggesting sleep problems were common enough to analyze as a developmental health domain rather than a rare complaint.1
The comparison that carried the signal was the shortest-sleep group vs. the longest-sleep group. The middle group usually sat between them and did not show the same adjusted differences.
This design is useful for screening-level signal detection, but it is not a sleep-lab study. It did not use actigraphy, polysomnography, or objective sleep staging. Parent report can be informative in large child samples, but it can also misestimate sleep onset, night waking, and weekday-weekend variation.3
≤9 Hours Was Linked to Higher Total Anxiety Score
The main adjusted estimate was a 3.13-point higher PAS total score in children sleeping ≤9 hours compared with children sleeping >10 hours. The 95% confidence interval was 1.01-5.25, and p = 0.004.1
Plain English: after adjusting for age, sex, only-child status, and main caregiver, the shortest-sleep group had higher anxiety scores than the longest-sleep group. The effect was statistically detectable but not large; Cohen's d was 0.25, which is generally considered small.
The subscale pattern was broader than one anxiety item:
- Physical injury fears: beta = 0.79, 95% CI 0.12-1.46, p = 0.021.
- Social phobia: beta = 0.71, 95% CI 0.09-1.33, p = 0.024.
- Obsessive-compulsive symptoms: beta = 0.49, 95% CI 0.14-0.84, p = 0.006.
- Generalized anxiety symptoms: beta = 0.60, 95% CI 0.14-1.07, p = 0.011, although the overall GAD model p-value was 0.056.
- Separation anxiety: beta = 0.54, 95% CI −0.20 to 1.09, p = 0.058.
That last line is important. Separation anxiety pointed in the same direction but did not meet the conventional p < 0.05 threshold. The better interpretation is a broad short-sleep anxiety gradient, not a clean finding in every subscale.
Small Effects Can Still Matter in Early Childhood
A Cohen's d of 0.19-0.25 is not a dramatic individual-level effect. Many children below 9 hours will be fine, and many children above 10 hours will still have anxiety symptoms for other reasons.
Small effects can still have public-health meaning when the exposure is common. Sleep duration is shaped by school start routines, parent work schedules, evening screen use, co-sleeping patterns, light exposure, and household stress. When many children are exposed, even a small shift in anxiety score can mark a useful prevention target.
The result also fits the broader pediatric sleep literature. Sleep problems and anxiety frequently travel together, and longitudinal work has linked shorter nighttime sleep with later emotional and behavioral difficulties in young children.4,5
The causal direction is probably bidirectional in many families:
- Short sleep can increase emotional reactivity. Tired children may have weaker regulation of fear, frustration, and uncertainty.
- Anxiety can disrupt sleep. Worry, separation fears, bedtime resistance, and physiological arousal can shorten sleep.
- Family routines can affect both. Irregular bedtimes, caregiver stress, noise, screen exposure, and inconsistent schedules can raise anxiety and reduce sleep.
That is why the study should not be turned into a simple blame frame. The clinical use is not “parents caused anxiety by letting children sleep too little.” It is “nighttime sleep is a modifiable domain worth checking when preschool anxiety is present.”
The reverse pathway deserves equal attention. A preschooler with physical fears, social avoidance, or repetitive worries may stretch bedtime because nighttime separation feels threatening. In that situation, the sleep problem is partly an anxiety symptom, not a separate habit failure.
That changes the intervention. Bedtime consistency can help, but a child whose anxiety is driving bedtime conflict may also need graduated separation practice, parent coaching, daytime anxiety work, or evaluation for broader emotional problems.
Daytime Naps May Not Offset Short Night Sleep
China's kindergarten policy includes a 2-2.5-hour daytime nap window. In theory, a long nap could make shorter nighttime sleep less concerning if total 24-hour sleep remains adequate.
Zhang et al. treated that as a real issue rather than ignoring it. Their weekday-only analysis still found the ≤9-hour threshold associated with higher anxiety symptoms, with effect sizes similar to the primary analysis.1
That does not prove naps are useless. It suggests that night sleep has features that daytime sleep may not fully replace: circadian timing, consolidated sleep architecture, parent-child bedtime routines, and morning wake pressure.
Sleep recommendations for preschoolers usually focus on total sleep across 24 hours. The Shanghai result adds a more specific question for clinicians and parents: is the child getting enough sleep at night, including enough consolidated sleep before morning wake time?6
This distinction is also culturally relevant. East Asian preschool sleep patterns can include later bedtimes, co-sleeping, and scheduled naps, so direct importation of Western nighttime sleep norms can be crude. The useful part of the study is not a universal moral rule about 9 hours. It is evidence that in this Shanghai sample, ≤9 hours of nighttime sleep marked higher anxiety scores.
A practical sleep review should ask concrete questions instead of stopping at total hours:
- Bedtime: how late lights-out happens on school nights.
- Wake time: whether the child is being awakened before natural sleep offset.
- Sleep onset: how long it takes the child to fall asleep.
- Night waking: whether sleep is fragmented even when total time in bed looks adequate.
- Weekend catch-up: whether the child sleeps much later on weekends, suggesting weekday restriction.
Those details are more useful than telling every family to hit a single number. A child sleeping 9 hours with fast sleep onset, stable wake time, and good daytime mood may need different guidance than a child sleeping 9.5 hours with long bedtime conflict and repeated night waking.
Limitations of This Preschool Sleep Study
- Cross-sectional design. Sleep and anxiety were measured at the same time, so causal direction is unresolved.
- Parent-reported sleep. CSHQ data are practical for large samples, but they are less precise than actigraphy or polysomnography.
- Shanghai sampling. The sample came from 2 public kindergartens, which limits generalization to rural China, private schools, and other countries.
- Low positive-screen rate. Only 2.14% met the significant-anxiety threshold, so the result is mainly about symptom-score gradients, not diagnosed anxiety disorder.
- No upper-threshold answer. The study could not clarify whether very long nighttime sleep carries separate risk because the >10-hour group was small.
Questions About Preschool Sleep and Anxiety
Does this prove that less than 9 hours causes anxiety?
No. The study showed an association. Anxiety can also shorten sleep, and household routines can influence both.
Was the effect large?
No. The adjusted differences were small, but they were consistent across several anxiety domains.
Should parents focus on nighttime sleep or total daily sleep?
Both are useful, but this study specifically points toward nighttime sleep. A long nap may not fully compensate for a short night.
Which sleep questions should parents check first?
Check bedtime timing, wake time, night waking, screen exposure, and caregiver stress before jumping to supplements or medication. For persistent anxiety symptoms, pediatric or mental-health evaluation is more appropriate than sleep hygiene alone.
References
- Zhang L, Hu Y, He D, et al. The relationship between night sleep duration and anxiety in preschool aged children. Nature and Science of Sleep. 2026;18:1-12. doi:10.2147/nss.s593442
- Spence SH, Rapee R, McDonald C, Ingram M. The structure of anxiety symptoms among preschoolers. Behavior Research and Therapy. 2001;39:1293-1316. doi:10.1016/s0005-7967(00)00098-x
- Werner H, Molinari L, Guyer C, Jenni OG. Agreement rates between actigraphy, diary, and questionnaire for children's sleep patterns. Archives of Pediatrics & Adolescent Medicine. 2008;162:350-358. doi:10.1001/archpedi.162.4.350
- Zheng M, Rangan A, Olsen NJ, Heitmann BL. Longitudinal association of nighttime sleep duration with emotional and behavioral problems in early childhood. Sleep. 2021;44:zsaa138. doi:10.1093/sleep/zsaa138
- Deng Y, Zhang Z, Gui Y, et al. Sleep disturbances and emotional and behavioral difficulties among preschool-aged children. JAMA Network Open. 2023;6:e2347623. doi:10.1001/jamanetworkopen.2023.47623
- Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation's sleep time duration recommendations. Sleep Health. 2015;1:40-43. doi:10.1016/j.sleh.2014.12.010