A 2026 mechanistic review linked microplastics to 6 proposed Alzheimer’s disease pathways and 6 proposed Parkinson’s disease pathways.1 The calibrated interpretation is that microplastics are biologically plausible brain stressors, but the human evidence does not yet prove that they cause Parkinson’s disease or Alzheimer’s disease.
Research Highlights
- Exposure is widespread: the review cited an estimate that adults may ingest up to 121,000 microplastic particles per year, with more than 90% cleared but a persistent fraction still biologically concerning.
- Alzheimer’s mechanisms clustered into 6 pathways: blood-brain barrier disruption, chronic inflammation, reactive oxygen species, mitochondrial dysfunction, impaired autophagy/proteostasis, and epigenetic changes.
- Parkinson’s mechanisms also clustered into 6 pathways: barrier disruption, dopaminergic oxidative stress, mitochondrial dysfunction, microglial neuroinflammation, α-synuclein aggregation, and gut-brain signaling.
- Human causality remains unproven: tissue-detection and experimental studies support plausibility, but 0 prospective human studies can yet turn exposure into a reliable individual risk estimate.
- Policy logic is stronger than clinical prediction: reducing plastic exposure may be sensible public-health hygiene, but it is not a validated 2026 Parkinson’s or Alzheimer’s prevention treatment.
Microplastics are plastic fragments smaller than 5 mm; nanoplastics are usually defined as particles below 1 μm. Size matters because smaller particles are more likely to cross biological barriers, interact with cells, and carry additives or absorbed pollutants into tissues.
Blood-brain barrier means the tightly regulated vascular interface that normally limits what enters brain tissue from blood. If particles or particle-triggered inflammation weaken that barrier, the concern includes direct plastic entry, immune activation, oxidative stress, and disrupted nutrient or waste exchange.
121,000 Particles Per Year Is Exposure, Not Disease Risk
Siu et al. opened with a striking exposure estimate: an average adult may ingest up to 121,000 microplastics annually. They also noted that the body may eliminate more than 90% of ingested particles, leaving the key question in the residual fraction that persists or reaches sensitive tissues.1
That distinction prevents overclaiming. Exposure is not the same as a quantified disease risk. A person can encounter particles without developing neurodegeneration, and a person with Parkinson’s disease or Alzheimer’s disease has many possible genetic, vascular, metabolic, inflammatory, and age-related contributors.
Practical interpretation: microplastics are best treated as a plausible chronic stressor in a larger risk network, not as a single-cause explanation for neurodegenerative disease.
Microplastics Map Onto Known Neurodegeneration Pathways
The reason the topic deserves attention is that the proposed pathways are not exotic. Parkinson’s disease already involves dopaminergic neuron vulnerability, mitochondrial stress, neuroinflammation, lysosomal-autophagy problems, and α-synuclein aggregation. Alzheimer’s disease already involves amyloid, tau, vascular dysfunction, oxidative stress, and clearance failure.
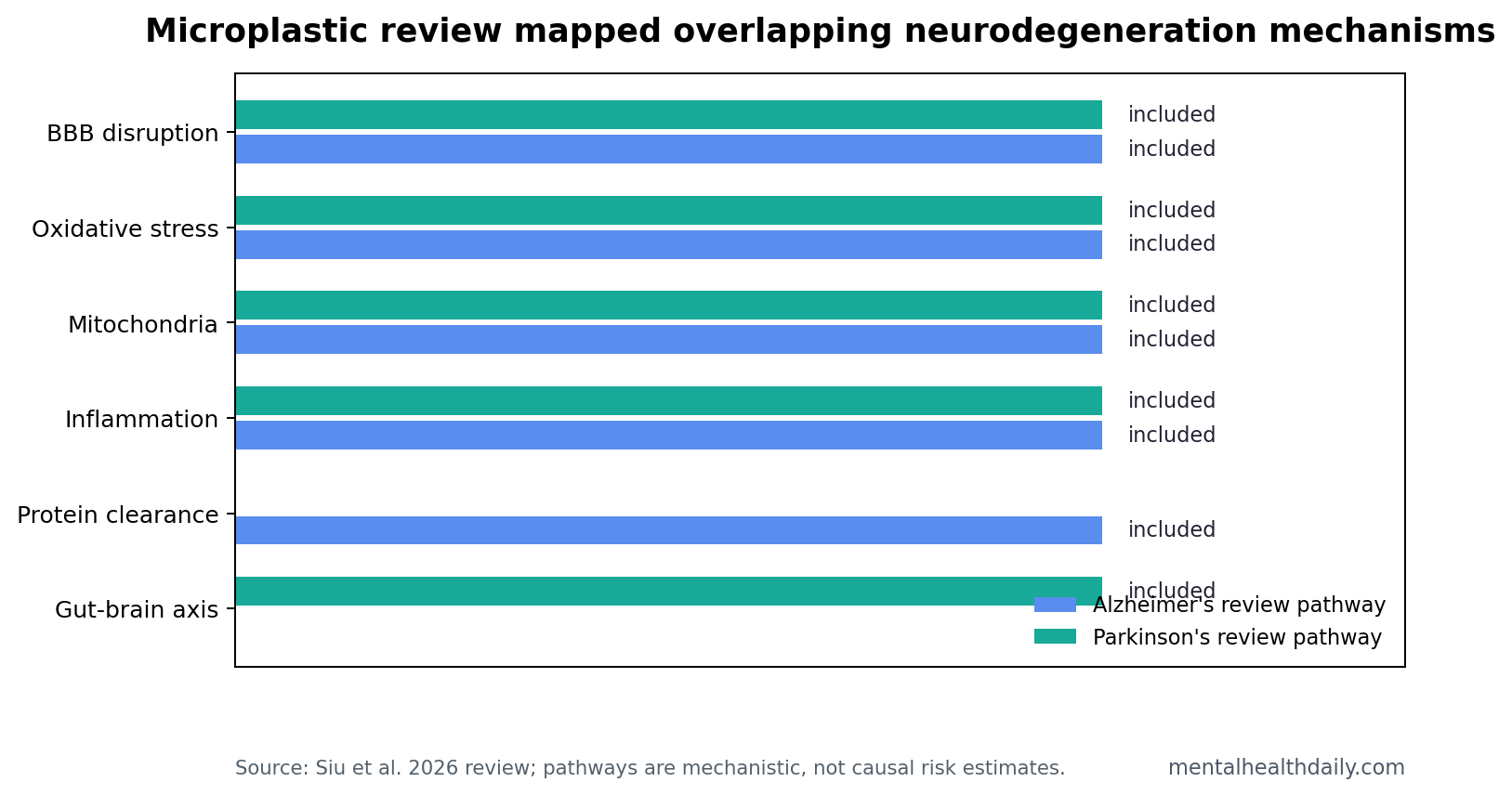
Siu et al. mapped microplastic exposure onto these familiar mechanisms.1
- Alzheimer’s disease pathways: blood-brain barrier disruption, chronic inflammation, oxidative stress and reactive oxygen species, mitochondrial dysfunction, impaired autophagy/proteostasis, and epigenetic alteration.
- Parkinson’s disease pathways: blood-brain barrier disruption, oxidative stress in dopaminergic neurons, mitochondrial dysfunction, microglial-driven neuroinflammation, α-synuclein aggregation, and gut-brain-axis disruption.
Why overlap matters: a weak environmental exposure claim becomes more plausible when it lines up with independent disease biology. But overlap still cannot prove causation. Many stressors can trigger oxidative stress, mitochondrial dysfunction, or inflammation in cells without causing human Parkinson’s disease.
Mechanism specificity: the most useful microplastic studies will need to show more than generic cell stress. A Parkinson’s-relevant experiment should connect exposure to dopaminergic injury, α-synuclein handling, mitochondrial function, or gut-brain signaling. An Alzheimer’s-relevant experiment should connect exposure to barrier leakage, amyloid or tau handling, vascular injury, or clearance failure.
Brain Entry Is Plausible Through Barrier, Blood, and Olfactory Routes
The review described several routes by which microplastics might reach or affect the brain. Particles may move from the gut into blood, interact with endothelial cells at the blood-brain barrier, or enter through inhalation and olfactory pathways that bypass some barrier protections.1
Particle size, surface charge, aging, and chemical coating change the biological problem. Weathered particles can differ from pristine laboratory particles because environmental exposure can alter surface oxidation and adsorbed chemical load. That means a clean plastic bead in a dish is not always a good substitute for what a person inhales or ingests.
Evidence-strength note: much of the mechanistic evidence comes from cell, animal, or tissue-detection work. Those designs can show exposure routes and biological responses. They cannot show that ordinary human exposure causes a particular neurodegenerative diagnosis years later.
Parkinson’s Plausibility Runs Through Dopamine, Alpha-Synuclein, and the Gut
Parkinson’s disease is especially relevant because its biology already includes environmental sensitivity, mitochondrial impairment, oxidative stress in dopaminergic neurons, misfolded α-synuclein, and gut-brain signaling. The review placed microplastics inside that map rather than claiming a new standalone cause.
Dopaminergic vulnerability: dopamine-producing neurons in the substantia nigra are metabolically demanding and sensitive to oxidative stress. A particle exposure that increases reactive oxygen species or disrupts mitochondrial function could, in theory, worsen a pathway already central to Parkinson’s disease.
Protein handling: α-synuclein aggregation depends partly on cellular stress, lysosomal function, inflammation, and proteostasis. Microplastic-linked autophagy and proteostasis disruption is therefore relevant, but the current evidence does not show that particles initiate Lewy pathology in humans.
Gut-brain signaling: Parkinson’s disease often includes constipation and other non-motor symptoms before diagnosis. A gut exposure that alters inflammation, barrier function, or microbial signaling is plausible enough to study, especially because the gut is a major exposure site for ingested microplastics.
Alzheimer’s Plausibility Runs Through Barrier Failure and Clearance
Alzheimer’s disease includes amyloid and tau pathology alongside vascular injury, blood-brain barrier leakage, neuroinflammation, impaired waste clearance, and mitochondrial stress. Microplastic mechanisms intersect with those processes in the review.
The most important bridge is barrier biology. If microplastics or particle-induced inflammation compromise the blood-brain barrier, the downstream problem could include immune-cell signaling, altered amyloid clearance, oxidative stress, and vascular dysfunction. Those processes are already implicated in Alzheimer’s disease and cognitive decline.2
Still, Alzheimer’s disease develops over decades. A mechanistic review cannot estimate whether microplastics add a large, small, or negligible amount of risk compared with age, APOE genotype, vascular disease, sleep, diabetes, traumatic brain injury, hearing loss, and other established factors.
How to Act Without Turning Plausibility Into Panic
The strongest action case is environmental and public-health oriented. Less plastic shedding, better water and food packaging standards, air-quality attention, and reduced unnecessary plastic exposure can be justified without claiming that microplastics are a proven dementia or Parkinson’s cause.
For individual readers, the evidence supports modest exposure hygiene rather than medical fear. Filtered drinking water, less heating of food in plastic, attention to indoor dust, and reduced disposable plastic use are reasonable low-risk steps. They should not replace exercise, blood-pressure control, sleep treatment, hearing correction, smoking cessation, diabetes management, or evidence-based neurological care.
Research standard: the next useful studies need measured exposure, tissue or blood biomarkers, longitudinal follow-up, and disease-relevant endpoints. Cross-sectional detection studies and animal dosing experiments can identify mechanisms, but prevention claims need years of human data.
That standard also protects against panic marketing. A product that claims to detox microplastics or prevent dementia would need evidence that it reduces measured exposure, changes disease-relevant biology, and improves clinical endpoints. The 2026 review does not provide that chain, and ordinary exposure-reduction advice should stay separate from treatment claims. Plausibility is enough for research priority, not diagnosis.
What Would Make the Human Evidence Stronger?
A convincing human study would need to measure microplastic exposure before disease develops, not after diagnosis. That means repeated sampling of drinking water, diet, air, household dust, occupational exposure, and possibly blood or stool particle burden, followed by years of neurological follow-up.
Exposure measurement: particle counts should separate polymer type, particle size, surface chemistry, and additives. A 5 μm polystyrene particle, a weathered tire-wear fragment, and a nanoplastic particle carrying a persistent organic pollutant are not interchangeable exposures.
Biological markers: useful studies would pair exposure with inflammation markers, oxidative-stress markers, blood-brain barrier markers, olfactory function, constipation, sleep behavior disorder, cognitive testing, and imaging where feasible. That would help distinguish “particles are present” from “particles are changing disease-relevant biology.”
Clinical endpoints: Parkinson’s diagnosis, mild cognitive impairment, Alzheimer’s dementia, rate of cognitive decline, and prodromal non-motor symptoms need to be analyzed separately. A broad “brain health” endpoint would blur the mechanism the review is trying to clarify.
Confounder control: age, smoking, pesticide exposure, air pollution, traumatic brain injury, diabetes, hypertension, APOE genotype, occupation, and socioeconomic factors would all need to be handled carefully. Plastic exposure may track other environmental risks, so a crude exposure-disease correlation could mislead in either direction.
Questions About Microplastics and Brain Disease
Does this review prove that microplastics cause Parkinson’s disease?
No. It identifies mechanisms that overlap with Parkinson’s biology, including oxidative stress, mitochondrial dysfunction, neuroinflammation, α-synuclein aggregation, and gut-brain signaling. That is plausibility, not proof.
Does this review prove that microplastics cause Alzheimer’s disease?
No. The Alzheimer’s argument is also mechanistic: barrier disruption, inflammation, mitochondrial stress, impaired protein clearance, and epigenetic changes are plausible links, but human causal risk remains unknown.
Is reducing plastic exposure still sensible?
Yes, as general exposure hygiene and environmental policy. The evidence is not strong enough to present microplastic avoidance as a validated neurodegeneration-prevention intervention.
References
- Siu ACW, Paudel KR, Singh G, et al. Do microplastics play a role in the pathogenesis of neurodegenerative diseases? Shared pathophysiological pathways for Alzheimer’s and Parkinson’s disease. Molecular and Cellular Biochemistry. 2026;481:669-694. https://doi.org/10.1007/s11010-025-05428-3
- GBD 2021 Nervous System Disorders Collaborators. Global, regional, and national burden of disorders affecting the nervous system, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Neurology. 2024. https://doi.org/10.1016/s1474-4422(24)00038-3
- PubMed search: human tissue microplastics and brain accumulation. https://pubmed.ncbi.nlm.nih.gov/?term=microplastics+human+brain+tissue
- PubMed search: weathered microplastics oxidative stress microglia. https://pubmed.ncbi.nlm.nih.gov/?term=weathered+microplastics+oxidative+stress+microglia