
A 2026 mixed-methods preprint found that iSupport-Malaysia, a multimedia web-based dementia caregiver psychoeducation program, reached a good System Usability Scale score of 74.3. That is enough to justify pilot testing, but not enough to claim caregiver mental-health benefit: 33.3% of usability-test participants failed sign-up, 20.0% failed search, and Loh et al. did not measure burden, depression, anxiety, or sustained use.1
Research Highlights
- Usability was good, not finished: iSupport-Malaysia scored 74.3 on the System Usability Scale, above the usual 68 benchmark, with caregivers rating it 76.1 and healthcare professionals rating it 71.7.1
- Access friction was concentrated early: 5 of 15 participants could not complete sign-up, and 3 of 15 could not complete the search task during usability testing.1
- Lesson-level tasks had higher completion: once participants reached a lesson page, 80.0% watched videos without assistance, 86.7% completed quizzes without assistance, and 80.0% downloaded handouts without assistance.1
- Caregivers wanted practical fit: feedback favored self-paced learning, handouts, and peer sharing, while warning that cartoons, long videos, right/wrong quizzes, small fonts, and mobile layouts could undermine use.1
- Effectiveness is still untested: adjacent dementia caregiver studies suggest remote support can help, but this preprint was a cultural-adaptation and usability study, not an outcomes trial.23
iSupport-Malaysia is a localized version of the World Health Organization’s iSupport for Dementia program, designed to teach family and paid caregivers about dementia symptoms, daily care, communication, behavior management, and caregiver self-care. The Malaysian adaptation translated the program into Bahasa Malaysia, changed names and scenarios to fit local family caregiving, added local resources, and rebuilt the lessons as 23 multimedia modules hosted on OpenLearning.
The calibrated read is narrow but useful: the platform appears usable among educated, internet-using Malaysian caregivers and professionals, while the exact points where people got stuck tell developers what must be repaired before a larger trial.
74.3 on Usability Supports Pilot Testing, Not Clinical Benefit
System Usability Scale (SUS) is a 0-100 questionnaire used to rate whether a website, app, or digital tool feels usable to intended users. Loh et al. reported a mean SUS score of 74.3 with a standard deviation of 18.0, which falls in the good range rather than the excellent range.1
Caregivers rated the platform slightly higher than healthcare professionals: 76.1 vs. 71.7. That split matters because the 2 groups were judging different things. Caregivers emphasized immediate usefulness, emotional fit, and whether lessons matched real caregiving problems. Professionals focused more on comprehensiveness, clinical sequencing, and whether caregivers might skip foundational material.
The study design cannot answer whether iSupport-Malaysia reduces caregiver burden, depression, anxiety, distress, or social isolation. It can only say that a small group of target users and professionals found the prototype usable enough to refine.
Evidence-strength note: this was a preprint, mixed-methods usability study with 35 total participants and 15 people in usability testing. It supports design iteration and feasibility planning, not treatment-effect claims.
Sign-Up and Search Were the Main Failure Points
The usability data make the implementation problem concrete. Participants were asked to complete 7 tasks: sign up, find a lesson, watch a video, complete a quiz, download a handout, use search, and check progress.1
The hardest step came before any dementia education could happen. Only 40.0% completed sign-up without assistance, 26.7% completed it with assistance, and 33.3% did not complete it. Problems included password requirements, forgotten OpenLearning credentials, and platform technical issues.
Search also created friction. Only 53.3% completed the search task without assistance, 26.7% needed assistance, and 20.0% did not complete it. Participants could not find the search button, typed in English rather than Malay, or entered long phrases instead of keywords.
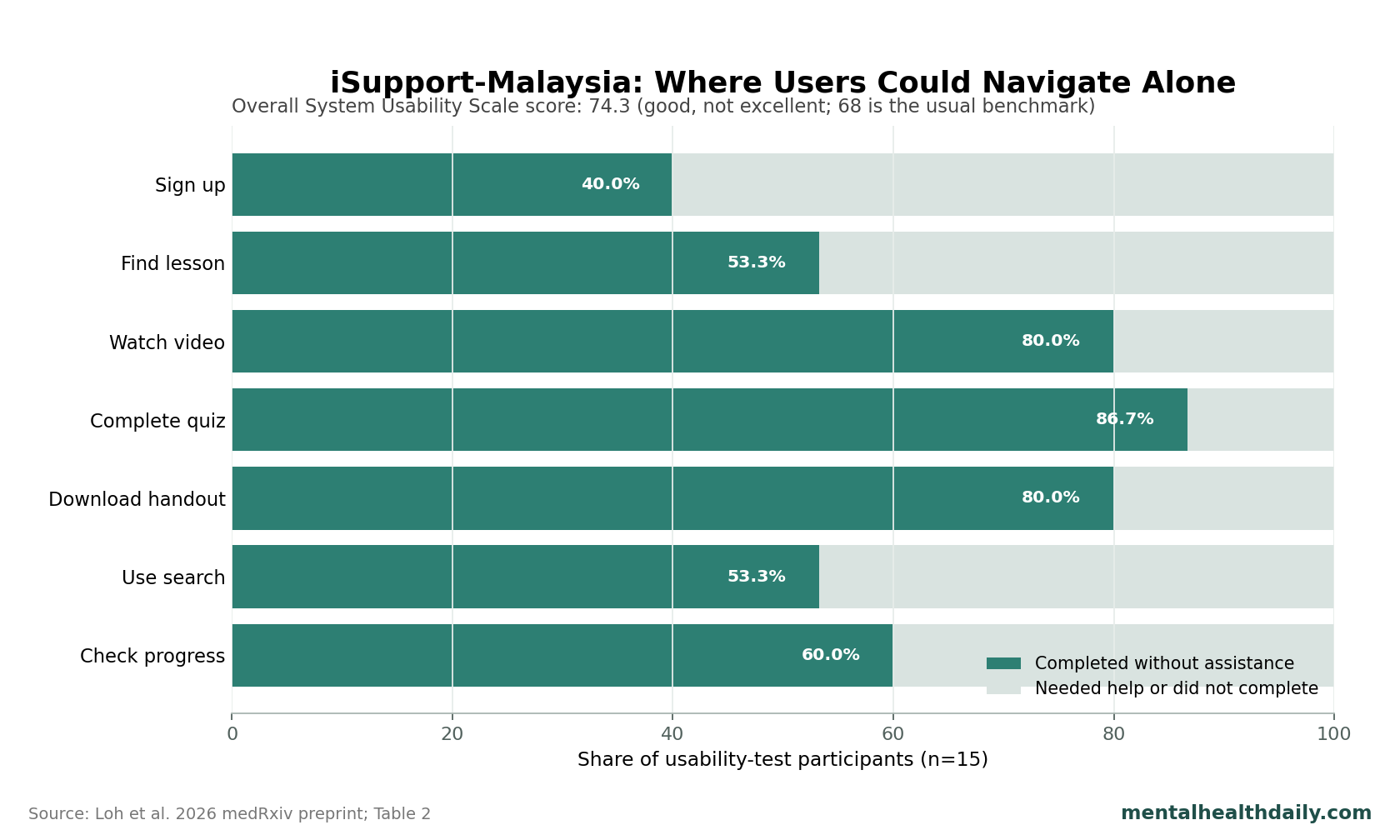
Lesson access: finding a specific lesson also required help for 46.7% of participants, even though no one failed the task entirely. A caregiver support program can look useful after entry but still lose users at the front door.
Videos, Handouts, and Peer Sharing Worked Better Than Quizzes
Once participants were inside a lesson, performance improved. Watching videos, completing quizzes, and downloading handouts had 80.0-86.7% independent completion rates. Difficulty ratings were also highest for handout download, with a mean of 4.27 on a 1-5 scale.1
Qualitative feedback separated helpful multimedia from distracting multimedia. Healthcare professionals often liked cartoon-style videos, while several caregivers found them distracting, too long, or too light for a serious caregiving problem. The practical design lesson is not “more video”; it is shorter, clearer, emotionally appropriate video.
- Handouts: participants saw downloadable summaries as practical tools that could be kept, printed, or revisited.
- Reflection exercises: caregivers liked peer-sharing opportunities because dementia caregiving often involves isolation and trial-and-error problem solving.
- Quizzes: right/wrong scoring felt invalidating when caregiving situations did not have one clean answer.
- Worksheets: PDF exercises seemed less useful when no facilitator was available to help caregivers apply them.
That pattern fits dementia caregiver support more broadly. Remote education is most likely to help when it reduces isolation and gives caregivers usable scripts, not when it turns messy family care into school-like testing.
Malaysia-Specific Adaptation Was More Than Translation
The adaptation changed language, examples, character names, family roles, local resources, and delivery format. Case scenarios were revised to reflect Malaysia’s Malay, Chinese, and Indian communities, and the program added memory clinics, dementia associations, and nonprofit daycare centers.1
Cultural adaptation means changing an evidence-based intervention so it fits local language, customs, literacy, family expectations, and service pathways while preserving the core intervention logic. For dementia caregiving in Malaysia, family-based care and filial duty are not background details; they shape who does the work, who asks for help, and how acceptable outside support feels.
The study also showed where adaptation remained incomplete. Participants flagged formal language, medical jargon, gendered caregiving assumptions, insufficient mid- and late-stage dementia content, and limited mobile accessibility. Those are not cosmetic issues. A caregiver who is working, exhausted, and caring for a parent with advanced dementia may abandon a platform that feels visually cramped, too early-stage, or morally judgmental.
Remote Dementia Caregiver Trials Still Need Outcome Data
Loh et al. cited a Malaysian telephone-delivered iSupport intervention that reduced caregiver burden, anxiety, and distress.2 That earlier trial matters because it suggests iSupport content can move mental-health outcomes when delivered with human support.
Online iSupport evidence from India also moved beyond pure usability: Baruah et al. tested an online training and support program for dementia caregivers in a randomized feasibility study.3 Portugal’s iSupport usability work provides another comparator, and the Malaysian preprint reported that Portugal’s usability score was 89.5, higher than the 74.3 score in iSupport-Malaysia.4
Those comparisons do not make the Malaysian multimedia platform ineffective. They clarify the next test. A fully self-guided multimedia version may scale better than telephone support, but scale is useful only if caregivers can enter, navigate, trust, and continue using the platform long enough for learning to affect daily care.
Broader reviews of internet-based and remotely delivered dementia caregiver support reach the same practical endpoint: usability, acceptability, caregiver burden, and sustained engagement are implementation variables, not afterthoughts.56
What the Pilot Trial Should Measure
The next iSupport-Malaysia trial should not treat usability as already solved. It should preserve the platform improvements from this study and measure whether those changes improve access, completion, and caregiver outcomes.
- Entry friction: sign-up completion, password problems, need for technical support, time from invitation to first lesson, and drop-off before module 1.
- Navigation quality: search success, lesson-finding success, mobile completion, font and contrast complaints, and progress-checking accuracy.
- Caregiver outcomes: burden, depressive symptoms, anxiety, distress, confidence, dementia knowledge, and perceived support.
- Engagement dose: lessons started, lessons completed, videos watched, handouts downloaded, comments posted, and return visits over weeks rather than one test session.
- Equity of reach: rural caregivers, older caregivers, lower-literacy users, male caregivers, and families caring for people with mid- or late-stage dementia.
Clinical implication: the platform should be treated as a promising caregiver-support infrastructure project. It is not yet evidence that unsupported web lessons can reduce Malaysian caregiver burden on their own.
Questions About iSupport-Malaysia
Does a 74.3 usability score mean iSupport-Malaysia is ready for national rollout?
No. A 74.3 SUS score supports refinement and pilot testing. National rollout would need evidence on completion, sustained use, caregiver burden, mental-health outcomes, technical support needs, and reach among less digitally confident caregivers.
Why did lesson tasks work better than sign-up and search?
Lesson tasks were concrete once users arrived at the correct page. Sign-up and search required platform navigation, password handling, language choices, and interface discovery before caregiving content was visible.
Should dementia caregiver programs use quizzes?
Quizzes can reinforce learning, but dementia caregiving often involves ambiguous situations. Feedback that offers options and reassurance may fit caregivers better than right/wrong scoring.
What is the strongest claim from this preprint?
iSupport-Malaysia appears culturally appropriate and usable enough to refine for a pilot trial. The strongest remaining uncertainty is whether caregivers will keep using it and whether use improves burden, distress, or care confidence.
References
- Development and Evaluation of iSupport-Malaysia: A Multimedia Web-Based Psychoeducational Intervention for Dementia Caregivers. Loh et al. doi:10.64898/2026.04.14.26350743
- Efficacy of a Telephone-Intervention on Caregiving Burden and Mental Health among Family Caregivers of Persons with Dementia in Malaysia: A Randomized Controlled Trial. Ahmad et al. doi:10.3390/ijerph21101354
- Feasibility and preliminary effectiveness of an online training and support program for caregivers of people with dementia in India: a randomized controlled trial. Baruah et al. doi:10.1002/gps.5502
- User feedback and usability testing of an online training and support program for dementia carers. Teles et al. doi:10.1016/j.invent.2021.100412
- Usability and acceptability of internet-based interventions for family carers of people living with dementia: systematic review. Ottaviani et al. doi:10.1080/13607863.2021.1975095
- Remotely delivered information, training and support for informal caregivers of people with dementia. Gonzalez-Fraile et al. doi:10.1002/14651858.CD006440.pub3