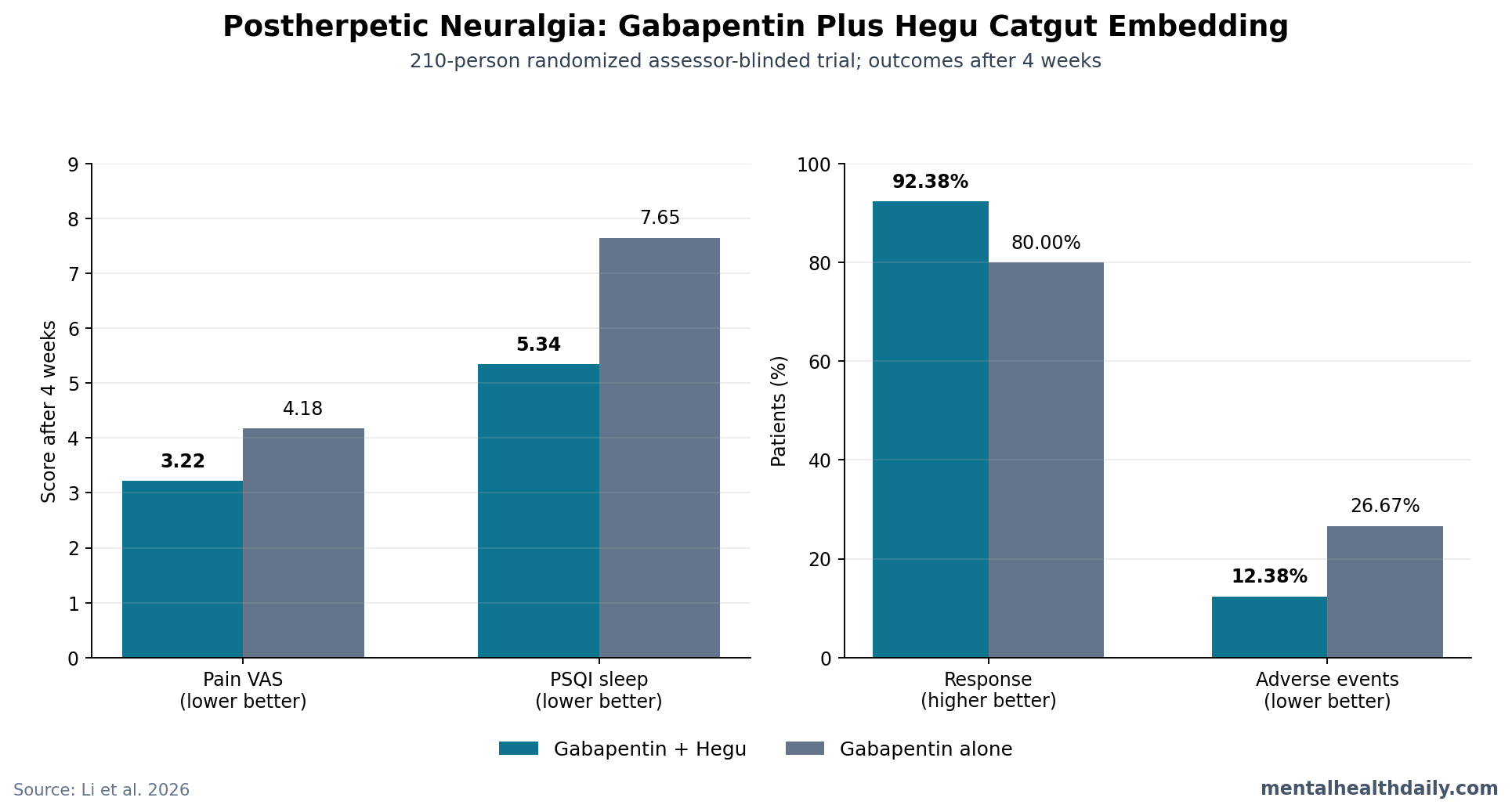
A 210-person randomized assessor-blinded trial found that adding weekly Hegu-point catgut embedding to gabapentin improved 4-week postherpetic-neuralgia response from 80.00% to 92.38%; compared with gabapentin alone, the add-on arm also ended with lower sleep-problem scores and fewer adverse events.[1] This 2026 trial supports an add-on signal that still needs sham-controlled confirmation because follow-up lasted only 4 weeks.
Research Highlights
- Response improved by 12.38 percentage points: 92.38% of patients receiving gabapentin plus Hegu catgut embedding met the trial’s response definition after 4 weeks vs. 80.00% with gabapentin alone.
- Pain scores ended lower: visual analogue scale pain scores fell to 3.22 ± 0.98 with the add-on vs. 4.18 ± 1.05 with gabapentin alone, a between-group difference reported at P < 0.001.
- Sleep moved with pain: Pittsburgh Sleep Quality Index sleep-problem scores ended at 5.34 ± 1.63 with combination therapy vs. 7.65 ± 1.90 with gabapentin alone.
- Adverse events were lower, not higher: dizziness, somnolence, ataxia, and local swelling/pain totaled 12.38% in the add-on arm vs. 26.67% in the gabapentin-only arm.
- Mechanism stayed indirect: serum substance P, IL-6, and TNF-α fell more, while β-endorphin rose more, but peripheral blood markers cannot prove central nervous system pain-circuit changes.
Postherpetic neuralgia is persistent nerve pain after shingles, usually felt as burning, stabbing, electric, or touch-evoked pain after the rash has healed. Chronic shingles-related nerve pain often disrupts sleep, mood, movement, and daily function, which is why a trial that measures both pain and Pittsburgh Sleep Quality Index (PSQI; a 0-21 sleep-quality score where higher is worse) is more useful than a pain-only trial.
Gabapentin is a gabapentinoid drug that binds the α2δ subunit of voltage-gated calcium channels, reducing release of excitatory pain-signaling chemicals such as glutamate and substance P. It is a standard neuropathic-pain option, but the practical ceiling is familiar: dizziness, somnolence, gait problems, dose limits, and incomplete pain relief often decide whether a patient can stay on an effective dose.[6]
Hegu Catgut Embedding Added Benefit Over Gabapentin Alone
Li et al. randomized 210 adults with postherpetic neuralgia to gabapentin alone or gabapentin plus weekly bilateral Hegu-point catgut embedding for 4 weeks.[1] Hegu, also called LI4, is an acupoint between the 1st and 2nd metacarpal bones of the hand. Catgut embedding means placing a short absorbable suture into the acupoint so the site receives prolonged mechanical stimulation instead of the brief stimulation used in ordinary needling.
Both groups received the same basic care and gabapentin schedule. Gabapentin started at 0.3 g at bedtime on day 1, increased to 0.3 g twice daily on day 2, then 0.3 g 3 times daily on day 3, with weekly titration up to 1.8 g/day depending on pain relief and tolerability. The add-on group received Hegu embedding once per week for 4 weeks.
Trial snapshot:
- Sample: 105 patients per group, age 40-70 years.
- Entry threshold: healed shingles lesions, neuropathic pain for at least 3 months, and VAS pain score at least 4.
- Design: randomized and assessor-blinded, but participants and treating clinicians were not blinded.
- Main endpoints: pain intensity, sleep quality, response category, serum biomarkers, and adverse events after 4 weeks.
The response definition was clinically concrete. “Markedly effective” meant at least 75% VAS reduction or near disappearance of pain. “Effective” meant 50-74% VAS reduction. Anything below 50%, no change, or worse pain counted as ineffective.
By that standard, 97 of 105 patients in the add-on group responded vs. 84 of 105 in the gabapentin-only group. Marked response was also more common with the add-on: 64.76% vs. 35.24%. That larger marked-response gap suggests the add-on shifted many patients into a stronger pain-relief category instead of only creating a small number of borderline responders.
Pain and Sleep Both Favored the Add-On Arm
Baseline pain and sleep scores were similar. After 4 weeks, both groups improved, but the combination group ended with lower pain and better sleep.
Pain: VAS scores ended at 3.22 ± 0.98 with combination therapy vs. 4.18 ± 1.05 with gabapentin alone. On a 0-10 pain scale, that is nearly a 1-point between-group difference after only 4 weeks, with P < 0.001.
Sleep: PSQI scores ended at 5.34 ± 1.63 in the add-on group vs. 7.65 ± 1.90 in the gabapentin-only group. Because smaller PSQI values mean fewer sleep problems, the direction is straightforward: sleep improved more when Hegu embedding was added.
The sleep result is not a decorative secondary outcome. In postherpetic neuralgia, pain and sleep reinforce each other: worse night pain reduces sleep, and poor sleep can increase next-day pain sensitivity. A pain intervention that improves PSQI while lowering VAS has a more plausible patient-level signal than one that shifts pain ratings without changing sleep.
Lower Adverse Events Make the Result More Interesting
The add-on arm had fewer reported adverse events: 13 of 105 patients (12.38%) vs. 28 of 105 patients (26.67%) in the gabapentin-only arm. Dizziness occurred in 4.76% vs. 11.43%, somnolence in 2.86% vs. 8.57%, and ataxia in 0.95% vs. 5.71%. Local swelling or pain at the embedding site was more common with the add-on, as expected for a needling procedure: 3.81% vs. 0.95%.
This pattern is clinically unusual for an add-on intervention. More treatments often mean more side effects.
Here, the adverse-event rate went down, likely because the combination group could tolerate less gabapentin escalation or needed less dose pressure, although the trial did not provide a detailed dose-by-dose adverse-event model. The paper stated that the mean required gabapentin dose was lower in the combination group, but the published table did not give the exact dose values.
Practical interpretation: the tolerability signal is promising but incomplete. A future trial should report final gabapentin dose, rescue-medication use, withdrawals, falls, sedation severity, and daily functioning so the lower adverse-event rate can be tied to actual dose-sparing rather than reporting noise.
Serum Biomarkers Supported Analgesia but Did Not Prove Brain Mechanism
Li et al. measured 4 serum markers before and after treatment: substance P, β-endorphin, interleukin-6 (IL-6), and tumor necrosis factor-α (TNF-α). Substance P is a pain-signaling neuropeptide involved in nociceptive transmission. β-endorphin is an endogenous opioid peptide produced by the body. IL-6 and TNF-α are inflammatory cytokines that can participate in nerve sensitization and sickness-behavior pathways.
After 4 weeks, the add-on group had lower substance P (46.69 vs. 52.23 pg/mL), lower IL-6 (7.35 vs. 12.58 pg/mL), lower TNF-α (5.83 vs. 7.02 pg/mL), and higher β-endorphin (68.34 vs. 57.26 ng/L) than the gabapentin-only group. All 4 between-group comparisons were statistically significant.
Biomarker interpretation: those shifts line up with the clinical pattern: less pain signaling, less inflammatory tone, and more endogenous opioid activity.
Peripheral serum markers do not show what happened inside spinal dorsal horn circuits, descending pain-control pathways, glia, or cortical pain networks. They show a systemic biological correlate of improvement, not a direct brain or spinal-cord mechanism.
Acupuncture Evidence for Postherpetic Neuralgia Is Positive but Fragile
The Li trial fits a broader literature in which acupuncture-related therapies often look helpful for postherpetic neuralgia, but the evidence base remains methodologically uneven. Pei et al. reviewed randomized trials and found pain reduction favoring acupuncture, including electroacupuncture, fire needle, and bloodletting/cupping subgroups, while still calling for better trials.[3]
Zhou et al. analyzed 16 studies with 1,140 patients and reported benefits for acupuncture and moxibustion combined with cupping compared with Western medicine comparators.[2] Yang et al. later ran a Bayesian network meta-analysis of 29 randomized trials involving 1,973 patients; pricking/cupping plus antiepileptics and electroacupuncture plus antiepileptics ranked highly, but the authors warned that risk of bias and uneven study quality limited certainty.[4]
The 2026 Li trial improves on some older work by using randomization, equal group size, assessor blinding, standardized gabapentin background therapy, and biomarker measurement. It does not solve the core expectancy problem. Without sham catgut embedding, patients knew whether they received a hands-on weekly procedure plus a drug or a drug alone. Pain and sleep are especially vulnerable to expectancy, contact time, and attention effects.
What the Trial Can and Cannot Support
The short-term result supports a specific claim: in this single-center 4-week trial, gabapentin plus weekly Hegu LI4 catgut embedding outperformed gabapentin alone on pain, sleep, response, adverse events, and serum biomarkers. That is enough to justify a larger replication trial.
It cannot support several stronger claims:
- Not durable remission: 4 weeks is too short for a chronic neuropathic-pain syndrome that can persist for months or years.
- Not specific acupoint proof: a single Hegu protocol cannot show that LI4 is uniquely necessary, that catgut embedding beats ordinary acupuncture, or that multi-acupoint protocols would be worse or better.
- Not placebo-resistant evidence: assessor blinding helps outcome rating, but participant and provider expectations remain live confounders.
- Not central mechanism proof: serum biomarker shifts are compatible with a neuroimmune pain model, but they do not directly measure central sensitization.
A stronger next study needs a sham-embedding comparator, longer follow-up, final gabapentin dose reporting, functional outcomes, and a prespecified sleep endpoint. If the 92.38% vs. 80.00% response gap survives that design, the add-on becomes more than an interesting short-term signal.
Questions About Gabapentin Plus Hegu Catgut Embedding
Should postherpetic neuralgia patients add Hegu catgut embedding to gabapentin?
The 2026 trial supports cautious interest, not routine adoption. Patients already using gabapentin who have access to a qualified practitioner may reasonably see this as a discussion point, but the missing sham control and short follow-up keep the evidence below a firm recommendation.
Was the sleep improvement just a side effect of pain relief?
Possibly, and that is not a weakness. In postherpetic neuralgia, less nighttime pain can directly improve sleep. The trial did not prove an independent sleep mechanism; it showed that the add-on group ended with both lower pain and better PSQI scores after 4 weeks.
Does a lower adverse-event rate mean catgut embedding protects against gabapentin side effects?
No. The lower rate is encouraging, but the trial did not isolate a protective mechanism. The more plausible interpretation is dose-sparing or symptom improvement that reduced the need for higher gabapentin exposure, but that needs explicit dose and adverse-event modeling.
How should the biomarker findings be read?
They support biological plausibility. Lower substance P, IL-6, and TNF-α plus higher β-endorphin fit a pain-and-inflammation pathway, but blood markers cannot prove that Hegu embedding directly changed spinal or brain pain circuits.
References
- Li LP, Song ZZ, Zheng Y, et al. Pharmacodynamic basis of gabapentin combined with Hegu-point catgut embedding for post-herpetic neuralgia. Pakistan Journal of Pharmaceutical Sciences. 2026;39(6):1611-1617. doi:10.36721/PJPS.2026.39.5.152.1
- Zhou Q, Wei S, Zhu H, et al. Acupuncture and moxibustion combined with cupping for the treatment of post-herpetic neuralgia: A meta-analysis. Medicine. 2021;100(31):e26785. doi:10.1097/MD.0000000000026785
- Pei W, Zeng J, Lu L, Lin G, Ruan J. Is acupuncture an effective postherpetic neuralgia treatment? A systematic review and meta-analysis. Journal of Pain Research. 2019;12:2155-2165. doi:10.2147/JPR.S199950
- Cui Y, Zhou X, Li Q, et al. Efficacy of different acupuncture therapies on postherpetic neuralgia: A Bayesian network meta-analysis. Frontiers in Neuroscience. 2022;16:1056102. doi:10.3389/fnins.2022.1056102
- Wang L, Qiu L, Zheng X, et al. Effectiveness of electroacupuncture at Jiaji acupoints (EX-B2), plus moxibustion and intermediate on postherpetic neuralgia: A randomized controlled trial. Journal of Traditional Chinese Medicine. 2020;40(1):121-127. PubMed:32227773
- Shi Y, Song C. Effectiveness and safety of gabapentin versus pregabalin in the treatment of postherpetic neuralgia: A retrospective cohort study. British Journal of Hospital Medicine. 2024;85(12):1-11. doi:10.12968/hmed.2024.0485
- Meaadi J, Obara I, Eldabe S, Nazar H. The safety and efficacy of gabapentinoids in the management of neuropathic pain: A systematic review with meta-analysis of randomized controlled trials. International Journal of Clinical Pharmacy. 2023;45(3):556-565. doi:10.1007/s11096-022-01528-y