A 2026 cross-sectional study of 79 adults receiving hemodialysis found dialysis headache in 40 patients (50.6%), and a prior history of recurrent headaches was the strongest adjusted signal: OR = 4.08 (95% CI 1.42-11.75; p = 0.009).
Research Highlights
- Dialysis headache was common: 40 of 79 hemodialysis patients met ICHD-3 criteria, putting frequency at 50.6% in this single-center Saudi sample.
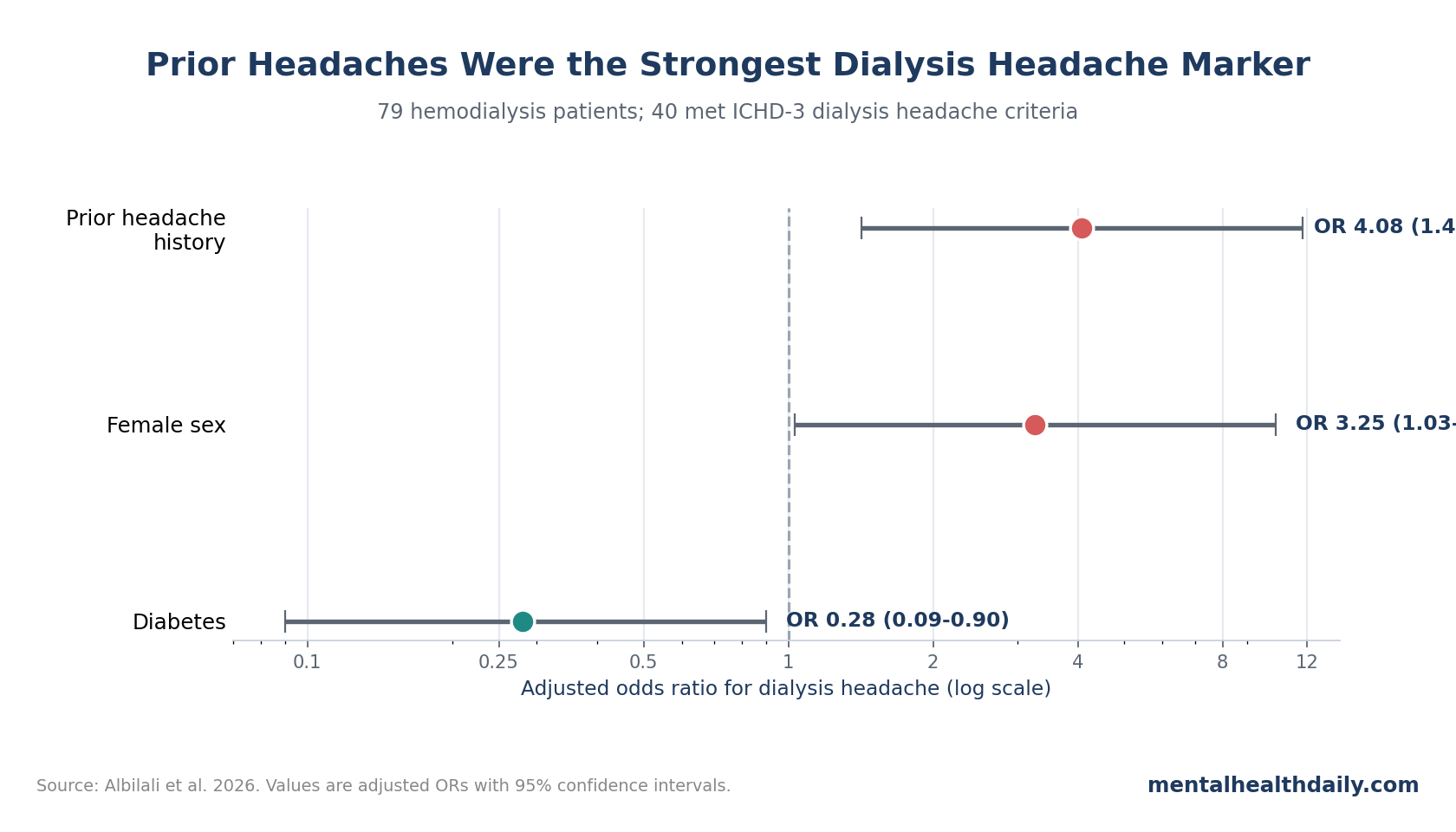
- Prior headaches carried the largest adjusted signal: recurrent headache history before dialysis was reported by 65.0% of patients with dialysis headache vs. 33.3% without it, and remained associated after adjustment (OR = 4.08; 95% CI 1.42-11.75).
- Female sex also raised odds: women had higher adjusted odds of dialysis headache than men (OR = 3.25; 95% CI 1.03-10.33), although the confidence interval was wide.
- Blood-pressure physiology stayed relevant: during-dialysis diastolic pressure averaged 61.1 mmHg in the headache group vs. 68.7 mmHg in the non-headache group (p = 0.028).
- The diabetes signal needs caution: diabetes showed an inverse adjusted association (OR = 0.28; 95% CI 0.09-0.90), but the study design cannot show protection.
Dialysis headache is a secondary headache disorder: the headache starts or worsens during hemodialysis and then improves after the session rather than behaving like a stand-alone migraine or tension-type headache. The International Classification of Headache Disorders requires repeated attacks linked in time to dialysis and spontaneous resolution after the treatment window.
The 2026 study points to a susceptibility-plus-trigger pattern: prior recurrent headaches, sex-linked vulnerability, intradialytic blood-pressure shifts, and neurovascular signaling can all point in the same direction.
50.6% of Hemodialysis Patients Met Dialysis Headache Criteria
Albilali et al. interviewed adults with end-stage renal disease who had been receiving regular hemodialysis for at least 6 months at King Khalid University Hospital. Of 83 people interviewed, 79 had complete usable data.
Headache status was not counted from vague discomfort alone. Patients were classified as having dialysis headache if they reported at least 3 headache episodes that developed or worsened during hemodialysis and resolved within 72 hours after the session, matching ICHD-3 criteria.
Sample: 40 patients with dialysis headache and 39 without dialysis headache.
Dialysis schedule: all patients were prescribed online hemodiafiltration for 4 hours per session, 3 times per week.
Clinical pattern: most dialysis headaches were moderate rather than severe. In the 40 headache cases, 21 patients (52.5%) rated pain as moderate, 14 (35.0%) as mild, and 5 (12.5%) as severe.
Timing and location were also fairly consistent. Headache began during the second half of dialysis in 23 of 40 cases (57.5%), lasted 5.2 ± 5.4 hours on average, and resolved within 72 hours in all cases. Frontotemporal pain was the most common location (35.0%), followed by temporal pain (25.0%), occipital pain (22.5%), and generalized headache (17.5%).
Prior Recurrent Headaches Were Tied to 4.08x Higher Odds
Prior headache history separated the groups more clearly than most ordinary demographic or dialysis variables. Among patients with dialysis headache, 26 of 40 (65.0%) reported headache attacks before starting hemodialysis. Among patients without dialysis headache, 13 of 39 (33.3%) reported prior attacks (p = 0.005).
Adjusted regression kept that signal. After accounting for age, sex, hypertension, diabetes, smoking, and caffeine intake, prior recurrent headache history was associated with OR = 4.08 (95% CI 1.42-11.75; p = 0.009).
How to read the odds ratio: the model estimated roughly 4x higher odds of dialysis headache among patients with prior recurrent headaches than among patients without prior recurrent headaches. It does not prove that old headaches caused the dialysis-linked attacks, because the study was cross-sectional and prior headache history was self-reported.
Still, the finding fits older dialysis headache work. Antoniazzi et al. prospectively studied headache and hemodialysis and reported that many dialysis headache cases had headache before hemodialysis, with migraine without aura and episodic tension-type headache both represented. Melo et al. later described dialysis headache clinically but did not find the same clear primary-headache link, which makes the 2026 result useful but not settled.
Female Sex and Lower Diastolic Pressure Point to Susceptibility Plus Trigger
Female sex also remained associated with dialysis headache in the adjusted model. Women had OR = 3.25 (95% CI 1.03-10.33; p = 0.045) compared with men. In raw counts, women made up 20 of 40 headache cases (50.0%) but only 9 of 39 non-headache cases (23.1%).
Blood pressure added a different kind of signal. Pre-dialysis systolic and diastolic pressure did not differ significantly between groups, and post-dialysis systolic pressure did not separate them either. The clearest pressure difference appeared during dialysis: diastolic blood pressure averaged 61.1 ± 14.7 mmHg in patients with dialysis headache vs. 68.7 ± 14.7 mmHg in those without it (p = 0.028).
Mechanistic interpretation: lower intradialytic diastolic pressure could reflect hemodynamic stress during treatment. If cerebral blood-flow regulation is already vulnerable, a dialysis-session pressure drop may help trigger head pain, especially in people with a headache-prone trigeminovascular system.
Clinical limitation: one pressure comparison cannot identify the triggering mechanism. A stronger design would track blood-pressure variability, ultrafiltration volume, sodium shifts, hydration status, headache timing, and cerebral autoregulation during the same session.
CGRP, Substance P, and Dialysis Physiology Make the Link Plausible
CGRP (calcitonin gene-related peptide) is a neuropeptide involved in migraine biology, pain signaling, blood-vessel dilation, and neurogenic inflammation. Substance P is another pain-related neuropeptide that can amplify nociceptive signaling.
Dialysis headache is more specific than head pain during a medical appointment. Alessandri et al. measured plasma CGRP and substance P in patients with dialysis headache and found changes around hemodialysis, supporting a neurovascular pain mechanism. Migraine and tension-type headache biology also involve altered sensory processing, which makes prior headache history biologically credible as a susceptibility marker.
Hemodialysis can then supply the trigger side of the equation. Adjacent work has studied blood sodium, blood-pressure variability, hydration status, nitric oxide signaling, caffeine withdrawal, and dialysis modality. Xiong et al. linked hemodialysis-related headache with intradialysis sodium and physiologic variation, while Aoun et al. tested caffeinated vs. decaffeinated coffee during dialysis and did not show a strong caffeine-withdrawal explanation.
- Susceptibility layer: prior migraine-like or tension-type headache biology may lower the threshold for dialysis-linked pain.
- Session trigger layer: fluid shifts, osmolality changes, blood-pressure variation, and vascular reactivity may push susceptible patients into headache during treatment.
- Clinical phenotype layer: moderate frontotemporal pain during the latter half of dialysis looks repeatable enough to ask about directly.
Diabetes Looked Inversely Associated, But Protection Is Not Proven
Diabetes was more common in the non-headache group than in the dialysis headache group: 23 of 39 patients without dialysis headache (59.0%) had diabetes vs. 13 of 40 patients with dialysis headache (32.5%; p = 0.018). The adjusted model estimated OR = 0.28 (95% CI 0.09-0.90; p = 0.033).
This is the easiest result to overread. The finding may reflect residual confounding, differences in vascular reactivity, diabetic neuropathy, pain perception, age and comorbidity patterns, or the small number of events per predictor in the model. Large epidemiologic data have sometimes linked diabetes with lower migraine prevalence, but causal protection against dialysis headache remains unproven.
Evidence-strength note: this was an exploratory cross-sectional study. It can identify associations worth testing prospectively, but it cannot establish causal risk factors, build a stable prediction model, or prove that changing intradialytic blood pressure will prevent headache.
How Dialysis Units Can Use the Finding Now
The low-risk clinical move is direct screening. Hemodialysis patients can be asked whether headaches start or worsen during the session, whether attacks resolve after treatment, and whether they had recurrent headaches before dialysis began.
For patients with repeated dialysis-linked attacks, documentation should separate 4 questions:
- Timing: whether pain begins early, during the second half of dialysis, after dialysis, or outside the dialysis window.
- Phenotype: location, intensity, duration, nausea, photophobia, phonophobia, and whether the headache resembles the patient’s older headache pattern.
- Dialysis physiology: intradialytic blood pressure, ultrafiltration, sodium shifts, hydration status, and other session changes.
- Safety screen: new neurologic deficits, severe sudden-onset headache, infection signs, uncontrolled hypertension, or other red flags that should not be filed under routine dialysis headache.
That approach stays calibrated. It treats prior headache history as a risk marker, not as a dismissal. It also keeps dialysis-session physiology visible instead of assuming every attack is just a migraine recurring in a medically complicated setting.
Questions About Dialysis Headache
Is dialysis headache the same thing as migraine?
No. Dialysis headache is defined by its timing around hemodialysis. Some patients may have migraine biology or a prior migraine-like history, but the dialysis-linked attack is classified by the treatment relationship.
Should prior recurrent headaches be documented before dialysis starts?
Yes. The 2026 study found prior headache history was the strongest adjusted marker of dialysis headache. Recording baseline headache history gives clinicians a cleaner way to interpret new or worsening headaches after dialysis begins.
Does lower blood pressure during dialysis cause the headache?
The study cannot prove causality. It found lower during-dialysis diastolic pressure in the headache group, which makes hemodynamic triggering plausible, but prospective session-level monitoring is needed.
Does diabetes reduce dialysis headache risk?
Possibly, but the safer interpretation is uncertainty. Diabetes showed an inverse association in this small cross-sectional model, and the mechanism could involve confounding or altered pain perception rather than true protection.
References
- Albilali AS, Bahammam RAS, Albadrani WF, Alharbi MK, Alfaadhel TA, Ashina S, et al. Dialysis headache in hemodialysis patients: is a history of recurrent headaches prior to hemodialysis a risk factor? Journal of Pain Research. 2026;19:594581. doi:10.2147/JPR.S594581
- Antoniazzi AL, Bigal ME, Bordini CA, Tepper SJ, Speciali JG. Headache and hemodialysis: a prospective study. Headache. 2003;43(2):99-102. doi:10.1046/j.1526-4610.2003.03025.x
- Melo ES, Pedrosa RP, Aguiar FC, Valente LM, Rocha-Filho PAS. Dialysis headache: characteristics, impact and cerebrovascular evaluation. Arquivos de Neuro-Psiquiatria. 2022;80(2):129-136. doi:10.1590/0004-282x-anp-2021-0133
- Alessandri M, Massanti L, Geppetti P, Bellucci G, Cipriani M, Fanciullacci M. Plasma changes of calcitonin gene-related peptide and substance P in patients with dialysis headache. Cephalalgia. 2006;26(11):1287-1293. doi:10.1111/j.1468-2982.2006.01217.x
- Xiong Y, You N, Liao R, et al. Association of intradialysis blood sodium level, blood pressure variability, and hydration status with hemodialysis-related headache: a prospective cohort study. The Journal of Headache and Pain. 2023;24:166. doi:10.1186/s10194-023-01701-2
- Aoun MH, Hilal N, Beaini C, et al. Effects of caffeinated and decaffeinated coffee on hemodialysis-related headache (CoffeeHD): a randomized multicenter clinical trial. Journal of Renal Nutrition. 2021;31(6):648-660. doi:10.1053/j.jrn.2021.01.025
- Headache Classification Committee of the International Headache Society. The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1-211. doi:10.1177/0333102417738202