
A 2026 randomized trial of 74 psychiatric inpatients found that 5 consecutive MIDI-assisted group music therapy sessions reduced DASS-21 stress more than 1 session during the same hospital week, but the frequency advantage did not extend to anxiety, depression, life satisfaction, or immediate session-impact ratings.
Research Highlights
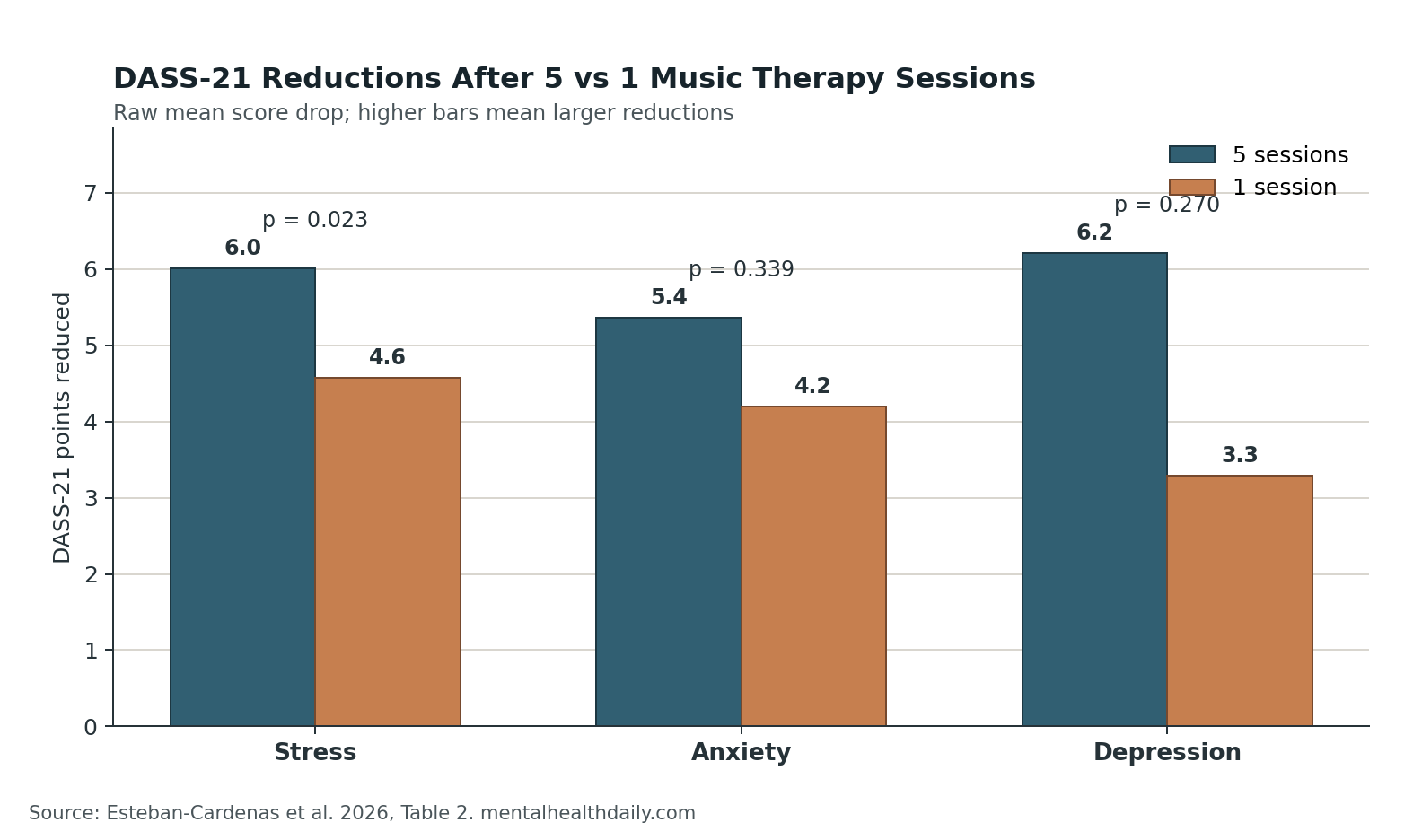
- Stress separated by frequency: 5 sessions produced a larger DASS-21 stress reduction than 1 session, with a significant group-by-time interaction (p = 0.023).
- Anxiety did not separate: anxiety fell in both arms, but the 5-session vs. 1-session difference was not statistically confirmed (p = 0.339).
- Depression stayed nonspecific: depression scores improved over the week, but the frequency comparison missed significance (p = 0.270).
- Session ratings were flat: CISMA ratings for current well-being, relaxation, and cheerfulness did not differ between the 5-session and 1-session groups (p = 0.18, 0.79, and 0.35).
- Evidence strength is limited: 91 patients were randomized, 74 completed post-intervention assessment, and the stress result was exploratory because multiple DASS-21 domains were tested.
Music therapy means using structured musical activity for clinical goals. In this trial, psychiatric inpatients used a Playtron MIDI controller connected to conductive objects such as fruit, water, and plants, alongside traditional instruments, group synchronization, breathing, and progressive muscle relaxation.
The best reading is calibrated: higher session frequency may help acute stress regulation inside a short psychiatric admission, but the study does not show a broad dose-response effect across mood, anxiety, life satisfaction, or subjective emotional response.
5 Sessions Beat 1 Session Only for DASS-21 Stress
Esteban-Cardenas et al. randomized 91 adult inpatients at a psychiatric hospital in Bogota, Colombia, to 5 music therapy sessions in 1 week or 1 session during the same inpatient week. The per-protocol analysis included 37 patients in each arm after discharge and follow-up losses.
DASS-21 is the Depression Anxiety Stress Scale, a self-report measure with separate depression, anxiety, and stress subscales. Scores are usually doubled to align with the longer DASS-42 format, so a lower score after treatment means fewer symptoms in that domain.
Raw mean stress scores moved from 12.5 to 6.49 in the 5-session arm and from 11.6 to 7.03 in the 1-session arm. That is a 6.01-point raw mean reduction with 5 sessions vs. 4.57 points with 1 session, and the mixed model found a significant group-by-time interaction for stress (p = 0.023).
The same pattern did not hold cleanly for anxiety or depression. Anxiety scores moved from 11.6 to 6.24 with 5 sessions and from 11.5 to 7.30 with 1 session, but the frequency comparison was not significant (p = 0.339). Depression scores moved from 12.7 to 6.49 with 5 sessions and from 12.4 to 9.11 with 1 session, but the between-frequency test also missed significance (p = 0.270).
The Trial Tested Intensity During a Brief Psychiatric Admission
The clinical question was unusually practical: if inpatient stays are short, should music therapy be concentrated into several sessions or offered once as a low-intensity adjunct?
The 5-session group received 30-minute sessions on 5 consecutive days. The 1-session group received a single 30-minute session during the same week, then could attend additional sessions after outcome measurement if they were still hospitalized. Both arms continued standard psychiatric care, including medication management.
Intervention structure: sessions used a 4-phase format: welcome and warm-up, group synchronization with breathing and progressive muscle relaxation, creative ensemble work with MIDI-connected conductive objects and instruments, and a closing phase. The intervention was designed to support emotional regulation, attention, group cohesion, and sensory novelty.
Patient mix: the analyzed sample was mostly female and mostly hospitalized for depressive or bipolar disorders. In the 5-session arm, 62.2% had depressive disorders and 18.9% had bipolar disorder; in the 1-session arm, 59.5% had depressive disorders and 24.3% had bipolar disorder.
Attrition: 106 patients were screened, 91 enrolled, and 74 completed the post-intervention DASS-21 assessment. Because the final analysis excluded patients who did not complete the intervention or follow-up assessment, the result is best treated as per-protocol evidence rather than a full intention-to-treat estimate.
Why the Stress Result Is Plausible but Narrow
Music-based interventions are especially plausible for acute arousal and stress because rhythm, breathing, attention, interpersonal synchrony, and relaxation practice can all shift the body out of a threat-heavy state. That makes the stress-specific result more biologically coherent than a broad claim that 5 sessions outperform 1 session for psychiatric symptoms overall.
Two features of this protocol make the stress signal believable:
- Repeated regulation practice: 5 sessions gave patients repeated exposure to breathing, muscle relaxation, group rhythm, and structured sensory engagement over consecutive days.
- Acute-state target: DASS-21 stress is closer to tension, agitation, and overarousal than to slower-moving constructs such as life satisfaction or diagnostic depression.
But the same specificity limits the claim. The study did not show that a higher dose of music therapy changed the broader inpatient course, reduced medication needs, shortened hospitalization, or improved objective clinical outcomes. It showed a short-term self-reported stress difference inside a multicomponent inpatient treatment week.
Adjacent Evidence Supports Music Therapy but Not a Clean Dose Rule
Inpatient setting: Carr et al. reviewed music therapy practice and outcomes in acute adult psychiatric inpatient units and found a field built around active group expression, improvisation, and verbal reflection, but also uneven methods and small samples. That review supports the setting, not a precise rule that 5 sessions are clinically superior to 1 session.
Severe mental illness evidence: Cassola et al. reviewed music therapy and musical interventions for moderate and severe mental disorders in 2024. The evidence base was compatible with symptom and engagement benefits, but the studies varied too much in population, intervention type, session number, control condition, and outcome choice to convert into a simple frequency prescription.
Depression trials: Tang et al. synthesized randomized music-therapy trials for depression and found antidepressant effects across broader clinical settings. That helps explain why both groups in the inpatient trial improved on depression scores, but it does not prove that more sessions inside 1 hospital week should beat fewer sessions for depression.
Ma et al. reported efficacy and acceptability evidence for music therapy in post-traumatic stress disorder (PTSD), a condition where arousal, threat memory, and avoidance can dominate daily function. Their review also raised the possibility that treatment duration matters, but PTSD trials cannot be directly mapped onto mixed-diagnosis inpatient psychiatry.
Together, the adjacent literature points in the same direction as the 2026 inpatient RCT: music therapy is a plausible adjunct for distress and engagement, but the dose-response question remains underdefined. The strongest immediate use case is stress regulation, not diagnosis-specific remission.
Life Satisfaction and CISMA Ratings Did Not Confirm a Broader Effect
SWLS refers here to a single life-satisfaction rating, not the full multi-item Satisfaction With Life Scale. The 5-session group improved from 54.7 to 66.3, and the 1-session group improved from 60.4 to 71.0, but the frequency comparison was not significant (p = 0.875).
CISMA is a music-therapy session-impact questionnaire. The study used 3 selected 0-to-10 visual analog items: “How do you feel now?”, “Right now, I feel relaxed,” and “Right now, I feel cheerful.”
Those immediate ratings did not support a clear frequency advantage. The 5-session group scored 8.08 vs. 7.38 on feeling now (p = 0.18), 7.31 vs. 7.46 on relaxation (p = 0.79), and 7.69 vs. 7.16 on cheerfulness (p = 0.35). The researchers also noted that the selected CISMA items may not have been sensitive enough to detect more specific emotional changes.
This is the main guardrail against overreading the trial. If 5 sessions had produced a robust general therapeutic advantage, the signal should have appeared across more than 1 self-report stress subscale. Instead, the measurable advantage stayed narrow.
Method Limits Make the Result Exploratory
The trial has enough structure to be useful and enough limitations to keep the claim modest.
- No usual-care-only arm: both groups received music therapy and standard psychiatric care, so within-group improvement cannot be credited to music therapy alone.
- Per-protocol analysis: 17 of 91 randomized participants did not enter the final post-intervention DASS-21 analysis, which can bias results if completion relates to clinical response or discharge timing.
- No participant blinding: patients knew whether they received 5 sessions or 1 session, and expectations may have influenced self-reported outcomes.
- Retrospective trial registration: public prospective confirmation of the planned protocol was unavailable, even though an ethics-approved written protocol existed before data collection.
- Multiple comparisons: stress, anxiety, depression, life satisfaction, and CISMA items were all tested. The stress interaction reached p = 0.023, but a simple Bonferroni-style correction across the DASS-21 domains would make that result less secure.
The evidence-strength note is therefore straightforward: this randomized trial can support a preliminary stress-specific signal for intensive music therapy during brief psychiatric hospitalization. It cannot establish a general inpatient music-therapy dose rule, prove antidepressant efficacy, or show that MIDI-assisted sessions improve hard clinical outcomes.
Questions About Music Therapy Frequency in Inpatient Psychiatry
Should psychiatric units treat 5 sessions as better than 1 session?
For acute stress, 5 sessions have the better signal in this trial. For anxiety, depression, life satisfaction, and immediate session ratings, the study did not statistically confirm a frequency advantage.
Was this really about MIDI technology?
Only partly. The MIDI controller made the intervention novel and multisensory, but the protocol also included group rhythm, traditional instruments, breathing, progressive muscle relaxation, and closing rituals. The trial cannot isolate the technology from the broader music-therapy structure.
Does this prove music therapy treats depression?
No. Depression scores improved in both arms, and broader meta-analyses support music therapy as a possible depression adjunct, but this trial did not show that 5 inpatient sessions reduced depression more than 1 session.
What outcome should future inpatient studies measure?
Stress should remain a core outcome, but future trials also need objective or clinician-rated endpoints: length of stay, agitation episodes, medication changes, sleep, group attendance, restraint use, readmission, and diagnosis-specific symptom scales.
Practical read: music therapy is a reasonable low-risk adjunct in psychiatric inpatient units when delivered by trained staff with safety monitoring. If the target is short-term stress regulation, several closely spaced sessions may be more useful than a single exposure.
The honest limit is equally important: current evidence does not justify presenting high-frequency music therapy as a stand-alone treatment for depression or anxiety during hospitalization. It is best understood as a structured engagement and regulation tool layered onto standard psychiatric care.
References
- Esteban-Cardenas M, Gomez-Puentes A, Torres-Delgado C, Hidalgo-Valbuena A, Ferro E. High-frequency vs. low-frequency MIDI-assisted group music therapy in psychiatric inpatients: A randomized controlled trial. PLOS One. 2026;21(4):e0317950. https://doi.org/10.1371/journal.pone.0317950
- Carr C, Odell-Miller H, Priebe S. A systematic review of music therapy practice and outcomes with acute adult psychiatric in-patients. PLOS One. 2013;8(8):e70252. https://doi.org/10.1371/journal.pone.0070252
- Cassola EG, Santos LCD, de Castro Ferreira MS, Correa Barbosa G, Betini M, Domingos TS. Systematic review of music therapy and musical interventions for patients with moderate and severe mental disorders. Journal of Integrative and Complementary Medicine. 2024;30(9):819-831. https://doi.org/10.1089/jicm.2023.0419
- Tang Q, Huang Z, Zhou H, Ye P. Effects of music therapy on depression: A meta-analysis of randomized controlled trials. PLOS One. 2020;15(11):e0240862. https://doi.org/10.1371/journal.pone.0240862
- Ma Y-M, Yuan M-D, Zhong B-L. Efficacy and acceptability of music therapy for post-traumatic stress disorder: A systematic review and meta-analysis of randomized controlled trials. European Journal of Psychotraumatology. 2024;15(1):2342739. https://doi.org/10.1080/20008066.2024.2342739
- Grocke D, Bloch S, Castle D, Thompson G, Newton R, Stewart S, et al. Group music therapy for severe mental illness: a randomized embedded-experimental mixed methods study. Acta Psychiatrica Scandinavica. 2014;130(2):144-153. https://doi.org/10.1111/acps.12224
- Morgan K, Bartrop R, Telfer J, Tennant C. A controlled trial investigating the effect of music therapy during an acute psychotic episode. Acta Psychiatrica Scandinavica. 2011;124(5):363-371. https://pubmed.ncbi.nlm.nih.gov/21740403/
- Zhou K, Li X, Li J, Liu M, Dang S, Wang D, et al. A clinical randomized controlled trial of music therapy and progressive muscle relaxation training in female breast cancer patients after radical mastectomy. European Journal of Oncology Nursing. 2015;19(1):54-59. https://doi.org/10.1016/j.ejon.2014.07.010