
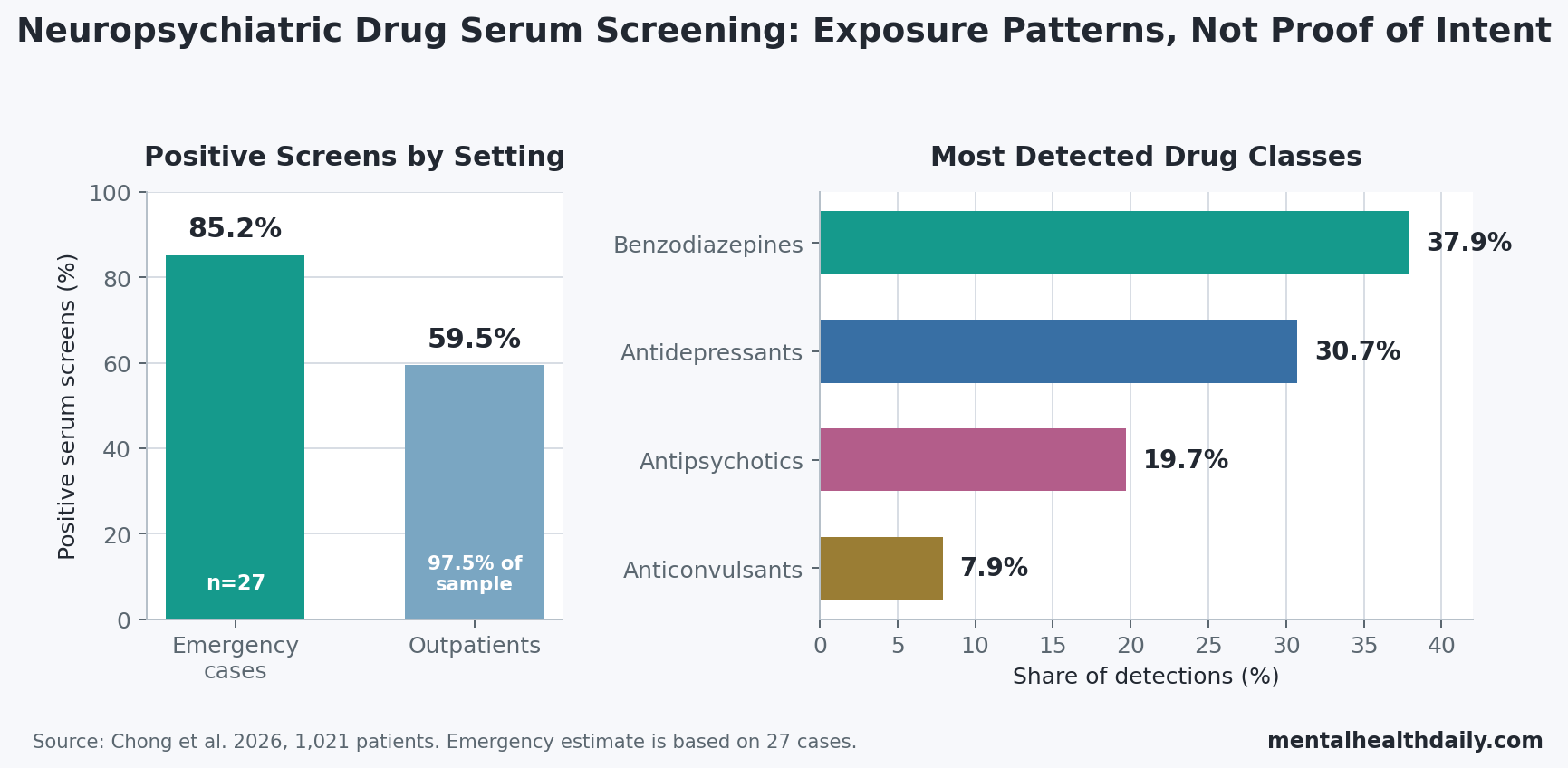
A 2026 clinical-lab study tested a 77-drug liquid chromatography-tandem mass spectrometry serum screen in 1,021 patients and found that benzodiazepines accounted for 37.9% of all detections, ahead of antidepressants and antipsychotics.1 Emergency-department cases were a small slice of the sample, but they were positive more often than outpatients: 85.2% vs. 59.5%.
Research Highlights
- Benzodiazepines dominated detections: across 1,021 patients, benzodiazepines made up 37.9% of positive detections, compared with 30.7% for antidepressants and 19.7% for antipsychotics.1
- Emergency screens were more often positive: 85.2% of emergency-department cases tested positive vs. 59.5% of outpatient cases, although the emergency sample included only 27 cases.1
- The panel was broad but fast: the method screened 77 drugs and metabolites from 20 uL serum, with sample preparation under 15 minutes per batch and a 15-minute chromatographic run.1
- Validation was strong but incomplete: 60 of 77 analytes had qualitative accuracy testing with 100% agreement across 138 of 138 checks; 17 analytes lacked suitable reference materials.1
- Exposure is not intent: a positive serum screen can support medication-history, adherence, or intoxication workups, but it does not by itself prove misuse, overdose intent, or exact toxicity level.1
Liquid chromatography-tandem mass spectrometry (LC-MS/MS) is a laboratory method that separates chemicals in a sample and then identifies them by mass and fragmentation pattern. In clinical toxicology, its advantage is specificity: it can distinguish many prescription drugs and metabolites that simpler immunoassays may miss or misclassify.
The useful clinical question is not whether a 77-drug panel sounds technically impressive. It is whether a serum test can answer a real-time medication question: which sedatives, antidepressants, antipsychotics, anticonvulsants, or hypnotics are currently present when history, prescribing records, symptoms, and patient recall do not line up.
77-Drug Serum Screening Used 20 uL and a 15-Minute Run
Chong et al. developed the assay for serum rather than urine. Serum drug screening captures a more current exposure window because the blood sample reflects drugs circulating near the time of testing; urine can remain positive after metabolites accumulate for several days, which is useful for some forensic questions but less direct for immediate clinical medication reconciliation.
The panel targeted 77 neuropsychiatric drugs and metabolites. It included benzodiazepines and related sedative-hypnotics, antidepressants, antipsychotics, anticonvulsants, barbiturates, and several metabolites that help identify the parent drug more reliably.
- Sample: 20 uL serum mixed with methanol containing internal standards.
- Preparation: simple protein precipitation and centrifugation, under 15 minutes per batch.
- Instrument run: 15 minutes per sample on LC-MS/MS.
- Identification rule: multiple reaction monitoring followed by product-ion spectrum confirmation and library matching.
That workflow is the point of the paper. The method was not trying to be the widest possible drug library. It was trying to make a clinically usable serum screen for common neuropsychiatric medications that appear in psychiatric, neurologic, sleep, and intoxication workups.
Benzodiazepines Were the Most Common Positive Drug Class
The clinical-application dataset included 1,045 serum drug-screening tests from 1,021 patients between March 2022 and March 2025. Only each patient’s first test was analyzed, which keeps repeat testing from inflating counts.
Psychiatry ordered most tests: 731 cases, or 71.6% of the sample. Neurology accounted for 263 cases, or 25.8%. Emergency medicine accounted for only 27 cases, or 2.6%, but those emergency cases had the highest positivity rate.
The detected-drug pattern was heavily tilted toward ordinary prescription neuropsychiatric medications:
- Benzodiazepines: 37.9% of detections.
- Antidepressants: 30.7% of detections.
- Antipsychotics: 19.7% of detections.
- Anticonvulsants: 7.9% of detections.
The most common analyte groups were clonazepam / 7-aminoclonazepam (159 detections; 10.2%), lorazepam (155; 10.0%), alprazolam / alpha-hydroxyalprazolam (136; 8.8%), aripiprazole (129), citalopram (128), quetiapine (103), and venlafaxine / norvenlafaxine (102). Those are not exotic toxicology findings. They are the drugs clinicians actually encounter when psychiatric medication histories become uncertain.
Emergency Cases Were Small but Clinically Revealing
Emergency-department testing is the part of the study most likely to be overread. The positivity rate was higher in emergency cases than in outpatients, but the denominator was only 27 emergency cases, so the estimate is directionally useful rather than stable enough for broad prevalence claims.
Within those 27 emergency cases, suspected drug intoxication accounted for 17 cases. Among suspected-intoxication cases, 14 patients had underlying psychiatric disorders, mostly depressive disorder or bipolar affective disorder, and all 14 tested positive.
Clinical interpretation: the screen helps when the presentation is nonspecific. Sedation, dysarthria, confusion, syncope, agitation, falls, or altered mental status can come from many causes. A serum panel that detects lorazepam, alprazolam metabolites, quetiapine, zolpidem, olanzapine, lamotrigine, or multiple benzodiazepines can narrow the medication-exposure question faster than history alone.
That is different from proving overdose intent. A positive screen can mean prescribed use, recent supervised use, extra dosing, drug accumulation, undisclosed co-use, or intoxication. The laboratory result strengthens the exposure side of the case; clinical judgment still has to connect exposure with symptoms, dose, timing, kidney or liver function, co-ingestions, and patient context.
LC-MS/MS Adds Specificity Where Immunoassays Are Blunt
Immunoassays are fast screening tests that use antibody binding to detect a drug class or compound. They are common because they are cheap and automatable, but they can cross-react with unrelated compounds and often cover a limited drug menu.
LC-MS/MS is slower and more technically demanding, but it can identify specific drug-metabolite pairs. Neuropsychiatric drug testing often has to answer broader questions than whether any drug is present.
- Medication-history verification: serum can confirm whether a reported drug is present near the time of testing.
- Adherence questions: a negative result for an expected medication can flag non-adherence, recent discontinuation, wrong medication list, timing issues, or assay-limit questions.
- Current-exposure assessment: serum is better suited than urine for recent circulating exposure.
- Polypharmacy clarification: multiple detected sedatives or antipsychotics can explain nonspecific neurologic or psychiatric presentations.
Chong et al. framed the method as qualitative screening. Qualitative means the test is built to identify whether a target compound is detected, not to report a precise blood concentration for clinical dosing or toxicity thresholds. The study team noted that positive screens may need supplemental quantitative LC-MS/MS for specific analytes when exact concentration matters.
Broader Drug Libraries Trade Off Against Clinical Workflow
The strongest adjacent literature is not general benzodiazepine background; it is other LC-MS/MS screening work asking how wide a clinical toxicology panel can be while remaining practical.
- Smith et al.: 127-analyte broad-spectrum LC-MS/MS screen in serum and urine, using 100 uL sample volumes and solid-phase extraction.2
- Robin et al.: automated plasma method for 42 drugs of abuse using 50 uL plasma and 43 patient samples.3
- Dresen et al.: 700-drug library screening with 1 mL serum or urine and only 4 postmortem samples in the comparison table.4
Chong et al. landed in a different lane. The analyte list was smaller than the largest library-screening methods, but the workflow used 20 uL serum, simple preparation, and more than 1,000 clinical patient specimens. For routine psychiatric and neurologic medication questions, that balance may matter more than sheer analyte count.
Practical tradeoff: a 700-drug library sounds broader, but a smaller panel focused on benzodiazepines, antidepressants, antipsychotics, anticonvulsants, and sedative-hypnotics may be more useful when the clinical problem is current exposure to prescribed neuropsychiatric medication.
Validation Was Strong but Not Complete for All 77 Analytes
The method performed well on the validation metrics the researchers could test. Total precision for calculated concentrations stayed under 30% coefficient of variation for all 77 analytes, and 84% of analytes stayed under 20%. Retention-time precision was under 1.5% coefficient of variation. Mean extraction recovery was 93.1%, and the mean internal-standard-normalized matrix effect was 99.9%.
Coefficient of variation is a way to express measurement variability relative to the average value. Lower values mean repeated measurements cluster more tightly. Matrix effect refers to how proteins, lipids, salts, or other sample components can suppress or enhance the mass-spectrometry signal, making a drug appear weaker or stronger unless the method controls for it.
The main validation caveat is coverage. Accuracy testing reached 60 of the 77 analytes and showed 100% agreement across 138 of 138 checks, but 17 analytes could not be accuracy-tested because suitable materials were unavailable. For another 20 analytes, accuracy relied on a single reference material.
Internal standards were another constraint. The method used 4 internal standards across the 15-minute run to monitor broad chromatographic and ionization behavior. For a qualitative panel, that tradeoff supports workflow speed while leaving some analyte-specific ion suppression or enhancement unresolved.
These limits do not erase the study. They define the right use case: a broad clinical screen that can identify likely current exposure and trigger a more targeted confirmatory or quantitative step when a specific concentration or legal-toxicology conclusion is needed.
Questions About Neuropsychiatric Drug Blood Screening
Does a positive benzodiazepine screen prove misuse?
No. The Chong study showed that benzodiazepines were the most common detected class, but a positive result only shows exposure within the test’s detection window. Misuse requires clinical context: prescription records, dose timing, symptoms, co-detections, and patient history.
Why use serum instead of urine?
Serum is better for recent circulating exposure. Urine is often better for a longer detection window, especially in forensic or substance-use screening, but it can be less direct when the question is what is currently in the bloodstream during confusion, sedation, suspected intoxication, or a medication-history mismatch.
Can this replace therapeutic drug monitoring?
No. Therapeutic drug monitoring measures drug concentrations to judge whether levels fall within a target range for efficacy or toxicity. This assay was qualitative. It can identify whether many drugs are present, but quantitative testing is still needed when the exact concentration drives clinical decisions.
What is the most useful clinical takeaway?
Common psychiatric and neurologic prescriptions can be the relevant toxicology signal. In the Chong dataset, benzodiazepines, antidepressants, antipsychotics, and anticonvulsants accounted for most detections, and emergency suspected-intoxication cases often involved patients with psychiatric histories.
What would make the evidence stronger?
External validation across more hospitals would help. The next useful step is proof that similar serum-screening workflows produce reliable results across laboratories, emergency settings, psychiatric units, and neurologic clinics, even when the analyte list changes.
References
- Chong E, Koo S-E, Kim S-M, et al. Targeted comprehensive screening of neuropsychiatric drugs in serum by LC-MS/MS: method development and three-year clinical utility. Drug Design, Development and Therapy. 2026;20:585730. doi:10.2147/dddt.s585730
- Smith K, Johnson-Davis KL, Shahrokh K. A new broad-spectrum drug screen for 127 analytes by LC-MS/MS. Journal of Applied Laboratory Medicine. 2023;8(2):240-250. doi:10.1093/jalm/jfac105
- Robin T, Barnes A, Dulaurent S, et al. Fully automated sample preparation procedure to measure drugs of abuse in plasma by liquid chromatography tandem mass spectrometry. Analytical and Bioanalytical Chemistry. 2018;410(20):5071-5083. doi:10.1007/s00216-018-1159-7
- Dresen S, Ferreiros N, Gnann H, Zimmermann R, Weinmann W. Detection and identification of 700 drugs by multi-target screening with a 3200 Q TRAP LC-MS/MS system and library searching. Analytical and Bioanalytical Chemistry. 2010;396(7):2425-2434. doi:10.1007/s00216-010-3485-2
- Sauvage FL, Saint-Marcoux F, Duretz B, Deporte D, Lachatre G, Marquet P. Screening of drugs and toxic compounds with liquid chromatography-linear ion trap tandem mass spectrometry. Clinical Chemistry. 2006;52(9):1735-1742. doi:10.1373/clinchem.2006.067116
- Hiemke C, Bergemann N, Clement HW, et al. Consensus guidelines for therapeutic drug monitoring in neuropsychopharmacology: update 2017. Pharmacopsychiatry. 2018;51(1-02):e1. doi:10.1055/s-0037-1600991