A 2026 individual participant data meta-analysis of 1,721 dementia trial participants linked risperidone to cerebrovascular adverse events, HR 4.11 (95% CI 1.77 to 9.51), and major cardiovascular adverse events, HR 2.00 (95% CI 1.23 to 3.26).1 The timing signal is the practical warning: median first cerebrovascular event appeared at 4.3 weeks, and median first major cardiovascular event appeared at 4.8 weeks.
Research Highlights
- Stroke-related events rose sharply: In six randomized dementia trials, risperidone was linked to cerebrovascular adverse events with HR 4.11 (95% CI 1.77 to 9.51; p = 0.001).1
- Cardiovascular events also increased: Major adverse cardiovascular events were higher with risperidone, HR 2.00 (95% CI 1.23 to 3.26; p = 0.006), with 6.8% incidence vs 3.8% on placebo.1
- The risk window arrived early: Median first cerebrovascular and major cardiovascular events appeared at 4.3 and 4.8 weeks, earlier than the common 12- to 16-week review limit.1
- Neurologic side effects accumulated: Somnolence was higher before and after week 4, while extrapyramidal symptoms after week 4 reached OR 2.93 (95% CI 1.68 to 5.08).1
- Risk stratification was incomplete: Baseline cardiac therapy predicted mortality in the risperidone arm, HR 2.87, and major cardiovascular events, HR 2.35, but subgroup analyses were exploratory.1
Behavioral and psychological symptoms of dementia (BPSD) are agitation, aggression, psychosis, sleep disruption, anxiety, mood symptoms, and other neuropsychiatric problems that can make dementia care unsafe or exhausting. Non-drug care is first-line, but antipsychotics still get used when symptoms create urgent risk.
Risperidone is an atypical antipsychotic that blocks dopamine D2 and serotonin 5-HT2A receptors, reducing some psychosis and agitation signals while also increasing sedation, movement symptoms, vascular risk, and other harms. Le et al. sharpened the prescribing question from “is risperidone risky?” to “how quickly do specific risks appear, and which baseline features should make continuation harder to justify?”1
Cerebrovascular Events Appeared Around Week 4
Le et al. pooled raw participant-level data from six placebo-controlled risperidone trials in dementia. Individual participant data meta-analysis means researchers reanalyzed each participant’s trial data instead of only combining published summary estimates, which gives more room to model timing, predictors, and subgroups.
The pooled sample included 1,009 people randomized to risperidone and 712 randomized to placebo. Mean age was 83 years in both groups, around 70% were female, and most had Alzheimer’s disease. Aggression, activity disturbance, and psychosis were the most common baseline symptoms.1
Risk did not wait for the usual end-of-treatment review. Cerebrovascular adverse events occurred in 35 risperidone participants (3.5%) vs 8 placebo participants (1.1%), and the hazard ratio was 4.11. The median first event occurred at 4.3 weeks.
Major adverse cardiovascular events followed the same direction: 69 risperidone participants (6.8%) vs 27 placebo participants (3.8%), HR 2.00. Median onset was 4.8 weeks. Major adverse cardiovascular events included cardiovascular death, stroke, heart failure, unstable angina, and myocardial infarction.
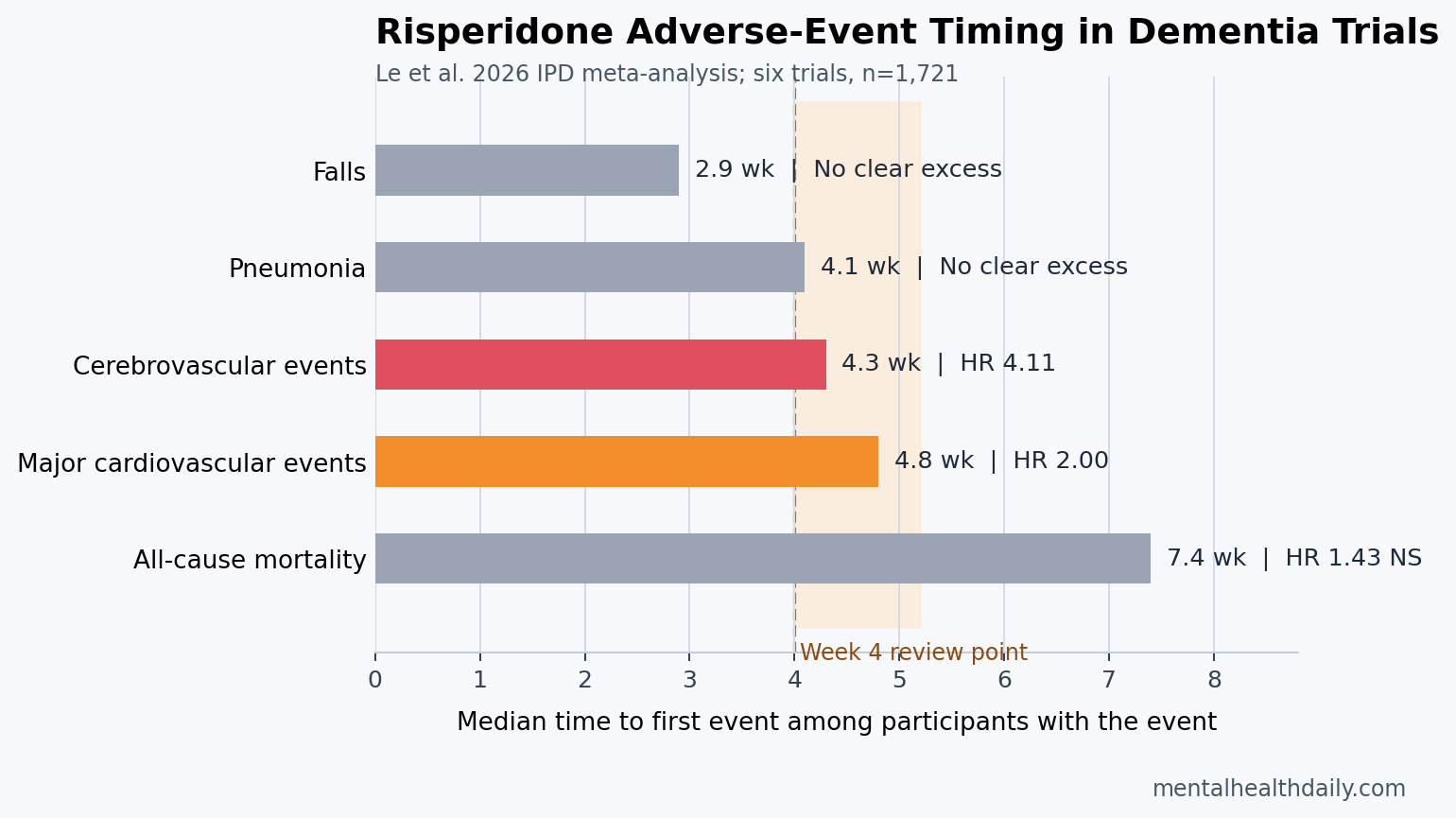
Timing interpretation: the first-event distribution among people who had these events centered near the first month. For a drug often reviewed at 12 to 16 weeks, that is a warning against passive continuation.
Somnolence Started Early, While EPS and Infections Rose After Week 4
Somnolence means clinically noticeable sleepiness or sedation. It was the most frequent short-term adverse effect in the trials, affecting 14% of risperidone participants vs 6.9% of placebo participants before week 4, and 9.9% vs 4.4% after week 4.1
Sedation can look deceptively like treatment success in dementia agitation: a patient may appear calmer because the drug suppresses arousal, not because distress, psychosis, pain, fear, or environmental triggers have been solved. That distinction changes how the benefit-risk tradeoff should be judged.
Extrapyramidal symptoms (EPS) are drug-induced movement problems such as parkinsonism, stiffness, tremor, slowed movement, or restlessness caused mainly by dopamine blockade in motor circuits. EPS was not clearly higher before week 4 after correction, but after week 4 risperidone was linked to EPS with OR 2.93 (95% CI 1.68 to 5.08).1
Upper respiratory tract infections also separated late: 5.2% in the risperidone group vs 2.3% on placebo after week 4, OR 2.31 (95% CI 1.24 to 4.32). The mechanism is less direct than dopamine-blockade movement symptoms, but the clinical consequence is still relevant in frail older adults.
MMSE Decline and Parkinsonism Undercut the Agitation Goal
Mini-Mental State Examination (MMSE) is a brief cognitive test used to track orientation, memory, attention, language, and simple visuospatial performance. Risperidone was linked to lower endpoint MMSE score vs placebo, MD −0.66 points (95% CI −1.14 to −0.17; p = 0.008).1
The point estimate is not a large cognitive-collapse signal, but it runs in the wrong direction for dementia care. A drug used to reduce dangerous agitation can still worsen the cognitive or motor conditions that make wandering, falls, fear, and confusion harder to manage.
Parkinsonism scores also moved against risperidone. The Simpson-Angus Scale showed SMD 0.43 (95% CI 0.25 to 0.61), and the Extrapyramidal Symptom Rating Scale showed SMD 0.25 (95% CI 0.13 to 0.38). Standardized mean difference (SMD) expresses change in standard-deviation units so different scales can be compared.
- Movement burden: stiffness or slowed movement can increase care needs and fall risk even when a fall signal is not statistically confirmed in short trials.
- Cognitive burden: even modest cognitive worsening is more costly in someone whose baseline reserve is already low.
- Behavioral feedback: sedation, infection, parkinsonism, and cognitive decline can themselves worsen distress or apparent BPSD.
Cardiac Therapy, Furosemide, and Antidepressants Flagged Higher-Risk Patients
Baseline cardiac therapy predicted worse outcomes within the risperidone group: mortality HR 2.87 (95% CI 1.34 to 6.12) and major cardiovascular events HR 2.35 (95% CI 1.31 to 4.21). The same predictor was not significant in the placebo group.1
Cardiac therapy in this analysis meant baseline use of medications coded for cardiac disease, used as a proxy for underlying cardiovascular vulnerability when detailed comorbidity data were incomplete. That makes the result clinically plausible but not perfectly specific: the medication category points to risk, not the exact disease mechanism.
Subgroup findings were narrower and should be treated as hypothesis-generating:
- Furosemide: baseline furosemide use significantly interacted with treatment in the mortality model, interaction HR 5.50, but the risperidone effect inside furosemide users did not reach significance (HR 3.46; p = 0.112).
- Musculoskeletal medications: participants using these drugs at baseline had higher fall risk on risperidone, HR 4.65 (95% CI 1.45 to 14.89).
- Antidepressants: baseline antidepressant use marked a larger endpoint sodium reduction with risperidone, MD −2.48 mmol/L (95% CI −4.08 to −0.88).
Evidence-strength note: subgroup analyses in this paper were exploratory and underpowered. They are strong enough to justify extra caution in medication review, not strong enough to build a precise individual calculator from this dataset alone.
Adjacent Evidence Supports a Shorter Prescribing Clock
The trial-level finding fits a broader antipsychotic-in-dementia safety literature. Mok et al. used matched cohort data and found antipsychotic use in dementia was associated with multiple serious outcomes, including stroke, venous thromboembolism, myocardial infarction, heart failure, fracture, pneumonia, and acute kidney injury.2 Observational data cannot erase confounding by symptom severity, but it captures frailer, longer-treated real-world patients than short trials do.
Choma et al. studied risperidone and stroke risk specifically in dementia, including cardiovascular-disease subgroups.3 That paper is adjacent because it asks the same drug-specific safety question in routine care, where baseline cardiovascular disease changes absolute risk even when relative estimates look similar.
Efficacy remains modest. Yunusa et al. found no clean atypical-antipsychotic winner across effectiveness and safety in BPSD, and the Cochrane review of antipsychotics for agitation and psychosis in Alzheimer’s disease and vascular dementia found small symptom benefits with adverse effects including somnolence and extrapyramidal symptoms.45
Le et al.’s companion 2025 IPD meta-analysis reported that response at week 2 could predict response at week 4, which is the benefit-side reason the new paper’s 4-week safety signal has practical force.6 If no concrete improvement is visible by week 2 and the event clock is already moving toward week 4, continued prescribing needs a stronger justification than habit.
What Safer Risperidone Use in Dementia Would Require
For severe aggression or psychosis in dementia, the least misleading reading is not “never use risperidone.” It is stricter: use only for a concrete target symptom, check response early, and treat continuation beyond 4 weeks as an active decision.
A practical risk-benefit review needs several pieces:
- Target symptom: name the behavior being treated, such as dangerous aggression or distressing psychosis, not vague “agitation.”
- Baseline risk: document stroke history, cardiovascular disease, cardiac therapy, dehydration risk, diuretic use, falls, sedation risk, infection vulnerability, and antidepressant use.
- Early response check: evaluate by 2 weeks whether the target symptom improved enough to justify ongoing exposure.
- Week-4 stop point: reassess before the median cardiovascular/cerebrovascular event window becomes a passive continuation problem.
- Deprescribing plan: set the dose-reduction or discontinuation path before starting the drug unless the emergency context makes that impossible.
The strongest clinical use case is narrow: short-term treatment for dangerous or severely distressing psychosis/aggression when non-drug measures are insufficient and the risk is documented. The weakest use case is open-ended sedation of nonspecific restlessness in a person with high cardiovascular vulnerability.
Questions About Risperidone and Dementia Risk
Does risperidone increase stroke risk in dementia?
In the 2026 IPD meta-analysis, risperidone was linked to cerebrovascular adverse events with HR 4.11. A separate population-based study also found elevated stroke risk with risperidone in dementia, making stroke risk one of the central safety concerns.13
Is 12 weeks too long to wait before reviewing risperidone?
For many patients, yes. Guidelines often limit use to 12 to 16 weeks, but this analysis found median first cerebrovascular and major cardiovascular events around 4 to 5 weeks. A 2-week response check and a serious week-4 continuation decision fit the data better than waiting until week 12.
Did risperidone increase mortality in these trials?
All-cause mortality was numerically higher with risperidone, 4.0% vs 3.1%, but the hazard ratio was not statistically significant: HR 1.43 (95% CI 0.77 to 2.63; p = 0.253). That does not cancel the statistically clearer cerebrovascular and cardiovascular signals.
Who looks highest risk before starting risperidone?
People already on cardiac therapy, people with cardiovascular disease or prior stroke risk, and people using furosemide or other medications that mark frailty deserve extra caution. The subgroup findings are not a validated calculator, but they are strong enough to force a medication-risk review.
Can risperidone still be reasonable for severe dementia aggression or psychosis?
Sometimes. The strongest case is short-term, goal-defined use when symptoms are dangerous or severely distressing and non-drug measures are insufficient. The article’s safety signal argues against vague, prolonged, or sedation-centered use.
References
- Le HT, Lau ECY, Lu CY, Hilmer SN, Jeon YH, Low LF, et al. Multiple adverse outcomes associated with risperidone in people with dementia: an individual participant data meta-analysis. CNS Drugs. 2026;40:697–708. doi:10.1007/s40263-026-01282-z
- Mok PLH, Carr MJ, Guthrie B, Morales DR, Sheikh A, Elliott RA, et al. Multiple adverse outcomes associated with antipsychotic use in people with dementia: population based matched cohort study. BMJ. 2024;385:e076268. doi:10.1136/bmj-2023-076268
- Choma J, Griffiths A, Henley W, Mueller C, Williams N, Ballard C, et al. Risk of stroke associated with risperidone in dementia with and without comorbid cardiovascular disease: population-based matched cohort study. British Journal of Psychiatry. 2025. doi:10.1192/bjp.2025.10419
- Yunusa I, Alsumali A, Garba AE, Regestein QR, Eguale T. Assessment of reported comparative effectiveness and safety of atypical antipsychotics in the treatment of behavioral and psychological symptoms of dementia: a network meta-analysis. JAMA Network Open. 2019;2(3):e190828. doi:10.1001/jamanetworkopen.2019.0828
- Mühlbauer V, Möhler R, Dichter MN, Zuidema SU, Köpke S, Luijendijk HJ. Antipsychotics for agitation and psychosis in people with Alzheimer’s disease and vascular dementia. Cochrane Database of Systematic Reviews. 2021;12:CD013304. doi:10.1002/14651858.CD013304.pub2
- Le HT, Lau ECY, Lu CY, Hilmer SN, Jeon YH, Low LF, et al. Treatment modifiers and predictors of risperidone response in dementia: an individual participant data meta-analysis of six randomized controlled trials. Alzheimer’s & Dementia. 2025;21:e70665. doi:10.1002/alz.70665
- Reus VI, Fochtmann LJ, Eyler AE, Hilty DM, Horvitz-Lennon M, Jibson MD, et al. The American Psychiatric Association practice guideline on the use of antipsychotics to treat agitation or psychosis in patients with dementia. American Journal of Psychiatry. 2016;173:543–546. doi:10.1176/appi.ajp.2015.173501