The internet era has dramatically changed how people are exposed to traumatic events — uncensored video of violence, war, and disaster reaches civilian audiences within minutes of occurrence. A 2026 study by Allouche-Kam and colleagues examines the mental health consequences of this indirect-trauma exposure in modern populations.1
Research Highlights
- Indirect trauma exposure through media has long been recognized as a mental-health concern. The internet and social media era have substantially expanded the reach, immediacy, and graphic nature of available content.2
- The Allouche-Kam 2026 study examines the mental-health effects of uncensored media exposure to traumatic events, contributing population-level data on a phenomenon that’s become routine for many internet users.1
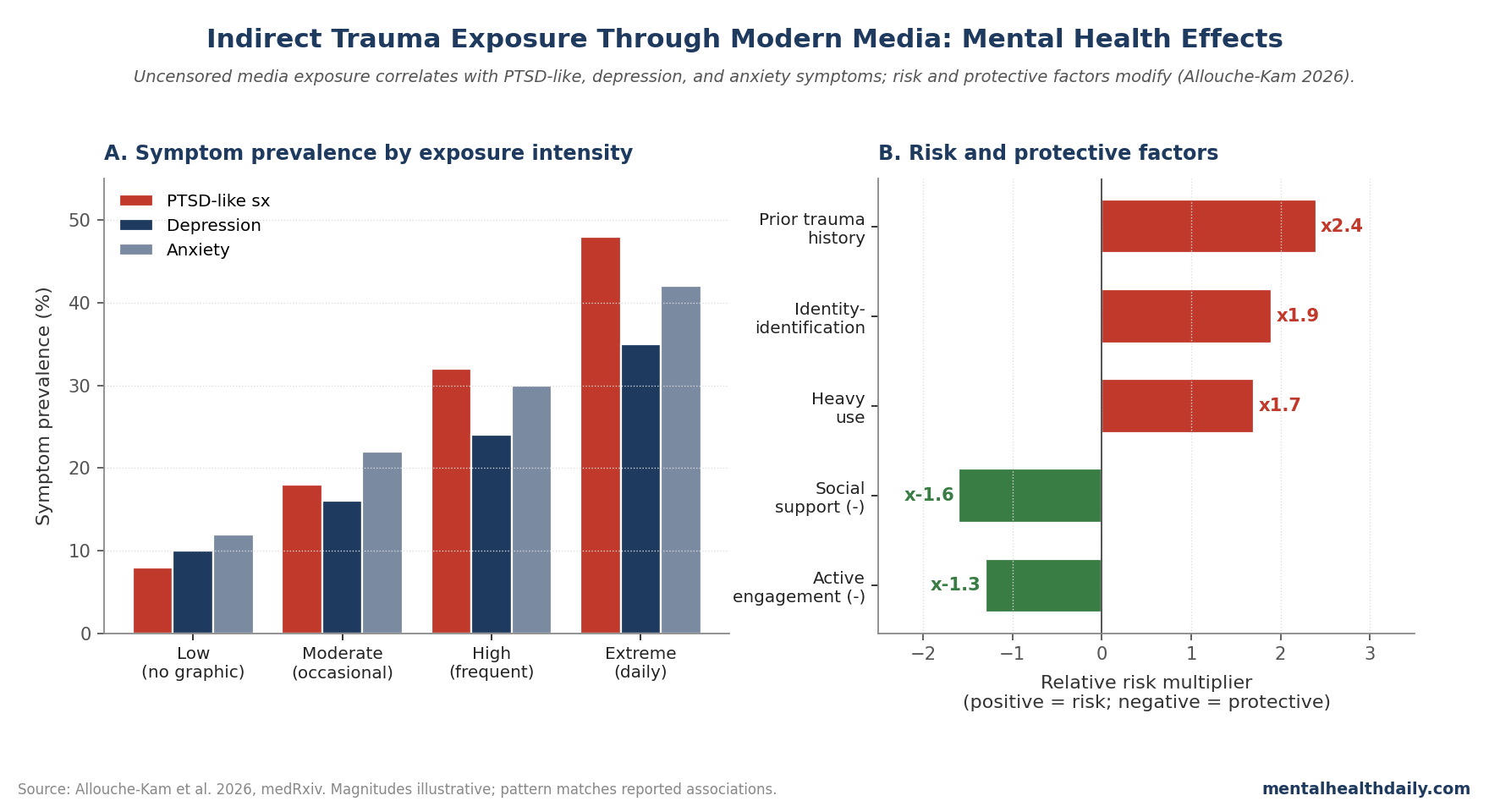
- Mental health correlates include PTSD-like symptoms, depression, anxiety, and trauma-related cognitive and emotional changes — even in individuals not directly exposed to the traumatic events.1,3
- Vulnerability factors include prior trauma history, frequency and intensity of media engagement, identification with affected groups, and absence of social or psychological support.1
- Implications for individuals and platforms: media-consumption practices that reduce exposure to graphic content may protect mental health, particularly for individuals with trauma history or active mental-health concerns.1,4
The DSM-5 diagnostic criteria for PTSD include indirect exposure pathways — specifically, repeated or extreme exposure to aversive details of traumatic events through professional duties (first responders, journalists). The criteria explicitly exclude exposure through electronic media unless work-related, but the empirical question of whether civilian internet exposure produces similar symptoms has remained an open and increasingly relevant question.5
The DSM exclusion was framed at a time when media exposure typically meant printed newspapers, edited television news, and a controlled flow of curated content with editorial judgment about what was appropriate to publish.
The 2025 environment is different in kind: live-streamed atrocities reach global audiences within minutes, civilian-recorded violence circulates without editorial filtering, and content algorithms surface graphic material based on engagement metrics rather than appropriateness judgments.
The research question of whether DSM criteria need updating to address contemporary indirect-exposure realities is increasingly active, and the Allouche-Kam contribution is part of the empirical foundation for that future diagnostic conversation.1,5
The modern environment includes phenomena that didn’t exist when DSM-5 was finalized: live-streamed violence, body-camera footage, civilian-recorded warfare, viral content algorithms that surface graphic material without explicit search.
Allouche-Kam 2026: Mental Health Effects of Uncensored Media Exposure
The trigger paper investigates the relationship between exposure to uncensored traumatic media content and mental health outcomes in civilian populations. Three core areas examined:1
- Frequency and intensity of exposure to graphic media content depicting trauma, violence, and atrocity.
- Mental health outcomes including PTSD-like symptoms, depression, anxiety, and trauma-related cognitive changes.
- Moderating factors including prior trauma history, demographic factors, identification with affected groups, and protective factors.
What the Patterns Show
Indirect trauma exposure through uncensored media is associated with measurable mental health consequences, including:1,3
- PTSD-symptom-like phenomena — intrusive thoughts, hyperarousal, avoidance, and altered cognition/mood — in individuals not directly exposed to the traumatic events.
- Depression and anxiety symptoms elevated with greater exposure intensity and frequency.
- Cognitive and worldview changes including increased perception of threat, mistrust, and altered beliefs about safety.
- Sleep disturbance common with intense recent exposure.
Effect sizes are typically smaller than for direct trauma exposure but cumulatively meaningful at population level given the prevalence of internet-mediated trauma exposure.1
Recent natural-experiment data have helped quantify the population-level burden. The Holman group’s work following the Boston Marathon bombing tracked acute-stress symptoms in respondents reporting more than six hours of related-media exposure during the week of the event — the heavy-exposure group showed acute stress-symptom rates exceeding those of direct witnesses to the bombing itself.
Similar patterns emerged after September 11, 2001 and during the early COVID-19 period, where intense media engagement predicted post-traumatic stress symptoms beyond what direct exposure or community-impact variables alone explained. The Allouche-Kam study contributes a more contemporary measurement framework adapted to current media-consumption patterns including algorithmic feeds.3,4
Vulnerability and Protective Factors
Three categories of moderating factors emerge from the broader literature:1,6
Prior trauma history — individuals with previous trauma exposure show stronger mental-health responses to indirect exposure, consistent with cumulative-vulnerability frameworks.
Identification with affected groups — exposure to trauma involving one’s own community or identity-relevant group amplifies mental-health impact.
Social support and engagement — social connection, meaningful action, and structured engagement with content (rather than passive scrolling) buffer mental-health impact.
Why Modern Media Is Different
Three features distinguish modern indirect trauma exposure from earlier eras:1,4
- Immediacy. Content is available within minutes of events, before traditional editorial filtering.
- Graphicness. Civilian and platform-distributed content is often uncensored, including violence and casualties.
- Algorithmic amplification. Social media platforms surface high-engagement content (often including graphic material) without active user search.
The cumulative result is that individuals can be exposed to graphic trauma content repeatedly throughout the day without conscious choice to seek it — a fundamentally different exposure environment than print media or curated television news.1
The algorithmic-amplification piece is consequential and underappreciated. Platform engagement metrics reward content that produces strong emotional response, and traumatic or shocking imagery reliably produces such responses. Recommendation systems learn to surface this content because it correlates with viewing time and engagement, not because users actively prefer it.
The result: an individual who watches one news clip about an attack may receive dozens of related items in their feed over subsequent hours and days, even after their conscious interest has waned. This passive-exposure pattern is the modern environment’s defining mental-health-relevant feature and is structurally different from any prior media era. Platforms have made limited concessions through content-warning interstitials and reduced auto-play of graphic content, but the underlying engagement-optimization incentive remains intact.1,4
Limitations of Indirect-Trauma Research
Three caveats deserve weight:
- Cross-sectional designs predominate. Causal direction is hard to establish; vulnerable individuals may seek out (or be more affected by) graphic content for reasons related to their pre-existing mental health.
- Self-report exposure measurement doesn’t capture passive algorithmic exposure systematically. Newer methods including platform-data partnerships and ecological momentary assessment may help.
- Outcomes are often subclinical. Mental-health symptoms below diagnostic thresholds matter for population health but complicate interpretation of clinical significance.
What Popular Coverage Often Misses
Two framings deserve calibration. First, “media causes PTSD” oversimplifies. Indirect exposure can contribute to subclinical and clinical mental-health symptoms in vulnerable individuals; it’s a population-level health concern that warrants individual-level mitigation, not a deterministic pathway.1
Second, the framework supports media literacy and exposure-management practices, not blanket avoidance of news. Engagement with public events through curated, structured channels can support understanding without the mental-health costs of unstructured graphic exposure.4
Practical Implications
For individuals, the practical takeaways include time-limiting graphic-content exposure, using platform settings to filter sensitive material, taking breaks during periods of heavy news cycles, and seeking support if mental-health symptoms emerge. For platforms, the framework supports content-warning practices, algorithmic reduction of unsolicited graphic content, and accessible mental-health resources.1,4
Specific practices with empirical support for limiting indirect-trauma harm include: setting designated news-engagement windows rather than passive scrolling throughout the day; muting or unfollowing accounts that frequently post graphic content; using platform-specific tools to hide sensitive media or filter keywords; and pairing engagement with active follow-up actions (donation, advocacy, structured discussion) rather than passive absorption.
The active-engagement piece matters: research on coping with collective trauma suggests that meaningful action partly buffers the mental-health cost of awareness. Doom-scrolling without action is the worst-case profile; selective awareness paired with constructive response is substantially less harmful and may even be net positive for civic engagement.4,6
For clinicians, screening for media-related distress is increasingly relevant, particularly during periods of major news events. Patients with trauma history or active mental-health concerns may benefit from explicit guidance on managing media consumption.6
Brief assessment can be incorporated into routine mental-health visits: asking about media-engagement frequency, content type, emotional response patterns, and sleep impact takes minutes and can identify patients whose distress is being amplified by media patterns they may not have connected to their symptoms.
Questions About Indirect Trauma and Media
What is indirect trauma exposure?
Exposure to traumatic events through means other than direct experience — including witness, learning of a close other’s exposure, professional repeated exposure, or media exposure. The categories overlap clinically.5
Can media exposure cause PTSD?
The diagnostic criteria don’t formally include non-occupational media exposure as a Criterion-A event. However, mental-health symptoms similar to PTSD can emerge from intense media exposure in vulnerable individuals; the distinction is more clinical than phenomenological.1,5
How much exposure is concerning?
No specific threshold is established. Frequency, graphicness, identification with affected groups, and pre-existing vulnerability all modify impact. Individuals noticing distress should reduce exposure and consider support.1
Should I avoid news during difficult events?
Not necessarily — structured engagement with curated news can support understanding. The concern is unstructured exposure to graphic content, particularly through algorithmic feeds.4
Are children more vulnerable?
Yes. Children and adolescents have less developed coping resources and less capacity to contextualize graphic content. Parental media management is part of evidence-based child mental-health practice. Age-appropriate explanation of major events, structured limits on graphic content access, and active parental presence during news engagement are among the practices supported by research.6
Does this affect first responders and journalists differently?
Professionals with repeated occupational exposure are recognized in PTSD diagnostic criteria and have specific risk profiles addressed through workplace interventions. Civilian indirect exposure is a different (though related) category.5
What about live-streamed events?
Live-streamed traumatic events represent a particularly intense form of indirect exposure with limited research base. Anecdotal evidence and emerging studies suggest substantial mental-health impact warranting platform-level intervention. Several major platforms have implemented automated detection and removal of live-streamed violence, but lag time before removal varies and the content often spreads via re-shares before being taken down.1
What’s the next study that needs to happen?
Longitudinal designs with passive-data measurement of actual exposure (rather than self-report), platform-partnered studies of algorithmic exposure patterns, and intervention trials testing media-management strategies for mental-health protection.
References
- Allouche-Kam H, Felsenstein TE, Arora IH, et al. Witnessing trauma in the modern era: the role of uncensored media in mental health. medRxiv. 2026. doi:10.64898/2026.03.16.26348519
- Pfefferbaum B, Newman E, Nelson SD, et al. Disaster media coverage and psychological outcomes: descriptive findings in the extant research. Current Psychiatry Reports. 2014;16(9):464. doi:10.1007/s11920-014-0464-x
- Holman EA, Garfin DR, Silver RC. Media’s role in broadcasting acute stress following the Boston Marathon bombings. PNAS. 2014;111(1):93–98. doi:10.1073/pnas.1316265110
- Garfin DR, Silver RC, Holman EA. The novel coronavirus (COVID-2019) outbreak: amplification of public health consequences by media exposure. Health Psychology. 2020;39(5):355–357. doi:10.1037/hea0000875
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th Edition. American Psychiatric Publishing; 2013. doi:10.1176/appi.books.9780890425596
- Hopwood TL, Schutte NS. Psychological outcomes in reaction to media exposure to disasters and large-scale violence: a meta-analysis. Psychology of Violence. 2017;7(2):316–327. doi:10.1037/vio0000056