
Daytime agitation in dementia fluctuates day-to-day, and a 2026 explanatory study from Liu et al. used contactless under-mattress sensors in 55 long-term-care residents and an external 17-person home-monitoring cohort to show that lower nocturnal respiratory rate and higher activity instability robustly predict next-day agitation occurrence — but not severity.1
Research Highlights
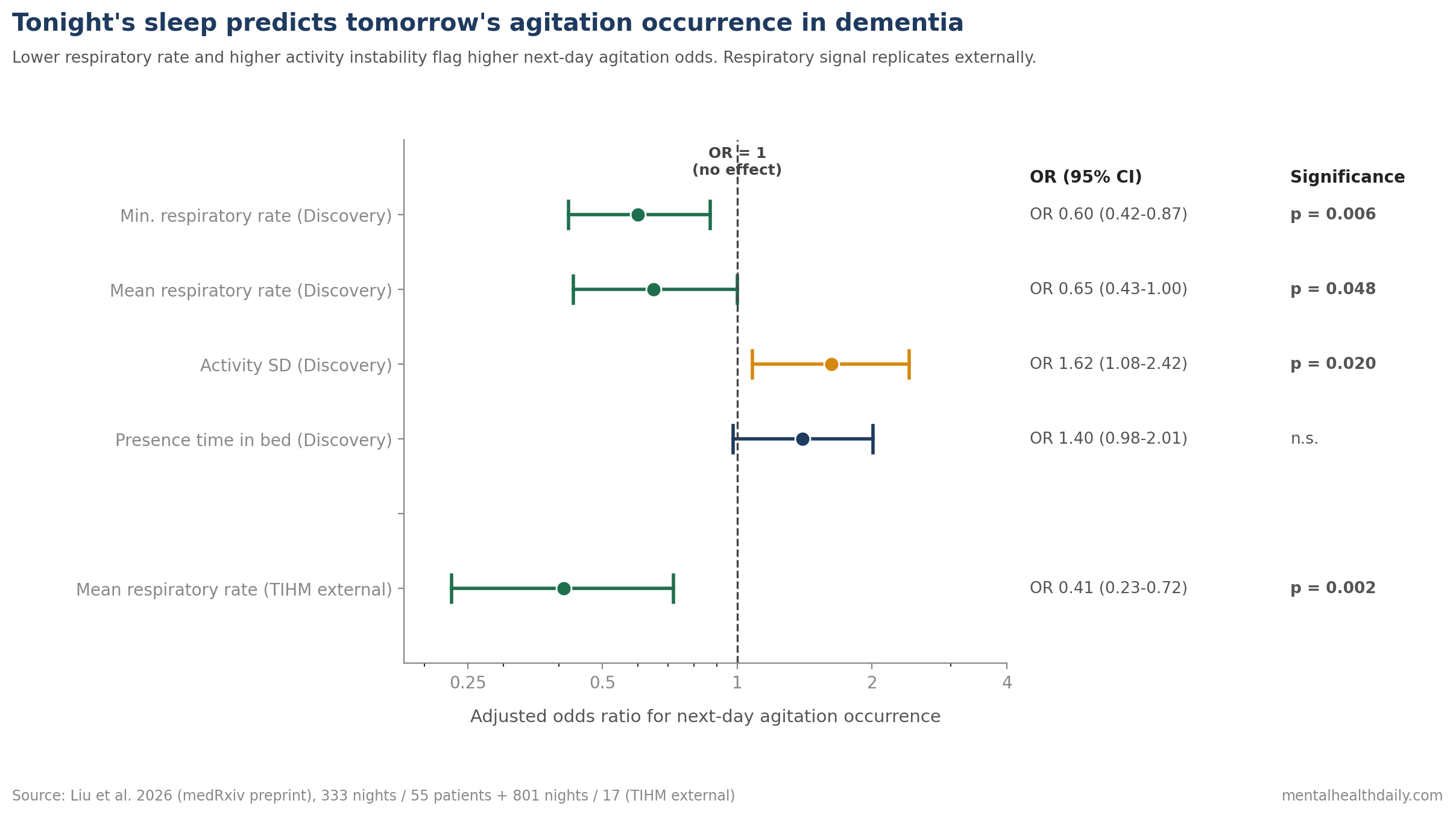
- Lower breathing rate: adjusted multivariable GLMM (generalized linear mixed model) linked lower nocturnal respiratory rate to higher next-day agitation odds: minimum respiratory rate OR 0.60 (95% CI 0.42–0.87, p = 0.006); mean respiratory rate OR 0.65 (CI 0.43–1.00, p = 0.048).1
- Higher activity instability: activity standard deviation predicted agitation with OR 1.62 (95% CI 1.08–2.42, p = 0.020), independent of respiratory features.1
- 17-person home replication: in the TIHM dataset (17 subjects, 801 nights), mean respiratory rate showed OR 0.41 (95% CI 0.23–0.72, p = 0.002) for next-day agitation — a stronger effect than in the discovery cohort. AUC 0.70–0.75.1
- Motor vs. verbal agitation: for motor episodes, minimum respiratory rate OR 0.49 and activity SD OR 1.99. For verbal episodes, only minimum heart rate (OR 0.49) survived FDR correction.1
- Severity near-zero signal: once an episode happens, how bad it gets depends on subject-level traits, not last night’s physiology — severity model marginal R² only 0.031, with patient-specific random intercepts explaining most variance.1
Agitation in dementia drives caregiver burden, safety incidents, and earlier institutionalization. Pharmacological options carry serious risks: antipsychotics in patients with dementia are associated with increased mortality and have an FDA black-box warning.2
Current best practice emphasizes identifying triggers and unmet needs first, with non-pharmacological interventions before drugs. The implementation problem is staffing — care teams cannot watch every patient continuously, and short-term risk stratification has been an unsolved problem.
The Liu study tests whether passive nocturnal monitoring — cheap, unobtrusive, already deployed in some care settings — can flag which patients are at higher agitation risk for the following day.
Liu 2026: Under-Mattress Sensors, Two Cohorts, External Validation
The discovery analysis pooled two long-term care cohorts in Belgium:
- EMFIT cohort: 21 residents (mean age 79.7 years, 11.4 MMSE), 1 week of monitoring with the Emfit QS sensor.
- WSA cohort: 16 residents (mean age 80.2 years, 13.1 MMSE), 2 weeks of monitoring with the Withings Sleep Analyzer.
Both devices use ballistocardiography (BCG) — a technique that detects the tiny mechanical vibrations the heart and breathing produce in the body, recorded through pressure sensors under the mattress without any skin contact or wearable.
The sensors output continuous time-series data on heart rate, respiratory rate, and in-bed activity at 1-minute (WSA) or 4-second (EMFIT) resolution.
The pooled analytical dataset comprised 333 complete observation pairs (sleep night matched to next-day agitation rating) from 55 patients.
An external validation used the TIHM dataset — 17 home-monitored subjects with 801 nights, who differed in setting (home vs. long-term care) and annotation density (twice-daily vs. event-contingent ecological momentary assessment).
Agitation was scored using the Pittsburgh Agitation Scale (PAS), a validated 0–4 instrument across four behavioral subtypes: motor, verbal, aggressive, and resistance to care.
The analytic strategy used a two-part mixed-effects framework: a generalized linear mixed model (GLMM) for whether agitation occurred at all, and a separate cumulative link mixed model (CLMM) for severity among agitation-positive days. False discovery rate (FDR) correction was applied across features.
Lower Respiratory Rate and Higher Activity Variability Predict Next-Day Agitation
The multivariable GLMM, adjusting for age, sex, and cohort, yielded three statistically significant nocturnal predictors of next-day agitation occurrence.1
Minimum respiratory rate was the strongest single predictor. OR 0.60 (95% CI 0.42–0.87, p = 0.006). Translation: a one-unit increase in robust z-scored minimum respiratory rate corresponded to a 40% reduction in the odds of agitation the following day.
Mean respiratory rate showed a similar pattern. OR 0.65 (CI 0.43–1.00, p = 0.048).
Activity standard deviation — how variable the in-bed movement signal was overnight — predicted agitation in the opposite direction. OR 1.62 (CI 1.08–2.42, p = 0.020), corresponding to a 62% increase in agitation odds per unit increase in activity instability.
Presence time in bed was significant in univariate screening but did not retain independent significance in the multivariable model (OR 1.40, p = 0.069).
The model AUC was 0.71 in-sample — modest discriminative performance, but meaningful for a passive, low-cost prediction.
Variance decomposition: marginal R² 0.139 (fixed effects), conditional R² 0.455 (full model), ICC 0.37. Translation: physiological features explain about 14% of agitation variance, patient-level random effects pick up another 31%, and the gap reflects substantial between-subject heterogeneity in baseline agitation propensity.
External Validation: The Respiratory Signal Replicates in Home Monitoring
The TIHM cohort tests generalizability across two important boundaries: setting (home vs. long-term care) and device (different under-mattress sensor with different annotation protocol).
The respiratory signal replicated, and arguably came in stronger:
- Mean respiratory rate: OR 0.41 (95% CI 0.23–0.72, p = 0.002).
- Respiratory rate standard deviation and IQR also showed protective associations.
- AUC 0.70–0.75 for respiratory features alone.
External validation is what separates a hopeful exploratory finding from a candidate clinical tool. The respiratory signal cleared this bar.
Activity-based features could not be tested in TIHM because the public dataset does not provide accessible activity data.
Subtype Differences: Motor Agitation Couples to Sleep, Verbal Agitation Less So
Pittsburgh Agitation Scale subtypes were analyzed separately for motor and verbal episodes (resistance and aggression were too rare for robust modeling).
Motor agitation (pacing, restlessness, repetitive movement) showed strong nocturnal coupling. Minimum respiratory rate OR 0.49, mean respiratory rate OR 0.53, activity SD OR 1.99, minimum heart rate OR also protective.
Verbal agitation (calling out, repeated questions, verbal aggression) showed limited coupling. After FDR correction, only minimum heart rate (OR 0.49) remained significant.
The phenotype-specific pattern is biologically reasonable. Motor agitation has straightforward connections to autonomic regulation and physical restlessness, both of which the under-mattress sensors capture directly. Verbal agitation is more cognitively driven and may require different upstream signals to predict.
Severity Is a Subject-Level Trait, Not a Sleep-Driven State
The two-part modeling separated occurrence (whether any agitation happened) from severity (how intense it was, given that it happened). Severity moved in the opposite direction from occurrence.
Sleep predicted risk, not intensity: no nocturnal sleep feature survived FDR correction as a predictor of severity. Sleep efficiency, total sleep time, sleep latency, awake time, sleep-wake entropy — none predicted how intense the next-day agitation episode would be.1
Patient-level differences explained more: marginal R² was 0.031, meaning fixed sleep and physiology features picked up almost nothing. Conditional R² was 0.292 and ICC was 0.27, so random intercepts — stable differences between people — explained most of what the model could explain.
State vs. trait split: Liu et al. proposed that sleep physiology modulates whether an agitation episode happens, a state-level and potentially modifiable factor. Once agitation starts, intensity appears to reflect more stable patient-level traits — disease stage, temperament, premorbid personality — that do not move from night to night.
Caregivers can use overnight signals to anticipate that an agitation episode is more likely tomorrow, but cannot rely on them to predict whether the episode will be mild or severe.
Practical Read for Clinicians, Caregivers, and Care-Home Operators
- Under-mattress sensing is now an evidence-supported risk-stratification tool. Two devices, two sensing modalities, and an external home-cohort validation converge on the same physiological signature. Care homes deploying these sensors for sleep monitoring can extract additional value as a next-day agitation early-warning system.
- The signature is specific. Lower nocturnal respiratory rate and higher activity instability flag higher next-day agitation odds. Other sleep features (sleep efficiency, sleep latency, awake time) did not predict.
- Use the signal for pre-emptive non-pharmacological care. Heightened agitation risk can trigger increased one-on-one staff attention, environmental adjustments, music or sensory interventions, and extra check-ins — the kind of front-line measures recommended over reflex antipsychotic prescribing.
- Don’t expect severity prediction. The data do not support using nocturnal sensors to forecast how severe an agitation episode will be once it starts. Severity tracks patient-level traits.
- Preliminary — not yet practice-changing. The Liu paper is a medRxiv preprint without peer review at time of analysis. Clinical deployment should wait for peer-reviewed publication and ideally a prospective intervention trial showing that acting on the signal improves outcomes.
What This Study Doesn’t Settle
It is associative, not causal. Lower nocturnal respiratory rate and higher activity variability predict agitation, but the analysis does not establish that intervening on those signals would reduce agitation. The mechanistic chain (autonomic dysregulation, sleep fragmentation, neurodegenerative substrate) needs further work.
The discovery cohort is small. 55 patients across two devices and two annotation protocols. The TIHM external validation strengthens the respiratory finding but the activity-based signal remains discovery-only.
Variance explained by physiology is modest. The marginal R² of 0.14 means most of the night-to-night variation in agitation is not captured by the nocturnal features tested. AUC 0.71 is useful but well short of definitive.
Phenotype generalizability is unclear. Resistance to care and aggression were too rare to model. Whether the same signature applies to those clinically important phenotypes is untested.
Implementation friction is real. Translating an OR or AUC into actionable bedside alerts requires threshold tuning, alarm fatigue management, and integration into existing care workflows — none of which this paper addresses.
Questions About Predicting Dementia Agitation From Sleep
Does this mean caregivers can know in advance which days will be hard?
The data support a probabilistic forecast, not a deterministic one. The model AUC of 0.71 means it correctly orders patients by risk most of the time, not that any individual day’s agitation can be reliably predicted.1
For care planning, that level of accuracy can still be useful: flagging the highest-risk nights to bias staffing and attention is a reasonable use case.
Why would lower respiratory rate predict more agitation the next day?
The most likely interpretation involves autonomic regulation. Lower nocturnal respiratory rate and reduced respiratory variability are associated with autonomic dysregulation, which is known to be more pronounced in advanced dementia and to correlate with overall behavioral instability.1
The mechanistic pathway is not fully established by this study, but the directional pattern is consistent with broader autonomic-symptom literature in dementia.
Why doesn’t the model predict severity?
Severity appears to be more trait-driven than state-driven. The variance decomposition showed that subject-specific random intercepts explained roughly 27% of severity variance, while measured nocturnal physiology explained 3%.1
Translation: who you are (disease stage, temperament, premorbid personality) determines how severe your agitation gets when it happens, more than how you slept the night before.
Is this technology available now?
Yes, both the Emfit QS and Withings Sleep Analyzer are commercially available. The TIHM home dataset uses similar consumer devices.1
Translating a research-grade prediction model into a deployed clinical tool with appropriate alert thresholds is a separate engineering and validation step that has not yet been completed.
What about antipsychotics for agitation?
Antipsychotics in dementia carry an FDA black-box warning for increased mortality. Current guidelines recommend non-pharmacological interventions first and pharmacology only when behavioral approaches fail and risk is high.2
A risk-stratification tool like the Liu model fits squarely in the non-pharmacological strategy: identify high-risk nights, deploy targeted attention and environmental adjustments before agitation escalates.
References
- Dissociating the nocturnal physiological drivers of agitation occurrence and severity in dementia: an explanatory study using contactless sleep sensing. Liu Z et al. medRxiv (preprint). 2026. doi:10.64898/2026.02.27.26346707
- The American Psychiatric Association Practice Guideline on the Use of Antipsychotics to Treat Agitation or Psychosis in Patients With Dementia. Reus VI et al. American Journal of Psychiatry. 2016;173(5):543-546. doi:10.1176/appi.ajp.2015.173501
- Sleep disturbance and risk of cognitive decline: a longitudinal analysis with the Wisconsin Registry for Alzheimer’s Prevention. Spira AP et al. Neurobiology of Aging. 2019;79:127-134. doi:10.1016/j.neurobiolaging.2019.03.014
- A meta-analysis of cytokines in Alzheimer’s disease. Swardfager W et al. Biological Psychiatry. 2010;68(10):930-941. doi:10.1016/j.biopsych.2010.06.012
- Behavioural and psychological symptoms of dementia: a seven-tiered model of service delivery. Brodaty H, Draper B & Low LF. Medical Journal of Australia. 2003;178(5):231-234. doi:10.5694/j.1326-5377.2003.tb05169.x