A 2026 medRxiv genetic analysis linked type 2 diabetes and 2-hour postprandial glucose — the blood-sugar rise after an oral glucose challenge — to higher lacunar stroke risk, with a stronger direct signal for post-meal glucose than for HbA1c after adjustment for brain small-vessel imaging markers.1
Research Highlights
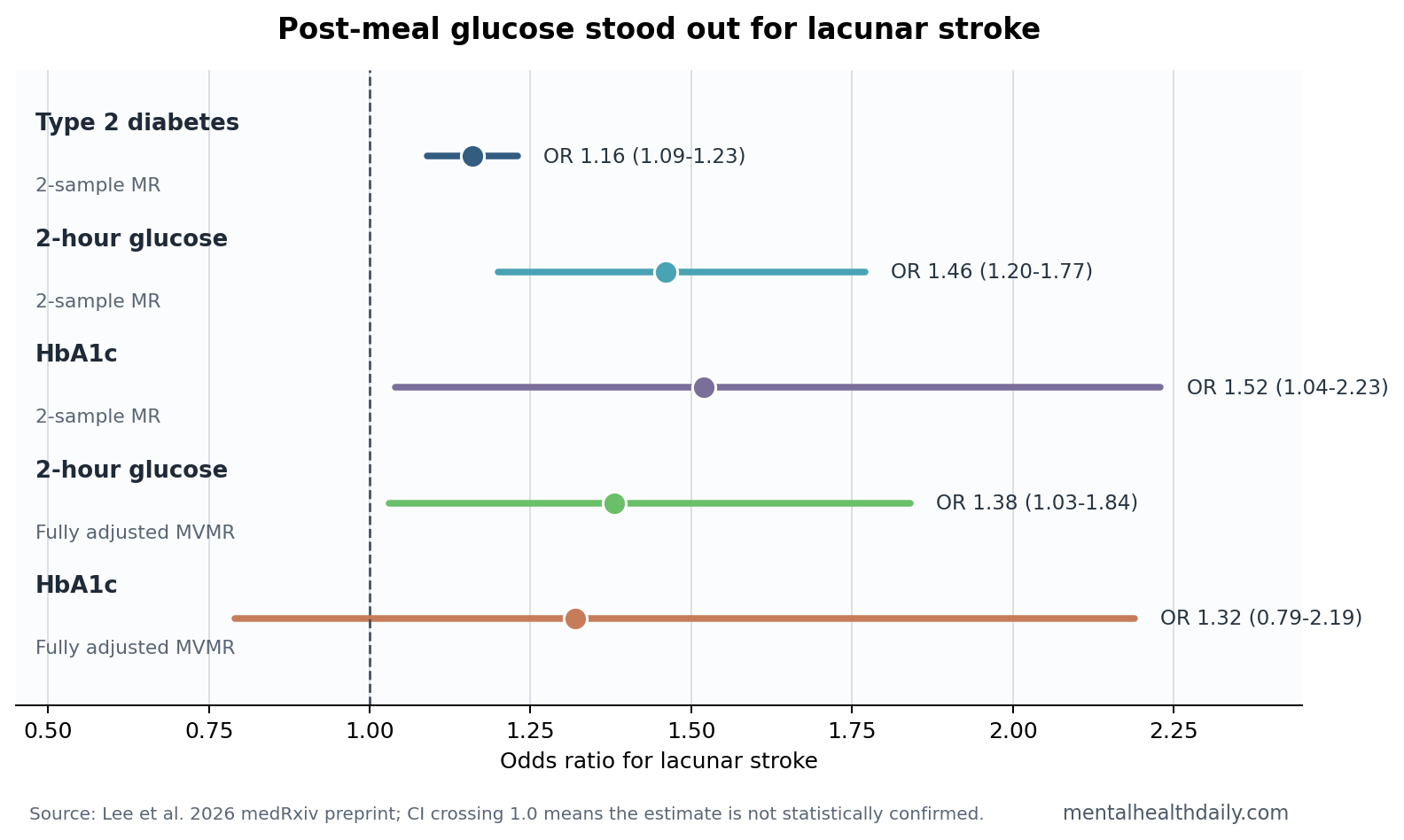
- Lacunar stroke was the clearest endpoint: genetically predicted type 2 diabetes raised lacunar stroke risk by OR 1.16, while 2-hour postprandial glucose raised it by OR 1.46 in 2-sample Mendelian randomization.1
- Average glucose was less direct: HbA1c reached OR 1.52 in the 2-sample model, but the fully adjusted multivariable model weakened to OR 1.32 with a 95% CI crossing 1.0.1
- Shared biology had locus-level support: Lee et al. identified 14 independent pleiotropic loci after screening 568 significant SNPs, including immune-linked MICB and HLA-region signals.1
- Small-vessel disease remains broader than glucose: prior work connects diabetes with stroke, cognitive dysfunction, depression, and small-vessel brain injury, but the strongest causal genetic read here was not every MRI marker equally.2,3
- Evidence strength is still limited: this was an unreviewed preprint using summary-level GWAS data, mostly European-ancestry datasets, and only 10-13 genetic instruments for 2-hour glucose.1
Cerebral small vessel disease refers to injury in the brain’s tiny perforating arteries, arterioles, capillaries, and venules. Its common clinical faces include lacunar stroke, white matter hyperintensities on MRI, cerebral microbleeds, enlarged perivascular spaces, gait impairment, cognitive decline, and depression symptoms tied to vascular brain injury.2,3
Diabetes has long been treated as a small-vessel disease risk factor, but the useful question is more specific: which glucose-related signal maps most cleanly onto which brain endpoint? Lee et al. sharpened that question by combining pleiotropy mapping, genetic correlation, 2-sample Mendelian randomization, and multivariable Mendelian randomization across diabetes, glycemic traits, and several small-vessel phenotypes.1
2-Hour Postprandial Glucose Had the Strongest Lacunar Stroke Signal
Mendelian randomization uses genetic variants as proxy instruments for an exposure, such as type 2 diabetes or 2-hour glucose, to estimate whether lifelong genetic liability to that exposure is associated with an outcome. It is not a randomized trial, but it is less vulnerable to some ordinary confounding than a standard observational cohort.
In Lee et al., the headline result was endpoint-specific. Genetically predicted type 2 diabetes was associated with lacunar stroke risk at OR 1.16 (95% CI 1.09-1.23). Genetically predicted 2-hour glucose after oral glucose challenge had a larger point estimate, OR 1.46 (95% CI 1.20-1.77). HbA1c, a marker of average glucose exposure over roughly 2-3 months, also reached OR 1.52 (95% CI 1.04-2.23) in the simpler 2-sample model.1
The multivariable analysis made the story narrower. When the researchers adjusted the postprandial-glucose signal for individual small-vessel imaging markers, the association with lacunar stroke remained significant in most models, with ORs from 1.34 to 1.40. In the fully adjusted model that included all small-vessel imaging phenotypes at once, the point estimate stayed similar at OR 1.38, but statistical support weakened (95% CI 1.03-1.84; p = 0.074).1
Instrument strength matters here: the 2-hour postprandial glucose models used only 10-13 genetic variants, but the reported F-statistics were 57.46-59.83.1 In plain terms, the instruments were not obviously weak, but the small number of variants still limits precision and makes the post-meal glucose result a focused signal rather than a broad clinical screening rule.
HbA1c looked different: after the same multivariable adjustment, HbA1c no longer showed a significant direct association with lacunar stroke (OR 1.32; 95% CI 0.79-2.19; p = 0.293). That pattern does not make HbA1c irrelevant. It suggests that average chronic glucose exposure may be partly routed through existing structural small-vessel injury, while post-meal glucose excursions may carry a more direct acute-microvascular signal.
The Genetic Signal Was Stronger for Lacunar Stroke Than for White Matter Hyperintensities
Small-vessel disease is a family of related phenotypes, not one endpoint. Lacunar stroke means a small, deep ischemic stroke caused by occlusion of a penetrating artery. White matter hyperintensities are bright MRI lesions that often reflect chronic small-vessel injury, but they are not the same event as an acute lacunar infarct.
That distinction shaped the result. Lee et al. reported positive genetic correlations between type 2 diabetes, fasting glucose, postprandial glucose, and several small-vessel phenotypes, including white matter hyperintensity volume, lacunar stroke, and perivascular spaces. But their Mendelian-randomization signal was clearest for lacunar stroke, not for white matter hyperintensity volume.1
Clinical read: the preprint does not justify saying that post-meal glucose spikes directly cause every brain MRI marker of small-vessel disease. The more defensible claim is narrower: genetic liability to diabetes biology, especially postprandial glucose dysregulation, pointed most strongly toward lacunar stroke risk.
Broader literature: Wardlaw et al. described small vessel disease as a major mechanism behind stroke and cognitive decline, while emphasizing that its imaging features and clinical consequences are heterogeneous.2 Diabetes-focused reviews likewise connect cerebral microvascular injury to stroke, cognitive dysfunction, and depression, while leaving room for endpoint-specific mechanisms.3
Immune Genes Pointed Toward Metabolic-Vascular Inflammation
Lee et al. did not rely only on causal modeling. Their PLEIO analysis — a method for finding genetic loci that jointly associate with multiple traits — first identified 568 significant pleiotropic SNPs and then retained 14 independent loci linking glycemic traits with small-vessel disease phenotypes.1
Mechanism handle: several loci sat near immune-related genes, including MICB and HLA-region genes. MICB encodes a stress-induced immune signal involved in natural-killer-cell and CD8+ T-cell activation, while HLA class II genes are central to antigen presentation. In reader language, the genetic overlap pointed toward immune surveillance, vascular inflammation, and endothelial stress alongside glucose biology.
The proposed biology is plausible. Postprandial hyperglycemia can trigger oxidative stress, protein kinase C activation, advanced glycation end-product formation, and inflammatory responses. Small perforating arteries in subcortical brain regions have limited collateral blood supply, so endothelial injury in those vessels has a plausible path to lacunar infarction.1
Prior genomics work also supports a multi-pathway view of small-vessel disease. Sargurupremraj et al. mapped cerebral small-vessel-disease genomics across the lifespan, while Traylor et al. focused specifically on lacunar-stroke genetics.4,5 Lee et al. add a diabetes and glycemic-trait layer to that landscape rather than replacing it with a single-glucose explanation.
What This Preprint Can and Cannot Support
This is a useful genetic triangulation paper, not a clinical treatment trial. Its strongest contribution is separating 3 ideas that often get blurred:
- Diabetes liability: genetically predicted type 2 diabetes tracked lacunar stroke risk.
- Post-meal glucose excursions: 2-hour glucose showed the most distinctive direct signal after adjustment for small-vessel imaging markers.
- Average glycemic exposure: HbA1c looked important in simpler models but less independently convincing after multivariable adjustment.
Evidence-strength note: the preprint cannot prove that lowering 2-hour postprandial glucose will prevent lacunar stroke. Summary-level GWAS data cannot test individual-level medication use, diet, exercise, blood pressure treatment, kidney disease, sleep apnea, or social risk. Most source data came from European-ancestry populations, partial sample overlap could bias estimates, and residual pleiotropy can survive sensitivity checks.
That limit is important for patient interpretation. A clinician can use post-meal glucose as one vascular-risk clue, especially in diabetes patients with other small-vessel risks, but this genetic analysis does not say that continuous glucose monitoring, a specific diet, or a specific diabetes drug prevents lacunar stroke. It mainly identifies postprandial glycemia as a biologically plausible target for future outcome studies, ideally with adjudicated stroke endpoints and ancestry-diverse replication cohorts.
The 2-hour glucose instrument set was also small: only 10-13 variants, although reported F-statistics from 57.46 to 59.83 argue against a weak-instrument-only explanation. The correct practical read is not “post-meal glucose is the new stroke test.” It is that postprandial glucose deserves more attention in vascular brain-risk research than an HbA1c-only model would give it.
Questions About Post-Meal Glucose and Lacunar Stroke
Does this mean post-meal glucose spikes cause lacunar stroke?
Not by itself. Mendelian randomization supports a causal interpretation more strongly than ordinary correlation, but this was a preprint analysis of genetic summary statistics, not a trial that lowered postprandial glucose and counted strokes.
Is HbA1c still relevant for brain vascular risk?
Yes. HbA1c was associated with lacunar stroke in the 2-sample model, and average glycemic exposure remains clinically important. The narrower point is that HbA1c did not retain the same direct signal after adjustment for small-vessel imaging phenotypes, while postprandial glucose stayed directionally stronger.
Why focus on lacunar stroke instead of all small-vessel disease?
Lacunar stroke is a discrete small-vessel ischemic event. White matter hyperintensities, microbleeds, and perivascular spaces are related but not interchangeable. Lee et al. found the clearest causal genetic signal for lacunar stroke, so stretching the result to every imaging marker would overstate the evidence.
What would make this clinically stronger?
Replication in larger and more ancestrally diverse GWAS datasets, stronger postprandial-glucose instruments, and prospective studies that track glucose excursions, MRI small-vessel changes, cognition, mood, and lacunar events in the same people would make the inference more clinically useful.
References
- Lee KJ, Lee JY, Lee SJ, Bae HJ, Sung J. Shared Genetic Architecture and Causal Relationship Between Diabetes, Glycemic Traits, and Cerebral Small Vessel Disease. medRxiv. 2026. doi:10.64898/2026.04.16.26351065
- Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurology. 2019;18:684-696. doi:10.1016/s1474-4422(19)30079-1
- van Sloten TT, Sedaghat S, Carnethon MR, Launer LJ, Stehouwer CDA. Cerebral microvascular complications of type 2 diabetes: stroke, cognitive dysfunction, and depression. Lancet Diabetes & Endocrinology. 2020;8:325-336. doi:10.1016/s2213-8587(19)30405-x
- Sargurupremraj M, Suzuki H, Jian X, et al. Cerebral small vessel disease genomics and its implications across the lifespan. Nature Communications. 2020;11. doi:10.1038/s41467-020-19111-2
- Traylor M, Persyn E, Tomppo L, et al. Genetic basis of lacunar stroke: a pooled analysis of individual patient data and genome-wide association studies. Lancet Neurology. 2021;20:351-361. doi:10.1016/s1474-4422(21)00031-4
- Duperron MG, Knol MJ, Le Grand Q, et al. Genomics of perivascular space burden unravels early mechanisms of cerebral small vessel disease. Nature Medicine. 2023;29:950-962. PubMed