Research Highlights
- The “kids of mentally ill parents do worse” idea flattens a significant gradient. Across 109 studies and 1.6 million participants, parental schizophrenia produced a moderate pooled deficit (SMD −0.46), bipolar disorder a small-to-moderate one (−0.28), and MDD a small one (−0.22).1
- The largest single number is the least precise. SMD −1.07 for general cognition in offspring of parents with schizophrenia carries a 95% CI from −1.92 to −0.22, the schizophrenia literature shows significant small-study effects (Egger’s p = 0.005), and the highest-quality studies report a smaller deficit (SMD −0.27).1
- The hardest-hit domains differ by parental diagnosis. Schizophrenia hits IQ, language, memory, attention, and executive function. Bipolar hits memory, executive function, IQ, and language. MDD hits IQ, general cognition, language, and executive function more modestly.1
- For bipolar disorder, deficits widen with age (β = −0.73, 95% CI −1.36 to −0.10 for adulthood vs. early childhood). Early-childhood testing alone may understate eventual cognitive impact.1
- These are population means, not individual fates. An SMD of −0.46 still means the distributions overlap more than they differ. Most children of parents with severe mental illness fall within the typical cognitive range for their age.
Roughly 4−6% of children grow up with a parent diagnosed with schizophrenia, bipolar disorder, or major depressive disorder.2 Coverage of that fact lands in one of two places: a generic warning about heritable risk, or a reassuring “most kids turn out fine.”
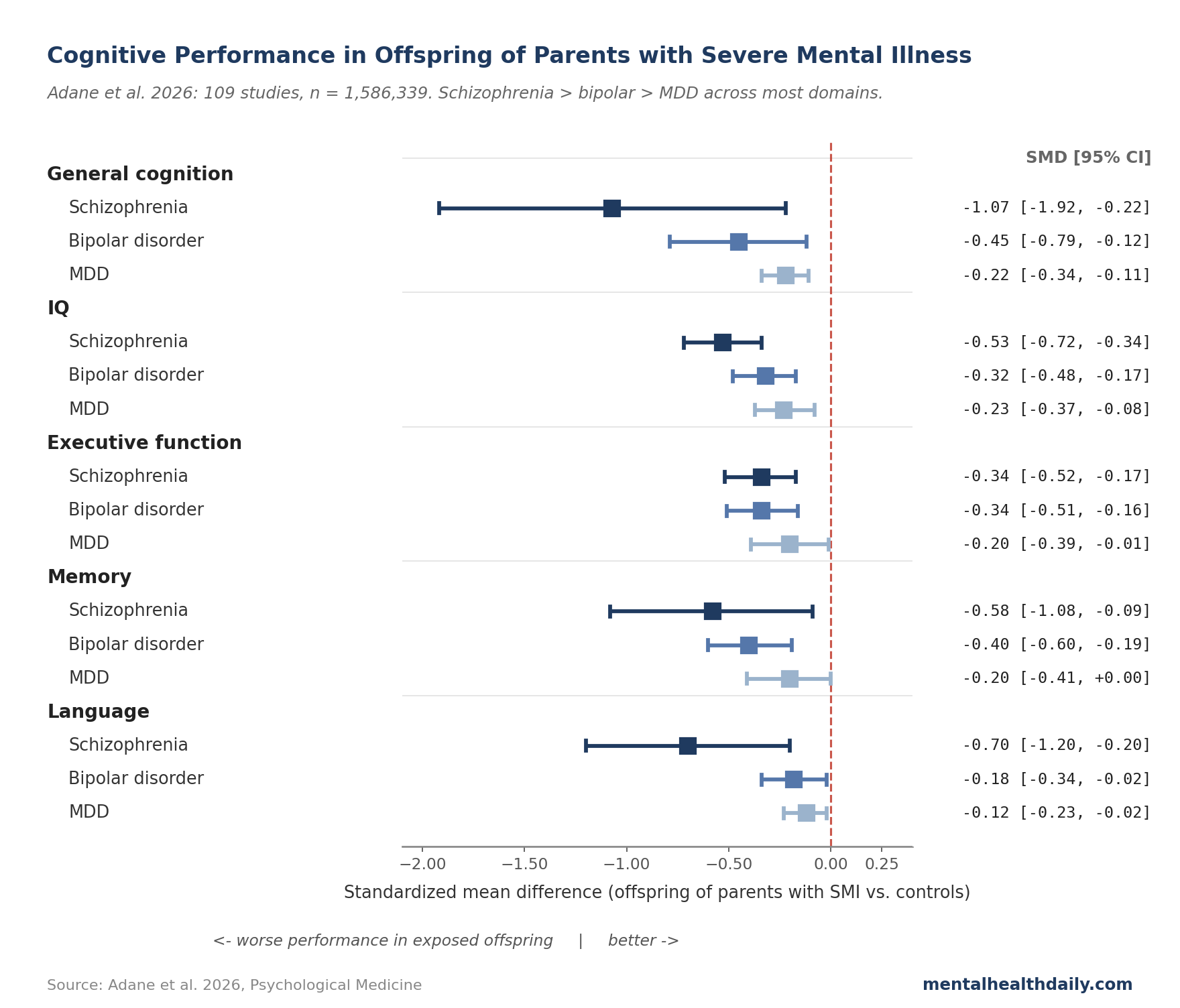
Adane and colleagues’ 2026 meta-analysis in Psychological Medicine — the largest synthesis to date, 109 studies and 1.6 million participants — lets the picture get more specific. There is a clear gradient by parental diagnosis, the hit lands on different cognitive domains depending on the condition, and the effect sizes that travel best in headlines are the ones with the widest confidence intervals.
The Gradient: Schizophrenia > Bipolar > MDD
Adane and colleagues pooled SMDs (standardized mean differences — a way to combine studies that used different cognitive tests onto one scale, where 0.2 is small, 0.5 is moderate, and 0.8 is large) across nine cognitive domains for each parental diagnosis.1 The picture splits cleanly by which condition the parent has.
- Parental schizophrenia: SMD −0.46 (95% CI −0.59 to −0.34). Moderate, with confidence intervals well clear of zero. IQ shows a reliable hit (SMD −0.53), with executive function (−0.34), attention (−0.33), memory (−0.58), and language (−0.70) close behind. General cognition shows the largest point estimate (−1.07) but also the widest confidence interval — more on that below.
- Parental bipolar disorder: SMD −0.28 (95% CI −0.36 to −0.20). Small-to-moderate. Memory (−0.40), executive function (−0.34), IQ (−0.32), and general cognition (−0.45) all show reliable hits. Attention, processing speed, social cognition, and academic performance don’t reach statistical significance, though most point estimates lean negative.
- Parental MDD: SMD −0.22 (95% CI −0.30 to −0.15). Small but reliably non-zero. The hits cluster on IQ (−0.23), general cognition (−0.22), language (−0.12), and executive function (−0.20).
The gradient is informative about mechanism. Schizophrenia carries the largest effect, broadest reach, and strongest genetic loading; lower premorbid IQ has been documented in people who later develop schizophrenia and in their unaffected relatives, suggesting some of the offspring deficit reflects shared genetic risk for cognition itself rather than just a downstream consequence of being raised by an affected parent.3
MDD’s smaller effect is consistent with older work on first-degree relatives of people with depression: small but reliable cognitive differences, mostly on executive function and verbal abilities.4
Interpreting the Headline Numbers
Coverage of meta-analyses tends to lead with the biggest effect size, and here that’s general cognition in offspring of parents with schizophrenia: SMD −1.07, close to a full standard deviation below average. Three reasons to read it as the least precise of the headline numbers, not the most.
- The confidence interval is enormous. The 95% CI runs from −1.92 to −0.22 — consistent with anything from a small deficit to an unusually large one. The underlying studies disagree by nearly an order of magnitude on how big the gap is.
- Small-study effects are documented. Egger’s test for funnel-plot asymmetry — a test for whether small studies systematically report larger effects than big ones, often a sign of publication bias — was significant for the schizophrenia studies (p = 0.005) and borderline for bipolar (p = 0.050). The Precision Effect Test confirmed significant small-study effects for schizophrenia (β = 2.18, p = 0.032). When small trials with flattering results are over-represented, the pooled deficit is probably inflated.
- Study quality matters a lot for schizophrenia. Low-quality studies produced an SMD of −0.87, moderate-quality −0.53, and high-quality only −0.27. A more than 3-fold range in apparent effect size depending on which slice of the literature you look at. The authors’ meta-regression confirmed quality as a significant moderator (β for low vs. high quality = −0.63, p < 0.05).
The most defensible read on parental schizophrenia is the pooled overall SMD of −0.46, which the high-quality subset roughly aligns with. The general-cognition headline of −1.07 leans correct in direction but partly inflated by which trials made it into print. The directional point estimate — that general cognition is hit harder than other domains in this group — survives; the magnitude shrinks.
What the Domain-Specific Pattern Tells You
The domains that get hit aren’t random. Two patterns map onto what to watch for in practice.
- Executive function and IQ show up across all three diagnoses. Both hit reliably for schizophrenia and bipolar (SMDs around −0.32 to −0.34) and for MDD (around −0.20 to −0.23). Executive function — the cluster of skills involved in planning, working memory, attention switching, and impulse control — is among the most heritable cognitive domains and overlaps with the prefrontal-cortex circuits implicated in all three conditions. The shared deficit suggests a partly shared genetic and neurodevelopmental substrate.
- Memory and language show a sharper gradient. Memory shows a moderate hit in schizophrenia (SMD −0.58) and bipolar (−0.40) but doesn’t reach significance in MDD. Language shows a large hit in schizophrenia (−0.70), smaller in bipolar (−0.18) and MDD (−0.12). Klimes-Dougan and colleagues’ review of bipolar offspring found similar domain-specificity, with more uncertainty given smaller sample sizes.5
Domains that mostly escape: academic performance and processing speed don’t reach significance in any group, attention is hit only in schizophrenia, and social cognition is largely spared. The pattern matters more than any single score — in a family affected by parental schizophrenia, a verbal-IQ subtest in the 30th percentile is something the literature predicts; an isolated slow processing-speed score is not.
Distributions May Overlap More Than People Think
Effect sizes in standardized units are easy to misread as predictions for individual children.
An SMD of −0.46 — the overall figure for offspring of parents with schizophrenia — corresponds to roughly a 63% chance that a randomly chosen exposed child scores below a randomly chosen control child on a given cognitive measure. The overlap between distributions is far larger than the gap.
Most children of parents with severe mental illness fall within the typical range for their age. The pooled deficits describe shifted means at the population level, not deterministic outcomes.
Rasic and colleagues’ 2014 family-high-risk meta-analysis on offspring mental-illness risk found similar overlap: elevated risk relative to general-population offspring, but the majority of high-risk children did not develop a serious mental illness.6
The findings are useful for what to monitor and what early supports might help. They aren’t a forecast for any specific child — genetic loading, environmental quality, parental treatment status, household stability, and access to early childhood services all shift the distribution in either direction.
Potential Limitations to Consider: Parental Mental Illness vs. Offspring Cognition
Even with 109 studies and 1.6 million participants, several constraints shape how strongly to read the conclusions.
Studies disagree on the size of the effect. The τ² values (a measure of how much the true effect varies across studies, beyond sampling error) range from 0.06 to nearly 1.2 across domains. Cognitive assessments, ages at testing, and sample-selection methods vary widely.
Risk of bias is mostly moderate. 65 of 109 studies were rated moderate quality on the Newcastle-Ottawa Scale, with 45 high and 15 low. The high-quality subset produces a smaller effect for schizophrenia (SMD −0.27 vs. pooled −0.46). Whether the “true” effect is closer to the high-quality estimate or the pooled one depends on whether the quality differences reflect bias inflation or real differences in which families got recruited.
Paternal exposure is undermeasured. Too few studies isolated paternal SMI for maternal-vs.-paternal comparisons. Mechanisms that run through pregnancy and early caregiving are harder to disentangle from genetic transmission when fathers aren’t separately measurable.
The literature is high-income-country dominated. 51 studies came from North America, 32 from Europe, 26 from elsewhere. Generalizability to low- and middle-income contexts — where access to mental-health treatment and early-intervention services differs sharply — is limited.
Cross-sectional age comparisons aren’t longitudinal. The bipolar age effect — deficits larger in adulthood than early childhood — is based on different cohorts at different ages, not the same children followed across development. Whether the gap genuinely widens or whether selection effects shape who participates in adult studies isn’t pinned down without prospective follow-up.
Implications for Parents and Clinicians
The findings point toward practical implications that don’t require deciding between “everything’s fine” and “everything’s determined.”
- The gradient is informative for monitoring, not labeling. Children of parents with schizophrenia warrant closer developmental tracking on IQ, language, and executive function than children of parents with MDD. Routine pediatric developmental screening — as a way to catch and address gaps early, not as a diagnostic exercise — has the strongest case in this group.
- Environmental factors are large and modifiable. Early-childhood adversity, chronic stress, disrupted caregiving, and lower socioeconomic status are well-documented risk factors for impaired cognitive development on their own,7 and they stack on top of any genetic loading. Parental treatment, predictable caregiving routines, and high-quality early-childhood education each shift the distribution in the right direction.
- Parental treatment matters for the child, not just the parent. Effective treatment of the parent’s condition reduces the home-environment risk factors most directly tied to offspring cognitive outcomes. Medication adherence, therapy engagement, and crisis-prevention planning have the most direct downstream effect on caregiving capacity.
- The pattern is not a forecast. Treating the meta-analytic gradient as a personal prediction overshoots both ways — overestimating risk for any single family and underestimating the population-level case for early supports.
- Wrap-around supports have evidence behind them. Nurse home-visiting programs and integrated parent-infant mental health services have track records for improving outcomes in high-risk families.8 Effect sizes are modest individually, but the supports are low-risk and the alternative is doing nothing.
Common Questions: Parental Mental Illness vs. Children’s Cognition
If I have schizophrenia or bipolar disorder, will my child have learning problems?
On average, exposed children score somewhat lower on cognitive tests — about half a standard deviation for schizophrenia, less for bipolar, less still for MDD. The distributions overlap heavily; most exposed children fall within the typical range. The averages tell you what to watch for, not what will happen to any specific child.1
Which conditions affect children’s cognition the most?
Parental schizophrenia produces the largest deficits (pooled SMD −0.46, hits across IQ, language, memory, attention, and executive function). Parental bipolar disorder produces smaller deficits (−0.28), concentrated on memory, executive function, and IQ. Parental MDD produces the smallest reliable effect (−0.22), mostly on IQ and language.1
Is this because of genetics or environment?
Both, in proportions that vary by condition. Schizophrenia carries strong genetic loading for cognitive ability itself — lower premorbid IQ shows up in unaffected relatives.3 Environmental factors — early-life stress, caregiving disruption, socioeconomic status — are also large and more modifiable.7 The cognitive gap reflects both pathways; the environmental side is where intervention has leverage.
Are these problems permanent?
The pooled deficits persist from childhood into adulthood across the included studies, and for parental bipolar disorder the gap appears to widen with age. But the within-individual trajectory varies; many children show improvement with stable parenting, parental treatment, and early supports.1
What should I do if I have severe mental illness and want to understand my child’s risk?
Focus on your own treatment — consistent care for the parent reduces home-environment risk factors directly. Ask your child’s pediatrician about routine developmental screening so any gaps surface early. Look into whether your family qualifies for nurse home-visiting or integrated parent-infant mental health services.8
References
- Cognitive performance in offspring of parents with severe mental illness: a meta-analysis. Adane AA et al. Psychological Medicine. 2026;56:e115. doi:10.1017/S0033291726103985
- Prevalence of serious mental illness among parents in the United States: results from the National Survey of Drug Use and Health, 2008-2014. Stambaugh LF et al. Annals of Epidemiology. 2017;27(3):222-224. doi:10.1016/j.annepidem.2016.12.005
- Premorbid IQ in schizophrenia: a meta-analytic review. Woodberry KA, Giuliano AJ, Seidman LJ. American Journal of Psychiatry. 2008;165(5):579-587. doi:10.1176/appi.ajp.2008.07081242
- Cognitive performance in first-degree relatives of individuals with vs without major depressive disorder: a meta-analysis. MacKenzie LE, Uher R, Pavlova B. JAMA Psychiatry. 2019;76(3):297-305. doi:10.1001/jamapsychiatry.2018.3672
- Intellectual functioning in offspring of parents with bipolar disorder: a review of the literature. Klimes-Dougan B, Jeong J, Kennedy KP, Allen TA. Brain Sciences. 2017;7(11):143. doi:10.3390/brainsci7110143
- Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: a meta-analysis of family high-risk studies. Rasic D, Hajek T, Alda M, Uher R. Schizophrenia Bulletin. 2014;40(1):28-38. doi:10.1093/schbul/sbt114
- Effects of stress throughout the lifespan on the brain, behavior and cognition. Lupien SJ, McEwen BS, Gunnar MR, Heim C. Nature Reviews Neuroscience. 2009;10(6):434-445. doi:10.1038/nrn2639
- Effects of nurse home visiting on maternal and child functioning: age-9 follow-up of a randomized trial. Olds DL et al. Pediatrics. 2007;120(4):e832-e845. doi:10.1542/peds.2006-2111