A 2026 Nature Neuroscience study found that awake mouse brain motion was driven mainly by locomotion-linked abdominal muscle activity, not by respiration or cardiac rhythm; the researchers mapped displacement vectors at 134 cortical sites in 24 mice and modeled how that motion could push fluid out of brain tissue.1 The result sharpens the body-brain mechanics question, but it does not prove that exercise flushes waste from the human brain.
Research Highlights
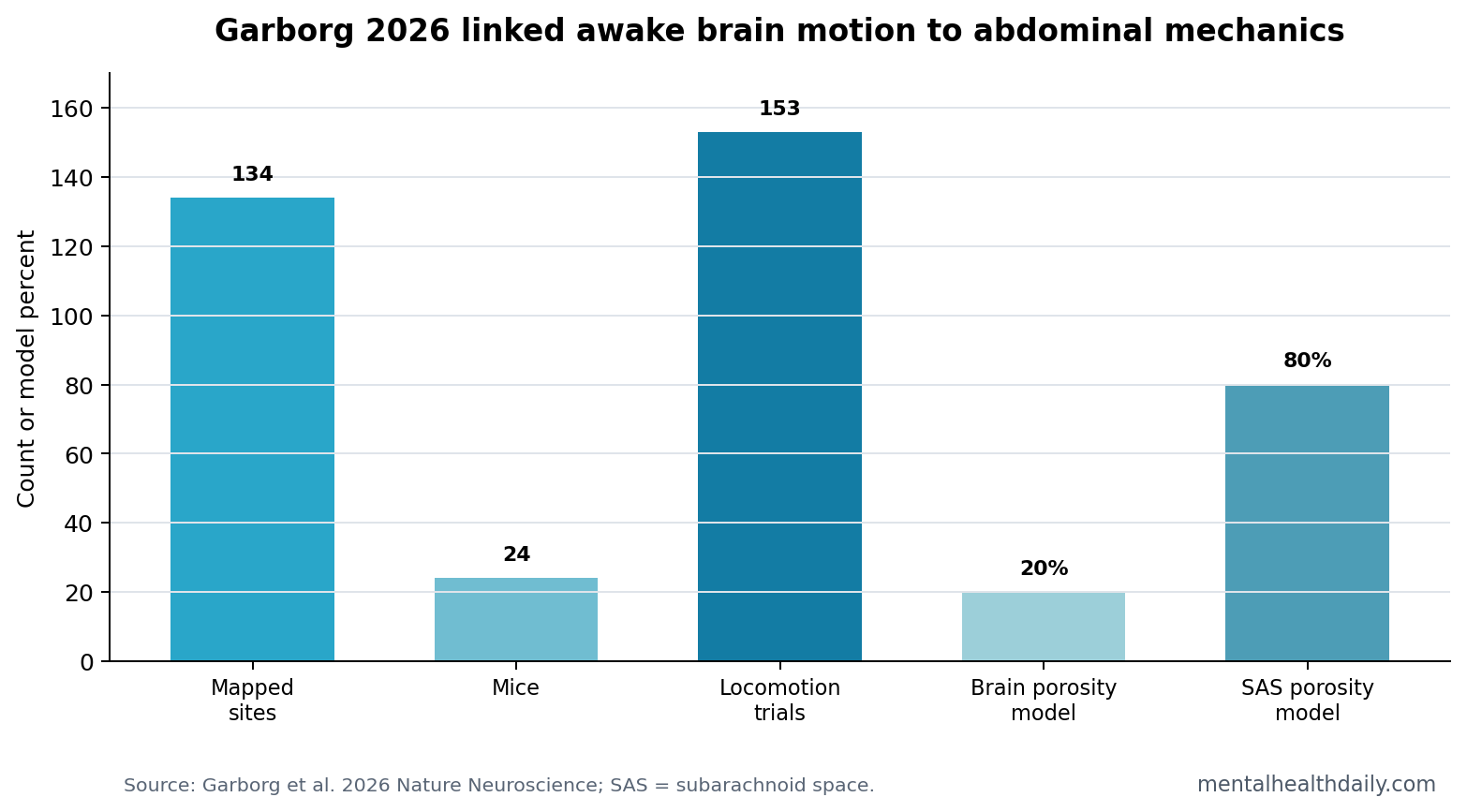
- 134 cortical sites were mapped: displacement vectors from 24 mice showed a consistent rostral-lateral brain-motion pattern during locomotion.1
- 153 locomotion trials supported timing: triggered averages showed brain movement tightly linked to movement onset and offset.1
- Heartbeat was not the main driver: awake brain motion was mainly low frequency, below 0.1 Hz, and did not align with respiration or heartrate frequencies.1
- Abdominal pressure reproduced the effect: externally applied abdominal pressure moved the brain rapidly in lightly anesthetized mice.1
- Fluid-flow claims remain modeled: simulations used 20% brain porosity and suggested outward interstitial-fluid movement, opposite the direction often discussed during sleep.
Brain motion means physical displacement of brain tissue relative to the skull. In anesthetized animals and supine humans, small motion is often linked to heartbeat and breathing. Garborg et al. asked what drives motion in awake mice, where locomotion creates stronger whole-body forces.
The glymphatic system is a proposed brain-fluid clearance pathway involving cerebrospinal fluid, interstitial fluid, and perivascular spaces. It is easy to overstate. The 2026 paper studied mechanical motion and modeled flow; it did not measure cognitive outcomes or human waste clearance.
Awake Brain Motion Tracked Locomotion More Than Respiration
The researchers used high-speed multiplane two-photon microscopy to visualize dorsal cortical motion in awake head-fixed mice. Brain displacement was primarily rostral and lateral. Across 134 imaging sites in 24 mice, the direction of movement was consistent enough to argue against random tissue wobble.1
Power-spectrum analysis showed that awake motion was dominated by low frequencies below 0.1 Hz. The paper reported no appreciable motion at respiration or heartrate frequencies in awake mice, despite prior work showing heartbeat-linked pulsations under other conditions.
Mechanical interpretation: locomotion changes abdominal pressure, venous pressure, and cerebrospinal-fluid dynamics. The brain is mechanically protected by the skull, but it is not mechanically isolated from the rest of the body.
Abdominal Muscle Activity Was the Candidate Driver
Garborg et al. linked brain movement to abdominal electromyography, a measure of muscle activity. EMG power rose before locomotion and correlated with brain motion. The researchers then applied controlled pressure to the abdomen of lightly anesthetized mice and reproduced rapid brain displacement.1
- Locomotion link: moving mice showed rostral-lateral brain displacement.
- Abdominal link: abdominal muscle activity tracked the motion signal.
- Pressure test: external abdominal compression could shift the brain, supporting a mechanical coupling route.
Modeled Fluid Flow Pointed Outward During Awake Motion
The simulation part used a simplified poroelastic model. Poroelastic means a deformable solid material saturated with fluid, which is a reasonable abstraction for brain tissue when the question is how displacement may move interstitial fluid.
The model set brain parenchyma porosity at 20% and surrounding fluid-rich compartments at 80%. Under motion conditions chosen to match empirical brain displacement and intracranial-pressure changes, simulations suggested interstitial fluid could move out of the brain into the subarachnoid space. The authors noted that this direction was opposite the glymphatic flow emphasized during sleep.1,2
Clinical Claims Need a Much Higher Bar
Evidence-strength note: this was a mouse mechanics study with modeling. It can support a body-brain mechanical coupling mechanism. It cannot show that walking, abdominal breathing, core exercise, or any consumer intervention clears human brain waste, prevents dementia, or improves cognition.
The most useful clinical implication is restraint. Movement probably changes brain mechanics. Sleep probably changes brain-fluid dynamics in a different way. Translating either into treatment requires direct human measurement, disease endpoints, and controls that separate physiology from wellness-language overreach.
Awake Motion and Sleep Flow May Be Different Physiological Modes
One reason the paper is interesting is that it pushes against a single “more flow is always better” story. Sleep-associated glymphatic work emphasizes fluid entry into brain tissue and metabolite clearance during quiescence.2 Garborg et al. modeled awake movement as pushing fluid out of brain tissue into the subarachnoid space.1
Those directions can both be physiologically useful. A living brain needs pressure regulation, waste movement, volume control, vascular pulsation, and protection from excessive tissue strain. Sleep and locomotion place different demands on those systems.
Sleep state: quiescence, altered neuromodulatory tone, and vascular dynamics may favor fluid entry and exchange.
Awake locomotion: abdominal pressure and body movement may favor displacement and outward fluid shifts. That could help explain why movement-related brain motion is robust while deep sleep remains special for clearance models.
The Vertebral Venous Plexus Is the Plausible Mechanical Route
The paper’s proposed pathway runs through abdominal pressure, the vertebral venous plexus, cerebrospinal-fluid displacement, and brain motion. The vertebral venous plexus is a valveless venous network linking the abdominal and spinal compartments. Because it lacks valves, pressure changes can transmit in ways that resemble a hydraulic system.
That anatomy makes the abdomen more relevant than it first sounds. The brain sits inside the skull, but the craniospinal fluid system and venous system are continuous with the spine and body. A pressure change in the abdomen can therefore become a pressure change in the central nervous system.
External abdominal compression in lightly anesthetized mice strengthened the causal story. Locomotion correlation alone could be indirect; pressure applied to the abdomen reproducing brain displacement makes the mechanical link more credible.
The proposed route is mechanical rather than mystical. Abdominal contraction can change venous pressure, spinal pressure transmission, and intracranial pressure. Those pressure changes can move brain tissue slightly and alter local fluid gradients. That does not require the abdomen to “control” the brain; it requires the craniospinal compartment to behave like a connected pressure system.
Human Translation Needs Direct Measurement
A human version of this question would need imaging or sensor methods that can separate cardiac pulsation, respiration, posture, gait, abdominal pressure, venous pressure, and cerebrospinal-fluid movement. That is difficult because walking humans move their heads, necks, blood pressure, breathing, and muscles at the same time.
Useful human endpoints would include phase-contrast MRI of CSF motion, high-resolution brain displacement imaging, wearable measures of gait and abdominal muscle activity, and sleep-wake comparisons in the same participants. Clinical endpoints such as cognitive performance or dementia risk would come much later.
The mouse data also make timing important. Garborg et al. were studying awake movement-linked displacement, not the same physiological state as sleeping glymphatic clearance experiments.1,2 If a human study measured only resting supine MRI, it might miss the abdominal-pressure component. If it measured only walking physiology, it might miss sleep-state clearance dynamics.
A serious translation study would therefore compare states within the same person: quiet wakefulness, paced breathing, standing, walking, and sleep or sleep-like rest. The question is not whether 1 pump explains all brain-fluid movement. The better question is which mechanical driver dominates under which body state.
Posture and Anesthesia Complicate the Old Assumptions
Garborg et al. also help explain why older observations can conflict. Under anesthesia or in supine humans, respiration and cardiac pulsation can dominate measured brain motion. In awake behaving mice, locomotion and abdominal muscle activity produced a different mechanical regime. The same brain can therefore have different dominant motion drivers depending on state.
State dependence: anesthesia changes muscle tone, breathing pattern, vascular regulation, arousal, and movement. Sleep changes neuromodulatory tone and fluid spaces. Awake locomotion changes abdominal pressure and body mechanics. A single model of brain motion across all states is too simple for the physiology.
That is why the paper should be read as a state-specific mechanism. It identifies a strong awake movement-linked driver in mice, then uses modeling to explore fluid consequences. It does not erase heartbeat, respiration, or sleep-related mechanisms in other settings.
State-specific framing: a mouse walking on a head-fixed setup, a sleeping mouse, an anesthetized mouse, and a walking human are different mechanical systems.
The shared lesson is that brain-fluid physiology is coupled to body state. The next question is which state, which pathway, which direction of flow, and which measurable outcome.
For now, the study’s strongest contribution is anatomical and mechanical: abdominal pressure can move the awake mouse brain through a plausible craniospinal coupling pathway. Clinical claims should wait for human measurement.
Questions About Brain Motion and Fluid Flow
Did the study show that exercise cleans the brain?
No. It showed that awake mouse brain motion was mechanically coupled to locomotion and abdominal activity, with simulations suggesting outward fluid movement.
Why is the abdomen involved?
Abdominal muscle contraction can raise intra-abdominal pressure. The study argues that pressure can communicate mechanically through venous and cerebrospinal-fluid pathways to the brain.
Is this the same as sleep glymphatic flow?
No. The modeled awake-motion flow was described as opposite the direction of sleep-associated glymphatic flow, which is why the result should not be simplified into one clearance story.
References
- Garborg CS, Ghitti B, Zhang Q, et al. Brain motion is driven by mechanical coupling with the abdomen. Nature Neuroscience. 2026. doi:10.1038/s41593-026-02279-z
- Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013. doi:10.1126/science.1241224
- Mestre H, Tithof J, Du T, et al. Flow of cerebrospinal fluid is driven by arterial pulsations and is reduced in hypertension. Nature Communications. 2018. doi:10.1038/s41467-018-07318-3
- Kedarasetti RT, Drew PJ, Costanzo F. Arterial pulsations drive oscillatory flow of CSF but not directional pumping. PubMed