
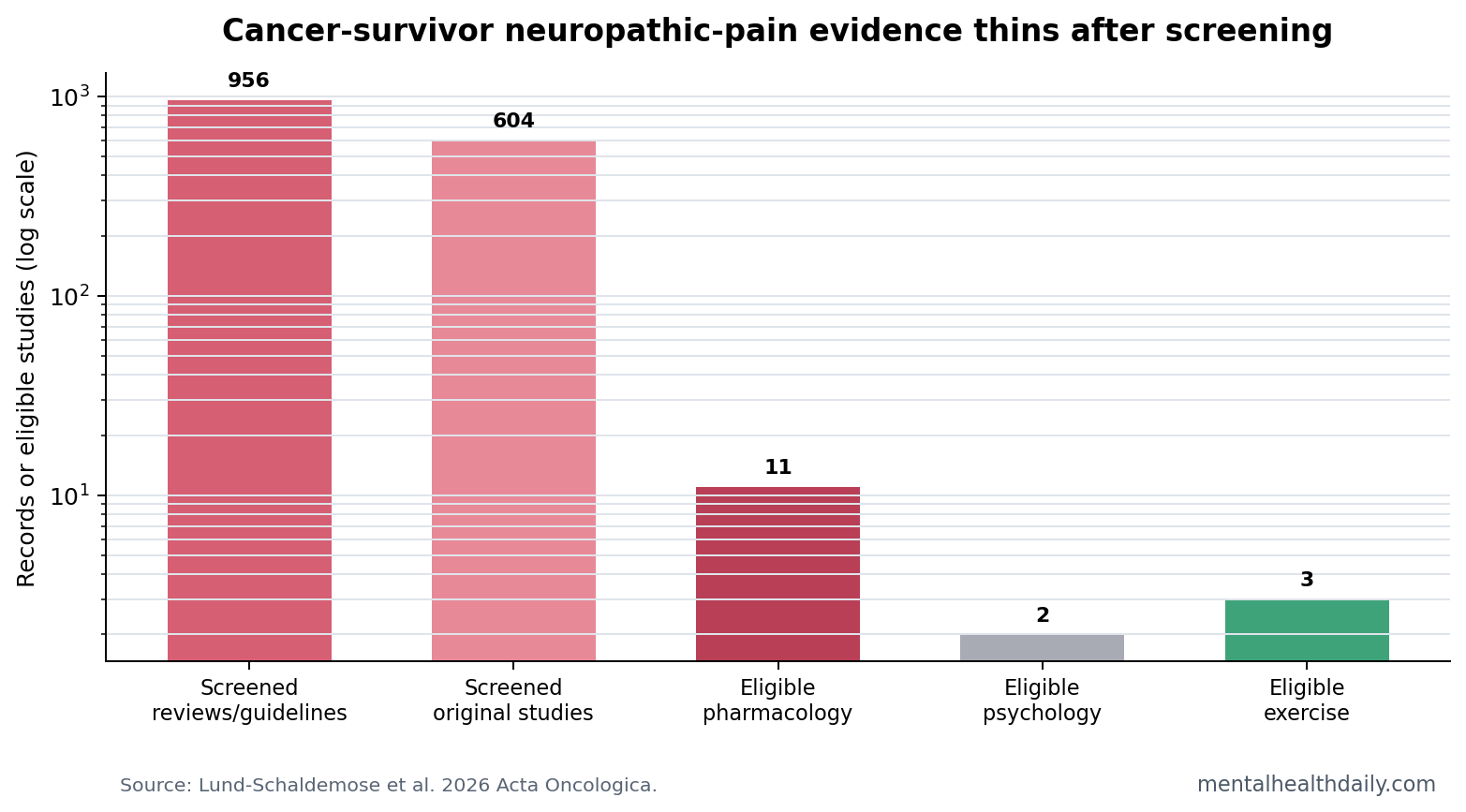
A 2026 scoping review screened 956 systematic reviews/guidelines and 604 original studies on cancer-survivor neuropathic pain, but only 11 pharmacological, 2 psychological, and 3 exercise studies were eligible.1 The practical signal is narrow: duloxetine and some exercise programs have the clearest support, while psychological and interdisciplinary evidence is still too thin for confident treatment ranking.
Research Highlights
- 1,560 records narrowed to 16 studies: the review found 11 pharmacological, 2 psychological, and 3 exercise studies eligible after screening.1
- Duloxetine had the clearest drug signal: the review found benefit for painful chemotherapy-induced peripheral neuropathy, consistent with prior randomized evidence.1,2
- Gabapentin plus morphine helped one subgroup: combined gabapentin and morphine reduced neuropathic pain more than morphine alone after radiotherapy or surgery-related pain.1
- Mindfulness-based CBT stayed uncertain: 2 open RCTs were identified, but effects did not hold after correction for multiple comparisons.1
- Exercise looked promising: one 9-week program reduced Douleur Neuropathique scores from 5.96 to 2.31, p = 0.001, in a small pilot.1
Neuropathic pain is pain caused by injury or dysfunction in the somatosensory nervous system. In cancer survivorship, it can follow chemotherapy, surgery, or radiotherapy and can persist after the original cancer is no longer active.
Chemotherapy-induced peripheral neuropathy (CIPN) is one of the common survivor problems: numbness, burning, tingling, shooting pain, balance problems, or sensory loss after neurotoxic chemotherapy. The treatment question includes pain relief, sleep, walking, work, daily activity, and medication harms that can stack onto cancer-treatment late effects.
Most Candidate Evidence Was Not Survivor-Specific
Lund-Schaldemose et al. searched PubMed, PsycInfo, and EMBASE for studies from January 2004 to January 2026. The target population was cancer survivors who had completed primary treatment and had no active disease. Neuropathic pain had to involve at least moderate pain intensity, neuropathy symptoms, or diagnosis by an experienced neurologist.1
The screening funnel is the main result. A broad literature search produced 956 systematic reviews/guidelines and 604 original studies, but only 16 original studies met survivor-specific eligibility criteria.
Duloxetine Remains the Medication With the Strongest Signal
Duloxetine is a serotonin-norepinephrine reuptake inhibitor, a drug class that can reduce pain signaling as well as treat depression and anxiety. In neuropathic pain, norepinephrine-mediated descending pain inhibition is part of the rationale.
The 2026 review found duloxetine effective for painful CIPN. That aligns with Smith et al.’s randomized trial, which remains a central reason guidelines often identify duloxetine as the clearest medication option for painful CIPN.2
Other drug signals were more situational. An open comparative RCT reported pain-score reductions with both duloxetine and pregabalin, from 7.04 to 4.04 for duloxetine and 6.89 to 4.91 for pregabalin, both p < 0.001, but pregabalin had more adverse effects.1
Psychological Treatment Evidence Was Thin
The review found 2 open RCTs of group-based mindfulness-based cognitive behavioral therapy in breast-cancer survivors. One analysis reported a small neuropathic-pain reduction, Cohen’s d = 0.24, but the abstract-level conclusion was that mindfulness-based CBT showed no effect after correction for multiple comparisons.1
Interpretation: psychological care may still help coping, distress, sleep, fear of movement, or pain interference. The source review does not show a strong survivor-specific neuropathic-pain reduction signal yet.
Exercise Looks Promising but Underbuilt
The exercise evidence came from 1 open RCT and 2 cohort/pilot studies. In a 26-person pilot, pain neuroscience education plus combined home and supervised resistance/aerobic exercise 3 times weekly for 9 weeks reduced Douleur Neuropathique questionnaire scores from 5.96 ± 1.83 to 2.31 ± 1.01, p = 0.001.1
A separate 12-week cardiovascular and upper-body strength program reported reduction in a McGill sensory pain rating index from 25% to 7% after 6 months, p < 0.05, though overall pain did not separate cleanly from control.1
Clinical boundary: exercise should be individualized around balance, numbness, fatigue, lymphedema risk, anemia, cardiopulmonary reserve, and fall risk. The evidence supports supervised, adapted movement as a plausible treatment component, not a generic instruction to push through neuropathic pain.
Scoping Review Limits
Evidence-strength note: a scoping review maps the evidence landscape; it does not pool effect sizes the way a meta-analysis does. Most included studies involved breast-cancer survivors, which limits extrapolation to neuropathy after other cancers and treatments.
The best read is therefore ranked but cautious. Duloxetine has the strongest medication support. Exercise has encouraging survivor-specific signals but small-study limitations. Mindfulness-based CBT may help broader coping outcomes, but pain-specific evidence remains uncertain.
Treatment Choice Should Start With Pain Mechanism and Survivor Constraints
Cancer-survivor neuropathic pain is not one entity. Chemotherapy-induced peripheral neuropathy, post-mastectomy neuropathic pain, radiation-related plexopathy, and surgery-related nerve injury can feel similar while arising from different tissue histories. A medication or exercise plan that fits one mechanism may be poorly matched to another.
CIPN pattern: distal numbness, burning, tingling, and sensory loss after neurotoxic chemotherapy often affects both feet or hands. Duloxetine has the clearest evidence signal here, especially when pain rather than numbness is the dominant complaint.2
Postsurgical pattern: localized burning, shooting pain, scar sensitivity, or movement-provoked nerve pain after mastectomy or other surgery may need regional assessment, physical therapy, desensitization, and sometimes medication.
Radiotherapy pattern: delayed nerve injury after radiotherapy can involve progressive sensory or motor features. That pattern needs careful medical review because structural complications, recurrence, or plexopathy may change management.
Why Exercise Belongs in the Discussion
Exercise is sometimes treated as a general survivorship recommendation, but the neuropathic-pain question is more specific. Movement may improve strength, balance, circulation, sleep, fear of movement, and pain-related disability. For peripheral neuropathy, those functional outcomes can matter even when numbness itself persists.
The 9-week pilot combining pain neuroscience education with resistance and aerobic exercise is small, but the change from 5.96 to 2.31 on the Douleur Neuropathique questionnaire is large enough to justify better trials.1 The key is supervision and adaptation. A survivor with foot numbness, fall risk, fatigue, or cardiotoxicity history needs a different plan from a survivor with isolated hand tingling.
Psychological Care May Target Interference More Than Nerve Pain
The mindfulness-based CBT findings should be read carefully. Lack of corrected pain reduction does not erase possible value for distress, sleep, fear, coping, attention to symptoms, or pain interference. It means pain-intensity claims need stronger evidence.
That distinction can help clinics avoid overpromising. Psychological care may be appropriate when neuropathic pain is entangled with anxiety, insomnia, catastrophizing, trauma from treatment, or loss of function. The current survivor-specific evidence does not make it a clear analgesic substitute for duloxetine or a graded physical program.
Interdisciplinary Care Is Plausible but Understudied
The review’s conclusion pointed toward interdisciplinary treatment. That is clinically sensible because neuropathic pain after cancer treatment often crosses oncology, neurology, rehabilitation, psychiatry, primary care, and pain medicine. The evidence base, however, has not caught up with that reality.
A strong future trial would compare duloxetine, adapted exercise, psychological pain skills, and combined care using outcomes survivors care about: pain intensity, numbness, falls, sleep, walking distance, return to work, medication adverse effects, and quality of life.
Adverse Effects Are Part of the Evidence Hierarchy
Neuropathic-pain drugs are rarely judged only by pain-score change. Duloxetine can cause nausea, sweating, insomnia, somnolence, blood-pressure effects, sexual side effects, and withdrawal symptoms if stopped abruptly. Pregabalin and gabapentin can cause dizziness, sedation, edema, weight gain, and fall risk. Opioids add constipation, sedation, endocrine effects, tolerance, dependence, and overdose risk.
Those tradeoffs are especially important in cancer survivorship because many patients already carry fatigue, sleep disruption, balance problems, polypharmacy, and anxiety about recurrence. A modest pain reduction may be worthwhile for one survivor and unacceptable for another depending on function and adverse effects.
Practical ranking: the best first option fits pain mechanism, expected benefit, tolerability, and the survivor’s functional goals.
That ranking also explains why the evidence gap is not academic. A survivor with numb feet, poor balance, and chemotherapy-related fatigue may value fall prevention and walking tolerance as much as a 1-point pain-score change. Another survivor with burning allodynia may accept medication adverse effects for a larger pain reduction.
Trials that only report average pain intensity miss those tradeoffs. Future survivor-specific studies need responder analyses, adverse-event reporting, function, sleep, and quality-of-life endpoints so treatment choice can move beyond borrowing from general neuropathic-pain populations.
Questions About Cancer Survivor Neuropathic Pain
Is duloxetine useful only if the survivor is depressed?
No. Duloxetine can reduce neuropathic pain through pain-modulation pathways even when depression is not the treatment target.
Does gabapentin work for chemotherapy-induced neuropathy?
The review did not identify gabapentin as the strongest CIPN signal. One benefit involved gabapentin plus morphine compared with morphine alone in radiation- or surgery-related neuropathic pain.
Should exercise be supervised?
Often yes, at least initially. Neuropathy can affect sensation and balance, so resistance and aerobic work should be adapted to fall risk, pain flares, fatigue, and cancer-treatment late effects.
Why separate cancer survivors from general neuropathic-pain patients?
Cancer survivors often have treatment-specific nerve injury, fatigue, sleep disruption, recurrence anxiety, and polypharmacy. Borrowed neuropathic-pain evidence can help, but survivor-specific trials are needed because tolerability and functional priorities may differ.
References
- Lund-Schaldemose E, et al. Treatment of neuropathic pain in cancer survivors: a scoping review. Acta Oncologica. 2026. doi:10.2340/ao.v65.45347
- Smith EML, Pang H, Cirrincione C, et al. Effect of duloxetine on pain, function, and quality of life among patients with chemotherapy-induced painful peripheral neuropathy. JAMA. 2013. doi:10.1001/jama.2013.2813
- Loprinzi CL, Lacchetti C, Bleeker J, et al. Prevention and management of chemotherapy-induced peripheral neuropathy in survivors of adult cancers. PubMed
- Lores-Peniche J, et al. Pain neuroscience education and exercise for chemotherapy-induced peripheral neuropathy. PubMed