A 2026 iScience paper used simultaneous sleep EEG-fMRI from 2 healthy cohorts totaling 24 people to build slow-wave-related BOLD reference maps and propose SloCAD, a framework for measuring how an individual’s slow-wave brain activity deviates from a healthy reference pattern.1
Research Highlights
- The proof of concept used 24 healthy participants: 2 independent cohorts (N1 = 11; N2 = 13) produced substantially overlapping slow-wave BOLD reference maps.1
- Slow waves anchored the fMRI analysis: EEG-detected slow wave events were used as timing markers for BOLD responses in cingulate cortex, thalamus, hippocampus, and cerebellum.1
- Synchronization changed the map: high-synchronization slow waves recruited broader cortical and subcortical networks than low-synchronization slow waves.1
- SloCAD is a deviation metric: the proposed framework subtracts an individual’s slow-wave BOLD map from a reference map to estimate network deviation.1
- Clinical validation remains at 0 patient cohorts: the paper explicitly describes SloCAD as a proof of concept, not a diagnostic biomarker.1
Slow wave events are large, low-frequency brain activity patterns that occur during non-rapid eye movement sleep. They help organize cortical state changes and are tied to memory, synaptic regulation, aging, and several neuropsychiatric conditions.2,3
EEG-fMRI combines electroencephalography, which records fast electrical brain signals from the scalp, with functional magnetic resonance imaging, which estimates slower blood-oxygen-level-dependent activity across brain regions. The appeal is timing plus location: EEG marks the event, fMRI maps the network response.
24 Healthy Sleep Scans Built the Reference Maps
Ilhan-Bayrakci et al. analyzed simultaneous sleep EEG-fMRI from 2 healthy cohorts. The first had 11 people and the second had 13. Despite small samples and design differences, the resulting reference masks overlapped enough for the researchers to propose a larger normative mapping strategy.1
The reference maps consistently involved the cingulate cortex, thalamus, hippocampus, and cerebellum. Those regions are biologically plausible because slow-wave sleep interacts with memory systems, arousal systems, and large-scale network regulation beyond the cortical surface rhythm alone.
Synchronization Efficiency Split Slow Waves Into Different Network States
Synchronization efficiency describes how coherently a slow wave spreads across the brain. In this paper, high-synchronization slow waves recruited widespread cortical and subcortical patterns, while low-synchronization slow waves leaned more toward posterior cortical regions.1
That distinction is more than a technical tweak. If all slow waves are pooled together, biologically different events may blur into a less sensitive average. Sorting slow waves by synchronization may make future maps better at detecting subtle network dysfunction.
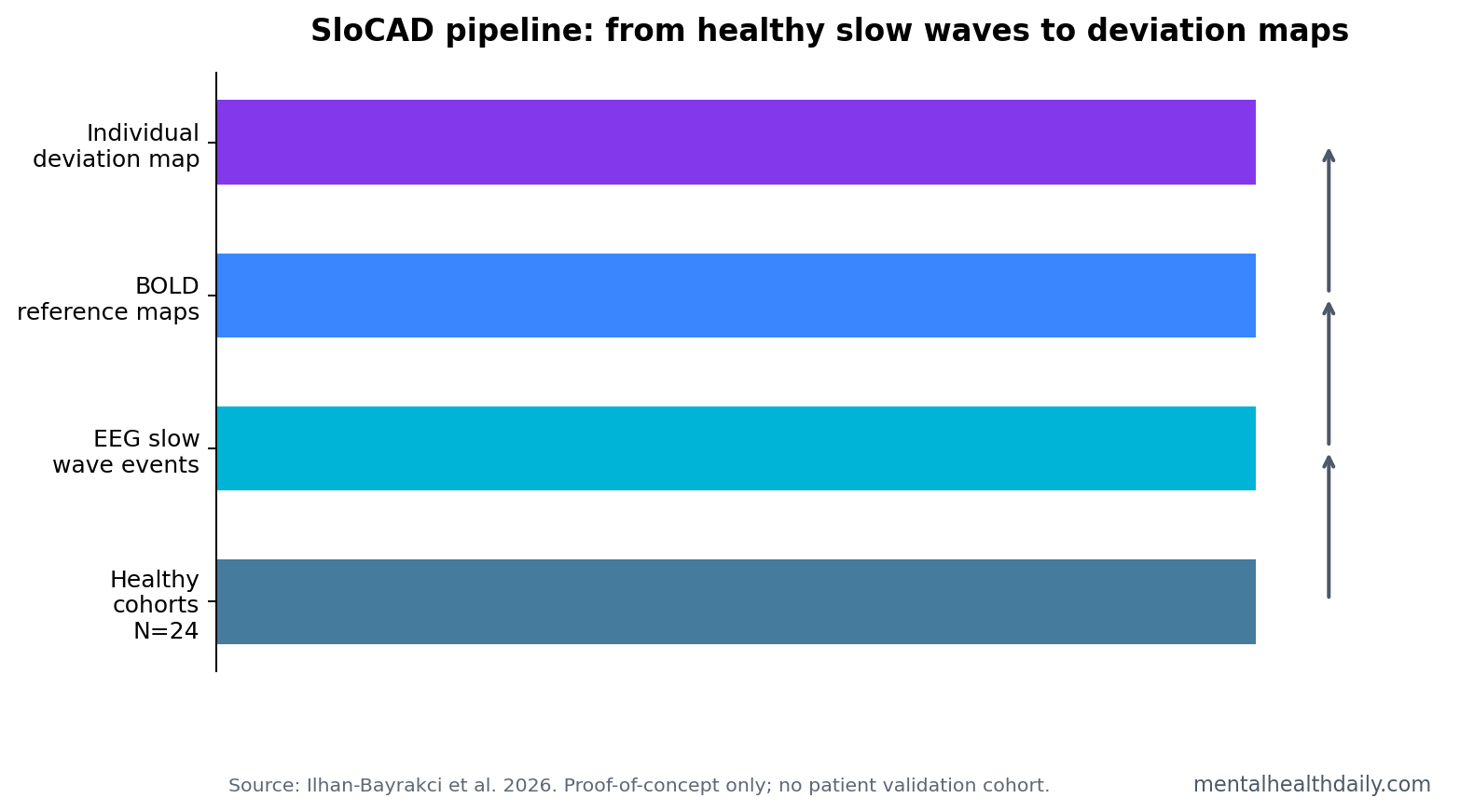
SloCAD Measures Deviation From a Healthy Slow-Wave Map
SloCAD stands for slow wave canonical activity deviation. The proposed workflow is straightforward in concept:
- Build age-matched healthy reference maps from sleep EEG-fMRI.
- Record the same sleep EEG-fMRI protocol in an at-risk or patient group.
- Generate each person’s slow-wave BOLD activation map.
- Subtract that individual map from the healthy reference map.
- Convert the difference into a deviation metric.
The clinical hope is that deviation from a healthy slow-wave network pattern could flag early network dysfunction before conventional structural changes are obvious. The current paper does not prove that hope; it specifies a path for testing it.
Sleep Network Mapping Is Relevant to Dementia, Parkinson’s, and Schizophrenia
The paper notes that slow-wave activity alterations have been reported in Alzheimer’s disease, Parkinson’s disease, and schizophrenia, while simultaneous sleep EEG-fMRI patient datasets remain scarce.1 That gap matters because ordinary EEG can show slow-wave changes, but it cannot localize the full BOLD network response with the same spatial detail.
Sleep and memory consolidation are already linked in neuroscience. Diekelmann and Born described sleep as an active state for memory reorganization and synaptic regulation.4 SloCAD pushes that logic toward individualized network mapping.
Evidence Strength and Limits
Evidence-strength note: SloCAD is a methodological proof of concept. It can show that healthy sleep EEG-fMRI maps can be created and that synchronization-informed slow-wave subtypes may be useful. It cannot diagnose disease, predict conversion, stage neurodegeneration, or guide treatment.
Large multisite datasets are the next requirement. Sleep EEG-fMRI is expensive, technically demanding, and sensitive to acquisition differences. A clinical biomarker would need standardized protocols, age-stratified norms, patient cohorts, test-retest reliability, and prediction against real clinical outcomes.
The Measurement Target Is Network Health, Not Sleep Quality Alone
SloCAD is not mainly a sleep-quality metric. Its target is network organization during a defined neurophysiological event. A person could sleep for the same duration as a control participant while showing a different slow-wave BOLD response. That distinction is why the method is interesting for early network dysfunction.
Mechanistic implication: slow waves give the analysis a biological timestamp. Instead of asking whether resting networks look different on average, SloCAD asks how the brain responds when a slow wave occurs and whether that response matches a healthy reference pattern. That could be more sensitive than ordinary resting-state averages if disease alters event-linked coordination before gross structure changes.
Clinical Translation Requires Norms Before Labels
The first major translation step is not patient classification. It is normative mapping. Researchers would need enough healthy people across age bands to define expected slow-wave BOLD patterns and normal variation. Only then can an individual deviation score be interpreted as unusually large rather than ordinary biological diversity.
Patient validation would then need prespecified outcomes: cognitive decline, seizure localization, psychosis-risk transition, insomnia severity, or neurodegenerative progression. Without those anchors, a deviation map is only a difference map. It becomes a biomarker only when it predicts something clinically meaningful.
Age Matching Is Central Because Slow Waves Change Across Life
The paper emphasizes age-matched reference cohorts because slow-wave activity changes strongly across development and aging. A deviation score is uninterpretable if it compares an older adult to a young-adult reference map without accounting for normal age-related change.
This is especially important for neurodegenerative disease. Alzheimer’s and Parkinson’s disease usually emerge in age ranges where sleep architecture is already shifting. A useful SloCAD atlas would need to distinguish disease-linked deviation from expected aging-linked slow-wave change.
Standardization Is the Real Bottleneck
Sleep EEG-fMRI is not like drawing blood. Participants must sleep in a scanner, EEG artifacts must be handled, fMRI preprocessing must be consistent, and slow-wave detection rules must generalize across sites. Small differences in preprocessing could change the reference map and make deviation scores hard to compare.
That is why multicenter replication matters more than a larger single-site proof. A biomarker intended to detect early network dysfunction has to survive ordinary site differences: scanner model, head coil, sleep environment, EEG setup, noise correction, and scoring rules.
Normative databases would also need transparent exclusion rules. Sleep apnea, restless legs symptoms, heavy alcohol use, shift work, sedative exposure, and untreated insomnia could all change slow-wave timing or BOLD coupling without representing neurodegenerative disease. If those variables are not measured and modeled, a deviation score could become a proxy for sleep-disruption burden rather than a disease-specific network marker.
A useful SloCAD report would therefore need uncertainty intervals, age-band context, sleep-stage context, and medication notes. A single abnormal-looking map without those guardrails could invite overdiagnosis.
Longitudinal anchoring would make the deviation score easier to interpret.
The Best Near-Term Use Is Research Stratification
The first practical use of SloCAD may be trial enrichment or subgroup discovery rather than clinical diagnosis. Researchers could ask whether people with larger slow-wave network deviation have faster cognitive decline, worse insomnia symptoms, greater seizure burden, or different treatment response. Those are testable research questions with clearer endpoints than a broad “brain health” label.
Deviation Scores Need Test-Retest Reliability
A clinical biomarker must be stable enough to interpret. If the same person has a very different SloCAD score on 2 nights without a meaningful clinical change, the metric would be difficult to use. Test-retest reliability is therefore a basic requirement before disease prediction.
Reliability testing should include ordinary sources of variation: sleep depth, first-night effects, medication use, caffeine, sleep deprivation, scanner noise, and motion. A deviation metric that survives those conditions would be much more credible as a research stratification tool.
Medication and Sleep Architecture Could Confound Future Patient Maps
Patient cohorts will also bring medication confounding. Antidepressants, antipsychotics, benzodiazepines, stimulants, dopaminergic drugs, and sleep medications can alter sleep architecture, arousal, movement, or EEG rhythms. A disease-linked SloCAD deviation could be exaggerated, masked, or mimicked by treatment exposure if medication status is not modeled carefully.
That does not make the framework unusable. It means early studies should record medication dose, sleep stage distribution, apnea risk, insomnia symptoms, and prior-night sleep. A slow-wave biomarker that ignores those variables would be vulnerable to false clinical interpretation.
Questions About SloCAD
Is SloCAD a diagnostic test?
No. The 2026 paper proposed a framework and built healthy reference maps. It did not validate SloCAD as a diagnostic test in any patient cohort.
Why use sleep slow waves instead of resting-state fMRI alone?
Slow waves provide event timing from EEG. That lets researchers ask how the brain’s BOLD network responds to a specific sleep event instead of averaging spontaneous activity without a neurophysiological anchor.
Which disorders could be tested next?
Neurodegenerative disease, schizophrenia, epilepsy, and insomnia are plausible targets because prior work links them to altered sleep physiology or network function. Each still needs direct validation.
References
- Ilhan-Bayrakci M, et al. Slow wave canonical activity deviation concept: Toward a slow wave-based EEG-fMRI reference map. iScience. 2026. https://doi.org/10.1016/j.isci.2026.115455
- Steriade M, Nunez A, Amzica F. A novel slow oscillation of neocortical neurons in vivo: depolarizing and hyperpolarizing components. Science. 1993. https://doi.org/10.1126/science.8235585
- Tononi G, Cirelli C. Sleep and the Price of Plasticity: From Synaptic and Cellular Homeostasis to Memory Consolidation and Integration. Neuron. 2014. https://doi.org/10.1016/j.neuron.2014.01.002
- Diekelmann S, Born J. The memory function of sleep. Nature Reviews Neuroscience. 2010. https://doi.org/10.1038/nrn2762