
Australian coronial data show that fatal poisonings involving new psychoactive stimulants and hallucinogens were rarely single-drug events. In 70 toxicology-confirmed deaths from 2007 through 2025, 92.9% involved other psychoactive drugs and 75.7% involved multiple stimulants or hallucinogens.
Research Highlights
- Fatal cases were usually polysubstance cases: 65 of 70 deaths (92.9%) had psychoactive drugs beyond the new stimulant or hallucinogen, and 53 cases (75.7%) had multiple stimulants or hallucinogens in blood toxicology.
- Cathinones led the overall toxicology profile: cathinones appeared in 34 cases (48.6%), followed by phenethylamines in 27 (38.6%), tryptamines in 13 (18.6%), and piperazines in 3 (4.3%).
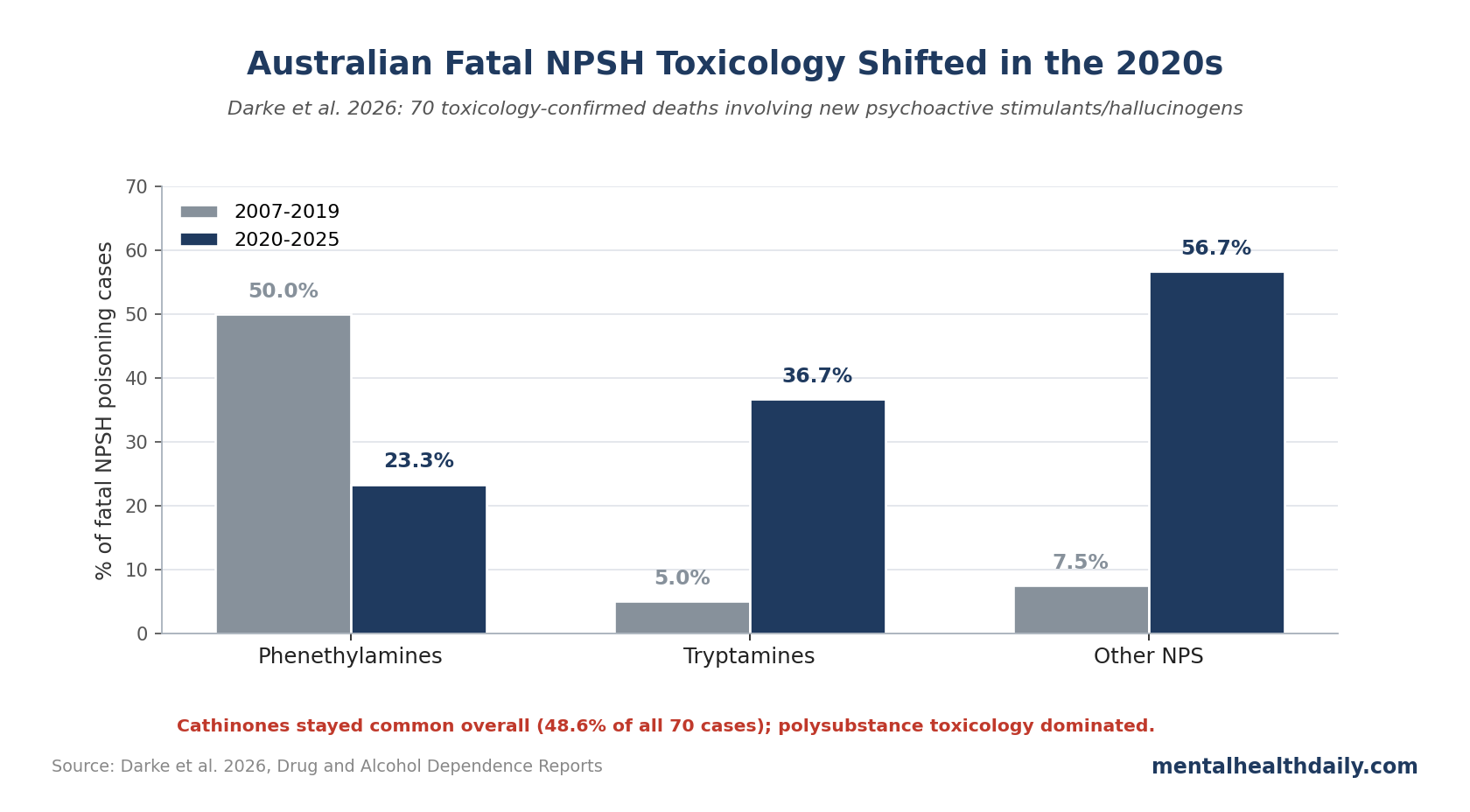
- 2020s cases shifted: later cases were more likely to involve tryptamines (36.7% vs. 5.0%) and other novel psychoactive substances (56.7% vs. 7.5%), while phenethylamines became less common (23.3% vs. 50.0%).
- Many people did not know what they had taken: in 16 cases (22.9%), witnesses reported that the person thought they were using MDMA, methamphetamine, or LSD rather than a new psychoactive stimulant or hallucinogen.
- Overdose signs were concrete: intense agitation and sudden collapse each appeared in 16 cases, followed by hyperthermia in 14, seizure in 13, and delirium in 12.
Darke et al. analyzed closed Australian coronial cases where death was attributed to drug toxicity and blood toxicology confirmed a new psychoactive stimulant or hallucinogen (NPSH).1 The study is not a national prevalence survey. It is a forensic case series of known fatal poisonings.
70 Fatal Poisonings, Mostly Private and Unintentional
Researchers identified 70 fatal NPSH-related poisonings, with the first occurring in 2007. Of those, 30 occurred in the 2020s. Annual counts ranged from 0 in 2008 to 9 in both 2014 and 2021, with a median of 4.5 deaths per year.
Case profile was concentrated but not narrow:
- Age: mean 32.8 years, standard deviation 10.8, range 18–62.
- Sex: 58 cases (82.9%) were male and 12 (17.1%) were female.
- Setting: 57 deaths (81.4%) occurred in a private setting, and fewer than 5 occurred at a music festival.
- Intent: 65 deaths (92.9%) were coded unintentional, 5 (7.1%) undetermined, and 0 intentional self-poisoning.
- Medical response: 36 cases (51.4%) involved ambulance or doctor intervention before death.
That profile cuts against the lazy “festival drug death” frame. Most deaths happened in houses or similar private settings, often with other people nearby, and many were not recognized early enough as rapidly dangerous stimulant or hallucinogen toxicity.
65 of 70 Fatal Cases Included Other Psychoactive Drugs
Only 11 deaths were attributed solely to NPSH toxicity. Another 59 involved multiple-drug toxicity. Other psychoactive drugs appeared in 65 cases (92.9%), led by psychostimulants in 48 cases (68.6%), hypnosedatives in 28 (40.0%), opioids in 25 (35.7%), alcohol in 20 (28.6%), cannabis in 13 (18.6%), antidepressants in 11 (15.7%), and antipsychotics in 11 (15.7%).
Blood toxicology also showed that 18 cases (25.7%) involved multiple NPSH. Those combinations most often involved multiple phenethylamines (9 cases) or multiple cathinones (6 cases). Five cases had more than one NPSH class detected.
Danger comes from pharmacological stacking. Multiple stimulants can push heart rate, blood pressure, temperature, agitation, and seizure risk in the same direction. Adding hypnosedatives, opioids, or alcohol can complicate recognition, respiration, aspiration risk, and emergency response.
Cathinones Led Overall, Tryptamines Rose in the 2020s
Blood toxicology detected 31 different NPSH, 13 of which were first detected in the 2020s. Cathinones were most common overall, appearing in 34 cases (48.6%). Frequent cathinones were α-pyrrolidinovalerophenone (α-PVP) and methylenedioxypyrovalerone (MDPV), each appearing in 11 cases.
Phenethylamines appeared in 27 cases (38.6%), with paramethoxymethamphetamine (PMMA) and N-benzylphenethylamines (NBOMe) prominent. Tryptamines appeared in 13 cases (18.6%), most often N,N-dimethyltryptamine (DMT) or 5-MeO-DMT. Piperazines appeared in 3 cases (4.3%).
Comparing 2020–2025 cases with earlier cases showed a clear change in the mix:
- Tryptamines increased: 36.7% of 2020–2025 cases vs. 5.0% of 2007–2019 cases; odds ratio (OR) 11.0, 95% confidence interval (CI) 2.2–54.7.
- Phenethylamines decreased: 23.3% vs. 50.0%; OR 0.3, 95% CI 0.1–0.9.
- Other novel psychoactive substances increased: 56.7% vs. 7.5%; OR 16.1, 95% CI 4.1–64.1.
- Cathinones stayed common: 50.0% vs. 47.5%; OR 1.1, 95% CI 0.4–2.9.
Cathinones still led overall. Tryptamines did not become the dominant fatal-toxicity class, but later fatal cases involved a wider and less predictable drug-market mix.
Acute Signs Were Agitation, Collapse, Hyperthermia, and Seizure
Signs and symptoms were documented in 41 cases (58.6%). Most often, reports described intense agitation in 16 cases (22.9%), sudden collapse in 16 (22.9%), hyperthermia in 14 (20.0%), seizure in 13 (18.6%), delirium in 12 (17.1%), respiratory distress in 7 (10.0%), and vomiting in 6 (8.6%).
These signs line up with what toxicology and emergency-medicine reports describe for synthetic cathinones, phenethylamines, and related stimulant/hallucinogen poisonings: cardiovascular stress, overheating, agitation, delirium, seizures, and rapid deterioration.3,4,5
Co-occurring symptoms were also informative. Intense agitation plus delirium appeared in 11 cases; intense agitation plus hyperthermia in 8; intense agitation plus seizure in 7; and hyperthermia plus seizure in 7. Those combinations are not subtle intoxication. They are emergency signs.
16 Deaths Involved Apparent Drug Misidentification
In 16 cases, people nearby reported that the person believed they had taken MDMA, methamphetamine, or LSD and did not mention an NPSH. That detail is one reason drug checking belongs in the discussion. Unknown substitution or unexpected co-presence changes risk because the user is dosing against the wrong mental model.
Smith et al. reported new psychoactive substances in Australian emergency departments through multi-center toxicosurveillance across 5 states in 2022–2023, showing the same drug-market problem during live emergency care.9 Emergency departments need testing strategies that can detect emerging substances alongside standard panels for older drugs.
Study results also support simple bystander messaging:
- Call emergency services for overheating, seizure, collapse, delirium, or extreme agitation. Waiting for someone to “come down” can be fatal when toxicity is escalating.
- Do not assume a purchased pill or powder is what it was sold as. The 22.9% apparent-unawareness figure is a direct warning.
- Polysubstance use changes the risk profile. Stimulant stacking and mixed sedative/stimulant patterns complicate toxicity.
Mental Health History Was Present but Suicide Was Not the Pattern
A documented substance-use history appeared in 38 cases (53.3%), injecting drug use in 29 (41.4%), and mental health issues in 24 (34.3%). Mental-health histories included affective disorders in 15 cases and psychotic disorders in 9.
Those numbers support treatment-access and risk-recognition work, while no case was coded as intentional self-poisoning.
Mental-health interpretation: substance-use disorders, mood disorders, psychosis, and drug-market unpredictability can converge in people who need earlier care, safer-use information, and emergency pathways that do not depend on perfect disclosure.
Limits of Coronial Data and Toxicology Drift
This case series is useful precisely because it is forensic and concrete, but several limits shape interpretation:
- Closed cases only: recent years are likely undercounted because some coronial investigations were still open.
- Known substances only: rapidly emerging NPSH may be missed if testing panels and laboratory methods lag the market.
- Poisoning deaths only: deaths from trauma or disease indirectly related to NPSH use were outside the case definition.
- Multiple-drug attribution is hard: blood toxicology can show what was present, but it cannot always assign exact causal weight to each drug in a mixed-toxicity death.
- Clinical-history data depend on records: substance-use history, mental health history, and circumstances of use were limited to what appeared in case files.
Even with those caveats, the forensic pattern is clear: fatal NPSH poisonings in Australia were dominated by polysubstance toxicology, private-setting incidents, and a shifting drug-market mix that became broader in the 2020s.
Questions About New Psychoactive Stimulants and Hallucinogens
Which NPSH classes drove these Australian deaths?
They are newer or emerging psychoactive drugs with stimulant, hallucinogenic, or mixed effects. Major groups include synthetic cathinones, phenethylamines, tryptamines, and piperazines.
Were these mostly festival deaths?
No. Most fatal incidents occurred in private settings, and fewer than 5 occurred at music festivals. Home and private-setting deaths are central to the public-health interpretation of this study.1
Which drug class appeared most often?
Cathinones appeared most often overall, present in 34 of 70 cases (48.6%). Tryptamines became more common in the 2020s but did not overtake cathinones overall.
What symptoms should trigger emergency action?
Sudden collapse, seizure, hyperthermia, delirium, severe agitation, respiratory distress, or repeated vomiting after stimulant or hallucinogen use should be treated as emergency signs.
Does drug checking solve this problem?
No single intervention solves it, but drug checking directly addresses one problem in the data: some people appeared unaware they had consumed an NPSH. Drug checking, emergency toxicology, and fast medical response work together.
What should future surveillance measure?
Future surveillance should combine emergency-department toxicology, drug-checking results, coronial data, and market-monitoring systems. That mix is better suited to fast-changing drug supplies than any single data source.
References
- The toxicology and characteristics of fatal new psychoactive stimulant and hallucinogen-related poisonings in Australia, 2000–2025. Darke S et al. Drug and Alcohol Dependence Reports. 2026;19:100434. doi:10.1016/j.dadr.2026.100434
- Characteristics and circumstances of death related to new psychoactive stimulants and hallucinogens in Australia. Darke S et al. Drug and Alcohol Dependence. 2019;204:107556. doi:10.1016/j.drugalcdep.2019.107556
- Synthetic cathinones and neurotoxicity risks: a systematic review. Daziani G et al. International Journal of Molecular Sciences. 2023;24:6230. doi:10.3390/ijms24076230
- Cardiotoxicity after synthetic cathinone use: 2 cases, a case series, and scoping review. Groenewegen KL et al. Cardiovascular Toxicology. 2024;24:209–224. doi:10.1007/s12012-024-09832-x
- Reports of adverse events associated with use of novel psychoactive substances, 2013–2016. Logan BK et al. Journal of Analytical Toxicology. 2017;41:573–610. doi:10.1093/jat/bkx031
- A review of synthetic cathinone-related fatalities from 2017 to 2020. La Maida N et al. Therapeutic Drug Monitoring. 2021;43:52–68. doi:10.1097/ftd.0000000000000808
- Psychedelic-related deaths in England, Wales and Northern Ireland (1997–2022). Kopra EI et al. Progress in Neuro-Psychopharmacology and Biological Psychiatry. 2025;136:111177. doi:10.1016/j.pnpbp.2024.111177
- Fatalities following DMT use: 2 case reports and a review of the literature. Pullen J et al. Journal of Analytical Toxicology. 2025. doi:10.1093/jat/bkaf064
- Novel psychoactive substances in Australian emergency departments: implications for public health practice from multi-center prospective toxicosurveillance across 5 states, 2022–2023. Smith JL et al. International Journal of Drug Policy. 2025;145:104969. doi:10.1016/j.drugpo.2025.104969