
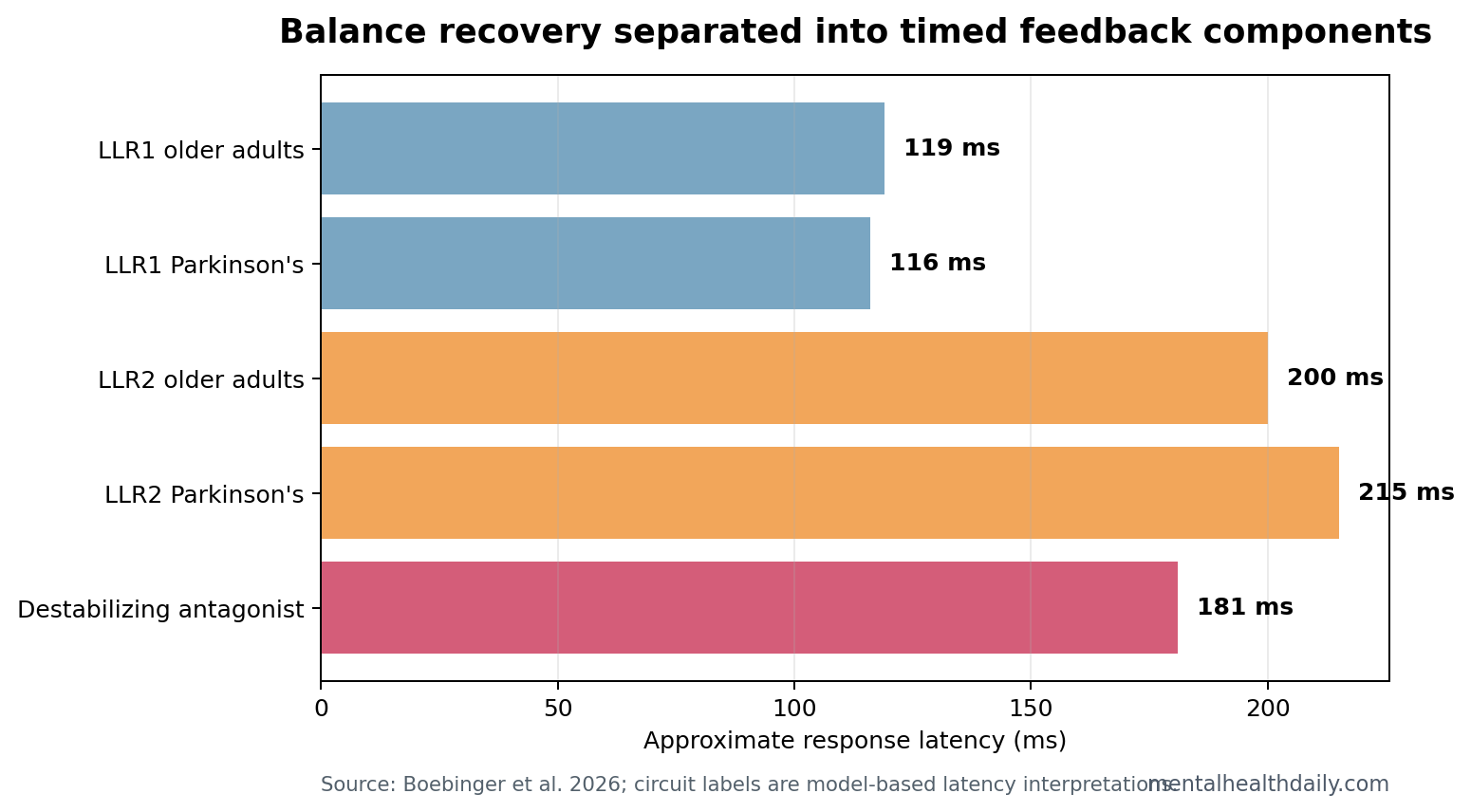
A 36-person Parkinson’s disease balance study found that perturbation-evoked muscle activity could be split into brainstem-latency LLR1 responses around 116-119 ms, cortical-latency LLR2 responses around 200-215 ms, and an antagonist destabilizing component around 173-181 ms.1 Parkinson’s disease lowered clinical balance scores, but the broad claim that Parkinson’s patients had higher cortical-latency LLR2 responses than older adults without Parkinson’s disease did not hold.
Research Highlights
- 36 people were analyzed: the study included 19 older adults and 17 people with Parkinson’s disease after 3 Parkinson’s participants were excluded.
- Challenge scaled the response: LLR1 and LLR2 both increased as perturbations moved from small to medium and large, with LLR1 around 116-119 ms and LLR2 around 200-215 ms.
- Parkinson’s did not broadly enlarge LLR2: LLR2 magnitude did not significantly differ between groups, contrary to the Parkinson’s-specific prediction.
- Clinical balance was lower in Parkinson’s: miniBEST scores differed by group (t(19.28) = 2.4; p = 0.027), even though stepping rates were similar at 9.25% vs. 8.21%.
- Destabilizing antagonist activity carried signal: the antagonist component around 180 ms correlated with poorer balance in older adults, but not in the Parkinson’s group.
Reactive balance recovery means the rapid correction that follows an unexpected shift under the feet. In this experiment, participants stood on a motorized platform while support-surface perturbations varied by direction and magnitude.
Long-latency responses are muscle responses that arrive later than simple spinal reflexes. Boebinger et al. treated LLR1 as a brainstem-latency component and LLR2 as a cortical-latency component because the timing matched known feedback-loop delays.
48 Platform Perturbations Tested Balance Without Stepping
The study analyzed 19 older adults and 17 people with Parkinson’s disease. Parkinson’s participants withheld dopaminergic medications for at least 12 hours, so the physiology reflects an off-medication testing state rather than normal daily medication coverage.1
Each participant received 48 translational platform perturbations: forward and backward directions across 3 magnitudes. Small perturbations were 5.1 cm at 11.1 cm/s and 0.15 g; medium perturbations were around 7-7.4 cm at 15.2-16.1 cm/s and 0.21-0.22 g; large perturbations were 8.9-9.8 cm at 19.1-21.0 cm/s and 0.26-0.29 g.
Trials with steps were excluded because stepping changes the motor goal. The overall stepping rate was 8.71%, with 9.25% in Parkinson’s disease and 8.21% in older adults without Parkinson’s disease. That similarity is useful: the model looked beneath stepping frequency into the timing of balance correction.
LLR1 and LLR2 Increased as Perturbations Became Larger
The model reconstructed muscle activity from center-of-mass displacement, velocity, and acceleration. Center of mass is the body’s overall balance point; when it moves relative to the feet, the nervous system has to correct the error quickly enough to prevent a fall.
LLR1 occurred around 119 ms in older adults and 116 ms in people with Parkinson’s disease. LLR2 occurred around 200 ms in older adults and 215 ms in Parkinson’s disease. The LLR2 latency difference reached significance only for backward perturbations (F(1, 34) = 4.17; p = 0.049), while LLR1 latency did not differ by group.
Model implication: older adults and people with Parkinson’s disease both recruited a longer-latency control component as balance challenge increased. The result supports a hierarchy of feedback loops rather than one generic reflex.
Parkinson’s Lowered Balance Scores Without a Broad LLR2 Magnitude Difference
Clinical balance differed between groups. People with Parkinson’s disease had lower mini Balance Evaluation Systems Test scores than older adults without Parkinson’s disease (t(19.28) = 2.4; p = 0.027). miniBEST is a balance test covering sensory orientation, dynamic gait, anticipatory postural control, and reactive postural control, with higher scores indicating better balance.
At the same time, the main LLR2 magnitude comparison did not separate the groups. LLR2 magnitude increased with perturbation magnitude in both forward and backward directions, but group effects were not significant (forward p = 0.78; backward p = 0.73).
That is the calibration point. Parkinson’s disease participants had poorer clinical balance, while the latency-based cortical component showed a more selective pattern than a one-line “more cortical control” claim would suggest.
The Antagonist Component Around 180 ms Was Clinically Selective
The model also separated antagonist muscle activity into stabilizing and destabilizing components. Antagonist muscles oppose the prime mover. During balance recovery, some co-contraction can stabilize the body, while poorly timed activity can resist the needed correction.
The destabilizing antagonist component occurred at 181 ± 3.6 ms in older adults and 173 ± 2.9 ms in Parkinson’s disease, with no significant group difference. But amplitude patterns mattered. The destabilizing component increased with perturbation magnitude in both groups, and the acceleration-driven piece was larger in Parkinson’s disease for forward perturbations (p = 0.048; feedback-gain p = 0.017).
In older adults without Parkinson’s disease, greater destabilizing antagonist output correlated with lower miniBEST balance ability. The same correlation did not appear in the Parkinson’s group, suggesting that Parkinson’s balance impairment may involve additional sources of variance not captured by that single component.
Latency-Based Circuit Labels Are Useful but Indirect
Evidence-strength note: the study did not record cortical activity directly. It inferred brainstem-, cortical-, and basal-ganglia-linked components from timing, muscle activity, and model structure. That is a reasonable mechanistic approach, but it is not the same as electroencephalography, magnetoencephalography, intracranial recording, or stimulation evidence.
Why the off-medication state matters: Parkinson’s participants were tested off dopaminergic medication, so the results describe a relatively unassisted motor-control state. The design is useful for detecting disease-linked timing problems. On-medication testing would still be needed before assuming the same response pattern after levodopa or other dopaminergic treatment.
The model still adds value because ordinary clinical observation cannot see these loops. A clinician sees a patient recover balance or step. The model separates rapid balance correction into timed pieces that may respond differently to age, Parkinson’s disease, medication state, perturbation size, and rehabilitation.
Adjacent Parkinson’s balance work has repeatedly suggested that cortical activity increases when balance becomes more demanding, but this lower-limb perturbation study shows why the statement needs precision.2 Some feedback components scaled with challenge; broad Parkinson’s-specific LLR2 enlargement did not.
Rehabilitation Logic Points Toward Feedback Timing
Balance rehabilitation is often discussed as strength, gait, confidence, or fall prevention. Those categories are useful, but the 2026 study points to timing. If a person has excessive or poorly timed antagonist activity, generic strengthening may not fully solve the neural-control problem.
Assessment target: perturbation-based testing can expose recovery patterns that quiet standing or straight-line walking can miss. A patient may walk acceptably in clinic yet struggle when the floor moves, the body is bumped, or the center of mass shifts unexpectedly.
Training target: reactive balance training may need to challenge multiple perturbation magnitudes and directions. The fact that LLR1 and LLR2 scaled with perturbation magnitude suggests the nervous system adjusts feedback loops according to task difficulty.
Medication context: Parkinson’s participants were tested off dopaminergic medication. Future work should compare off-medication and on-medication states before turning these model outputs into treatment decisions.
Why Similar Stepping Rates Still Leave a Parkinson’s Signal
One easy misread is that similar stepping rates make the Parkinson’s finding unimportant. The opposite is closer. Because 9.25% of Parkinson’s trials and 8.21% of older-adult trials involved stepping, the model had a chance to look beneath the obvious behavioral outcome.
Same gross outcome, different control strategy: 2 people can both avoid stepping, but one may do it with cleaner feedback timing and the other with more co-contraction, more cortical effort, or a larger destabilizing antagonist component. That difference matters for fatigue, dual-task walking, uneven terrain, and real-world fall risk.
Why perturbation magnitude matters: the nervous system did not produce one fixed response. LLR1 and LLR2 scaled as platform motion became larger. That scaling is clinically relevant because falls often happen when an ordinary response is suddenly inadequate for a larger-than-expected challenge.
Why the null group effect matters: the lack of a broad Parkinson’s LLR2 increase keeps the interpretation honest. Parkinson’s disease can involve greater cortical engagement during balance, but this study’s lower-limb automatic postural responses did not support a simple disease-wide LLR2 magnitude story.
Clinical signal vs. diagnosis signal: the antagonist component is more interesting as a balance-control marker than as a diagnostic marker. It may help explain why some people with similar stepping rates still differ in stability, fatigue, and fall vulnerability, but it is not ready to classify individual Parkinson’s patients on its own.
Next measurement step: pairing this perturbation model with EEG, functional near-infrared spectroscopy, or transcranial magnetic stimulation would test whether the latency-based cortical label matches direct cortical physiology in the same people and same task.
Questions About Parkinson’s Balance Control
Did Parkinson’s disease patients have worse balance in the study?
Yes. The Parkinson’s group had lower miniBEST clinical balance scores (p = 0.027), although stepping rates during the analyzed perturbation trials were similar between groups.
Did the study prove that cortex caused the LLR2 response?
No. LLR2 was interpreted as cortical-latency based on timing and prior work. Direct brain recordings were not part of this analysis.
Which balance signal did this study add?
Reactive balance impairment may involve the timing and sign of feedback loops, including antagonist activity, co-contraction, weak muscles, and slow walking.
References
- Boebinger SE, Payne AM, Xiao J, et al. Cortically-mediated muscle responses to balance perturbations increase with perturbation magnitude in older adults with and without Parkinson’s disease. eNeuro. 2026. https://doi.org/10.1523/eneuro.0423-25.2026
- PubMed search: Parkinson disease cortical activity balance perturbation. https://pubmed.ncbi.nlm.nih.gov/?term=Parkinson+disease+cortical+activity+balance+perturbation
- PubMed search: long latency response Parkinson disease postural perturbation. https://pubmed.ncbi.nlm.nih.gov/?term=long+latency+response+Parkinson+disease+postural+perturbation
- PubMed search: miniBEST Parkinson disease reactive balance falls. https://pubmed.ncbi.nlm.nih.gov/?term=miniBEST+Parkinson+disease+reactive+balance+falls