A 745-child cohort found positive MCHAT-R/F autism screens in 22 of 218 children exposed to maternal SARS-CoV-2 infection during pregnancy (10.1%) vs. 30 of 527 pre-pandemic controls (5.7%; p = 0.03).1 The same 2026 analysis added a small serum-proteomics layer: exposed newborns who later screened positive showed altered immune and metabolic markers, but the paper does not prove that COVID-19 caused autism.
Research Highlights
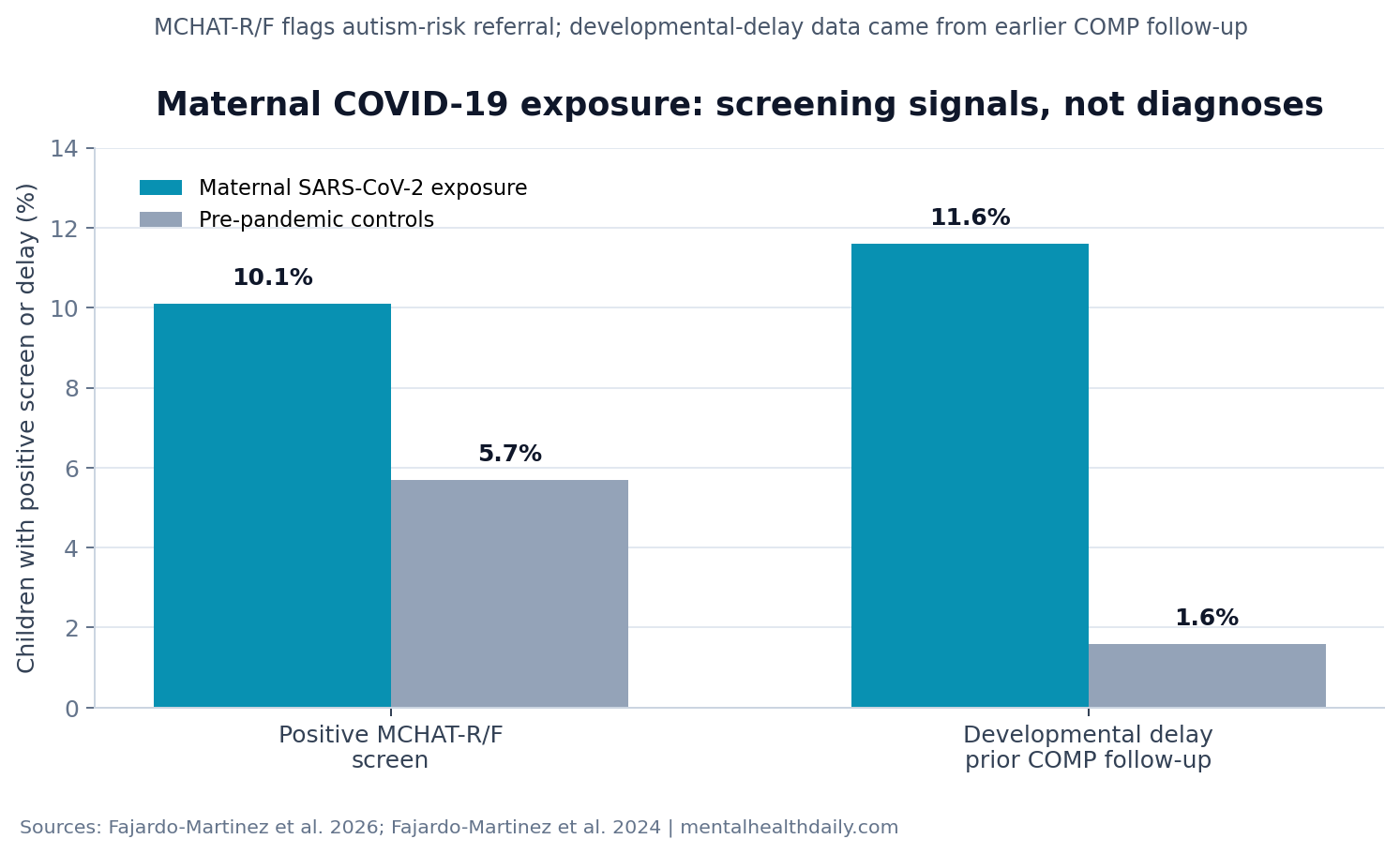
- Autism-screen positivity was higher after pregnancy COVID-19: 10.1% of exposed children screened positive on MCHAT-R/F vs. 5.7% of controls, a statistically significant difference (p = 0.03).1
- The outcome was a screen, not a diagnosis: MCHAT-R/F flagged toddlers screened between 18 and 32 months who needed evaluation; it was not confirmed autism spectrum disorder.1
- Prior developmental-delay data pointed the same direction: the same cohort previously reported developmental delay in 11.6% of exposed children vs. 1.6% of controls when ASQ follow-up was included.2
- The immune signal was exploratory: infant proteomics involved only 34 newborns, including 4 exposed children who later screened positive, so the pathway findings are hypothesis-generating.1
- Large cohorts remain mixed: a 2,003-pregnancy ASPIRE cohort found no adjusted increase in abnormal developmental screens through 24 months after maternal COVID-19 exposure.4
MCHAT-R/F means Modified Checklist for Autism in Toddlers-Revised with Follow-Up, a 2-stage parent questionnaire used to identify toddlers who should receive more detailed developmental evaluation. In the original validation study, children who remained screen-positive after follow-up had a high probability of autism or another developmental concern, but the tool was designed for referral, not diagnosis by itself.6
Maternal immune activation means immune signaling during pregnancy that may alter fetal development indirectly, even when the pathogen does not infect the fetal brain. That distinction is central here: the researchers reported immune-signature plausibility, not confirmed fetal infection or a one-step causal chain.
10.1% of Exposed Children Screened Positive vs. 5.7% of Controls
Fajardo-Martinez et al. followed mother-child dyads from the COVID Outcomes in Mother-Infant Pairs study in Los Angeles and Rio de Janeiro. Pregnant participants had laboratory-confirmed SARS-CoV-2 infection during pregnancy, and children were screened for autism risk between 18 and 32 months. Controls were children born before the pandemic who had MCHAT-R/F results from routine pediatric care.1
Autism-screen result: 22 of 218 exposed children had a positive MCHAT-R/F screen, compared with 30 of 527 controls. That works out to 10.1% vs. 5.7%, with p = 0.03.1
Clinical meaning: the signal supports developmental follow-up for exposed children, especially because screen-positive children were referred for diagnostic early-intervention services. A 10.1% screen-positive rate means more children crossed a referral threshold; many screen-positive toddlers ultimately receive another developmental diagnosis, and some are false positives.
Several baseline differences make the comparison harder than a simple exposed-vs.-unexposed headline. Exposed pregnancies had more cesarean delivery, hypertensive disorders, diabetes, obesity, and mental-health disorders than controls. Those differences may partly reflect pandemic-era care patterns, maternal health, or cohort selection rather than SARS-CoV-2 biology alone.1
Male Sex and Maternal Vaccination Were the Only Adjusted Signals
Among exposed children, the adjusted model found 2 statistically significant predictors of a failed MCHAT-R/F screen. Male infant sex was associated with higher odds of a positive screen (adjusted OR 1.12, 95% CI 1.03-1.22; p = 0.01). Maternal SARS-CoV-2 vaccination before delivery was associated with lower odds (adjusted OR 0.89, 95% CI 0.82-0.98; p = 0.02).1
Non-significant factors: preterm birth did not remain significant after adjustment (adjusted OR 1.13, 95% CI 0.97-1.32; p = 0.12). Infection trimester also did not separate risk: second vs. first trimester adjusted OR 0.98 (p = 0.76), and third vs. first trimester adjusted OR 1.01 (p = 0.85). Fever during pregnancy, COVID-19 severity, low birth weight, small-for-gestational-age status, and head circumference categories were also not significant predictors in the exposed cohort.1
The vaccination association should be kept narrow. Observational vaccination status can track health behavior, access to care, exposure timing, infection severity, and other unmeasured differences. The paper can support the possibility that reducing maternal infection severity or inflammatory burden helps infant outcomes. It cannot prove that vaccination prevents autism.
Small Proteomics Subsets Pointed to Immune and Metabolic Pathways
Proteomics measures large panels of proteins in blood or tissue to identify biological pathways that differ between groups. This study used the Olink Explore 1536 platform, a proximity-extension assay that links antibody detection to sequencing readouts, in small nested maternal-infant serum subsets.1
Infant proteomics included 34 newborns: 27 exposed infants and 7 controls. Only 4 exposed infants in that subset later screened positive on MCHAT-R/F. Against that small base, the researchers reported 62 altered serum biomarkers in exposed screen-positive children, with enrichment in nicotinamide biosynthesis, neutrophil extravasation, and microglial cell activation.1
Nicotinamide biosynthesis feeds NAD+ biology, a cellular energy and redox system needed for neuron survival and stress handling. Microglial activation refers to activity in immune-like brain support cells that can shape synapse pruning, inflammation, and neurodevelopment. Neutrophil extravasation means immune cells moving from blood vessels into tissue, a marker of inflammatory traffic rather than a brain-specific autism mechanism.
Maternal proteomics included 52 women: 33 SARS-CoV-2-positive pregnant women and 18 controls. Compared with healthy pregnancies, SARS-CoV-2-positive mothers whose children later screened positive showed 34 altered biomarkers, with apoptosis-related signaling upregulated. Apoptosis is programmed cell death; in pregnancy biology, it can reflect injury response, placental stress, or immune remodeling depending on context.1
Evidence-strength note: the proteomics layer is best treated as a mechanism map. It can identify candidate pathways for replication. It cannot classify individual children, diagnose autism, or prove that a specific immune protein caused a later screen result.
Prior COVID-19 Pregnancy Development Studies Are Not Uniform
The same COMP cohort previously reported developmental delay in 11.6% of exposed children vs. 1.6% of controls when Bayley-III and Ages and Stages Questionnaire results were combined.2 Bayley-III is a standardized developmental assessment administered by trained evaluators; ASQ is a parent-completed screening questionnaire. The 2 tools do not measure exactly the same thing.
Santos et al. studied a Brazilian cohort and reported developmental impairment in children exposed during pregnancy to maternal SARS-CoV-2, with language delays standing out during first-year assessments.3 That result supports the idea that some exposed cohorts show developmental vulnerability, but it still leaves open whether the driver is maternal infection biology, pandemic conditions, preterm birth, health-system disruption, or a mix of those forces.
Jaswa et al. reported the counterweight. In the ASPIRE cohort, 2,003 pregnant individuals enrolled before 10 weeks’ gestation, and child ASQ-3 data were collected at 12, 18, and 24 months. Exposed children did not show higher adjusted risk of abnormal developmental screens at 12 months (ARR 1.07, 95% CI 0.85-1.34), 18 months (ARR 1.15, 95% CI 0.84-1.57), or 24 months (ARR 1.01, 95% CI 0.69-1.48).4
The mixed evidence makes the Fajardo-Martinez result more useful as a follow-up signal than as a final verdict. A positive MCHAT-R/F pattern plus immune-pathway differences gives clinicians and researchers a reason to watch exposed children carefully. It does not make every exposed pregnancy a high-risk autism case.
Maternal Immune Activation Is Plausible, But Cohort Design Limits Causal Claims
Foo et al. previously mapped the systemic inflammatory landscape of COVID-19 in pregnancy using mother-infant serum proteomics, showing that in utero exposure can leave measurable immune signatures even when vertical transmission is uncommon.5 The 2026 paper reuses that biological logic and links it to later developmental screening.
That link is plausible because fetal brain development is sensitive to immune signaling, placental vascular function, oxidative stress, and metabolic stress. But plausibility is not causality. Pandemic-era exposed children and pre-pandemic controls differ in calendar time, care patterns, family stress, viral exposure context, vaccination availability, and follow-up environment.
Best current use: children exposed to maternal COVID-19 during pregnancy should not be labeled as autistic because of exposure history. They should receive ordinary developmental surveillance with a lower threshold for timely screening and referral when language, social-communication, motor, or sensory concerns appear.
Replication target: the next useful studies need confirmed autism diagnoses after age 36 months, contemporaneous controls, maternal vaccination and infection-severity data, placental measures, infant immune markers, and repeated developmental assessments. The strongest design would separate effects of maternal infection from effects of being born during the pandemic.
Questions About Maternal COVID-19 and Autism Screening
Does this study show that maternal COVID-19 causes autism?
No. It found more positive autism screens after maternal SARS-CoV-2 exposure and exploratory immune signatures in small serum subsets. A positive MCHAT-R/F screen is a referral signal, not a confirmed autism diagnosis.
What should parents do with a positive MCHAT-R/F screen?
A positive screen should lead to follow-up evaluation and early-intervention referral when appropriate. Waiting for diagnostic certainty can waste months during a period when speech, occupational, behavioral, and developmental supports may help.
Was vaccination protective in this study?
Maternal vaccination before delivery was associated with lower adjusted odds of a failed MCHAT-R/F screen, but the observational design cannot prove protection against autism. The result is compatible with lower infection severity, better prenatal care access, or other unmeasured differences.
Why include immune biomarkers if the sample was small?
The biomarker results help identify pathways worth testing in larger cohorts. They should be read as biological plausibility evidence, not as a clinical blood test for autism risk.
References
- Fajardo-Martinez V, Ferreira F, Salem GM, et al. Maternal-infant immune signatures in infants at risk for SARS-CoV-2-associated neurodevelopmental disorders. Communications Biology. 2026. doi:10.1038/s42003-026-10019-z
- Fajardo-Martinez V, Ferreira F, Fuller T, et al. Neurodevelopmental delay in children exposed to maternal SARS-CoV-2 in-utero. Scientific Reports. 2024;14:11851. doi:10.1038/s41598-024-61918-2
- Santos CAD, et al. Developmental impairment in children exposed during pregnancy to maternal SARS-COV2: A Brazilian cohort study. International Journal of Infectious Diseases. 2024;139:146-152. doi:10.1016/j.ijid.2023.12.001
- Jaswa EG, Huddleston HG, Lindquist KJ, et al. In utero exposure to maternal COVID-19 and offspring neurodevelopment through age 24 months. JAMA Network Open. 2024. PubMed:39412802
- Foo SS, et al. The systemic inflammatory landscape of COVID-19 in pregnancy: extensive serum proteomic profiling of mother-infant dyads with in utero SARS-CoV-2. Cell Reports Medicine. 2021;2:100453. doi:10.1016/j.xcrm.2021.100453
- Robins DL, Casagrande K, Barton M, Chen CMA, Dumont-Mathieu T, Fein D. Validation of the Modified Checklist for Autism in Toddlers, Revised With Follow-up (M-CHAT-R/F). Pediatrics. 2014;133:37-45. doi:10.1542/peds.2013-1813