Psychedelic-assisted therapy has been one of the most-covered mental-health stories of the past decade. A 2026 quantitative analysis by Evers and colleagues maps how media enthusiasm grew, peaked, and partially pulled back across major U.S. outlets — and how the coverage related to the actual evidence base for depression and PTSD.1
Research Highlights
- Psychedelic clinical trials (psilocybin for depression, MDMA for PTSD) have shown promise across several phase 2 and 3 studies, though FDA approval has been delayed and methodological concerns including functional unblinding remain unresolved.2
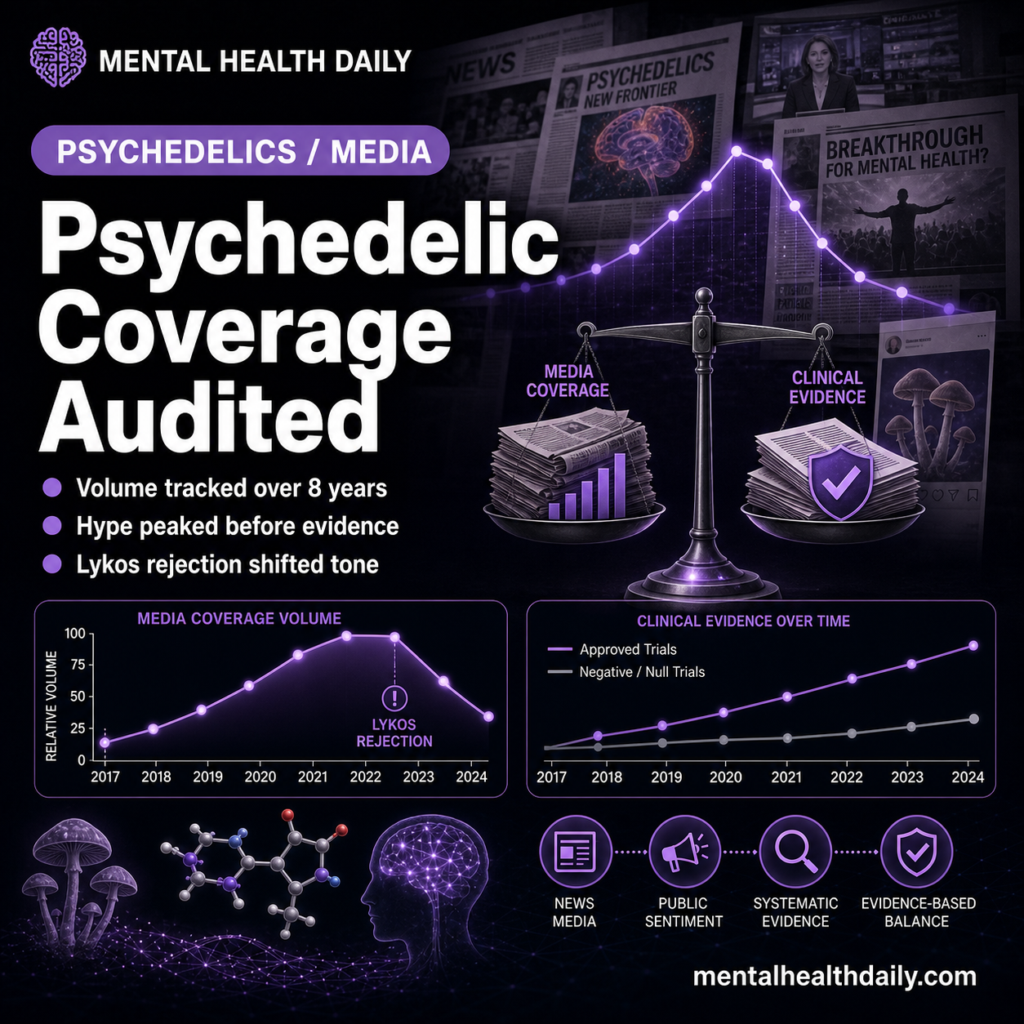
- The Evers 2026 study systematically analyzed media coverage of psychedelic treatments for depression and PTSD across major U.S. outlets from 2017 through 2024, tracking volume, sentiment, and accuracy.1
- Coverage volume grew substantially from 2017 to 2022, with peak enthusiasm typically preceding peak evidence quality. Articles often emphasized benefits while underemphasizing methodological limitations.1
- The Lykos MDMA-PTSD FDA rejection in 2024 produced a noticeable shift in coverage tone, with more critical analysis of trial methodology and regulatory concerns appearing thereafter.1,3
- Implications for science communication: the gap between media enthusiasm and evidence quality affected patient expectations, clinical-trial enrollment, and broader public discourse about psychedelic medicine.1
The arc of psychedelic-medicine coverage from 2017 to 2024 included Michael Pollan’s influential 2018 book, multiple high-profile clinical trials, the Lykos FDA submission and 2024 rejection, and a continuing landscape of evolving regulatory and scientific developments.2,4
Whether media coverage tracked the underlying evidence base or ran ahead of it has been a contested question. The Evers analysis provides quantitative data on this question, with implications for how the broader psychiatric drug-development pipeline communicates with public audiences during ongoing clinical-trial readouts.
Systematic Coverage Analysis Across Major U.S. Outlets
The trigger paper analyzed psychedelic-treatment coverage across major U.S. media outlets from 2017 through 2024.1
Articles were identified through systematic database searching with structured keyword queries for psilocybin, MDMA, ketamine, ayahuasca, and related terms paired with depression or PTSD.
Each identified article was coded for sentiment (positive, negative, balanced), accuracy (faithful representation of study findings), emphasis (benefits vs limitations), and other features relevant to evidence-quality alignment.
Coverage Volume Peaked Before Evidence Did
The headline pattern: coverage volume grew dramatically from 2017 to 2022, with peak enthusiasm preceding peak evidence quality.1
Major positive coverage waves followed individual phase 2 trial publications, regulatory designations (FDA Breakthrough Therapy for psilocybin and MDMA), and high-profile clinical-program announcements.
The volume-evidence mismatch reflects the standard pattern in emerging-treatment coverage: each positive signal generates substantial coverage, while limitations and replication failures typically receive less attention.
Tone Shifted After the Lykos FDA Rejection
The 2024 Lykos MDMA-PTSD FDA rejection marked a clear inflection point in coverage tone.1,3
Pre-rejection coverage tended toward cautious optimism with limited methodological critique. Post-rejection coverage included more substantive engagement with trial-design concerns: functional unblinding, therapist-patient relationship issues, and informed-consent and regulatory-process questions.
The shift demonstrates that media coverage *can* engage with methodological rigor when triggered by external events, but the trigger has to be substantial.

What Coverage Underemphasized
Several aspects of the evidence base received insufficient attention in the Evers media-coverage analysis:
Functional unblinding. The dramatic subjective effects of psychedelics make placebo-controlled blinding nearly impossible. Patients usually know whether they received active drug, which inflates effect-size estimates compared to genuinely blinded interventions.5
Sample size and replication. Headline-generating trials often had small samples, with replication patterns that didn’t consistently mirror the initial signals.
Cost and accessibility. The therapy structure of psychedelic-assisted treatment requires substantial therapist time, increasing per-treatment costs and accessibility constraints that aren’t obviously addressable through standard healthcare reimbursement.6
Adverse-event characterization. Coverage emphasized treatment effects without proportional attention to adverse-event profiles, including the rare but serious psychiatric reactions documented in some patients.
The Patient-Expectation Consequences
Inflated media coverage has downstream consequences for patient expectations and clinical encounters.1
Patients with treatment-resistant depression or PTSD often arrive at consultations expecting psychedelic-assisted therapy as imminent or effective options, sometimes despite limited current availability and unresolved approval status.
Managing expectations becomes its own clinical challenge, requiring extended conversations about what the evidence actually supports vs what coverage has implied.
Realistic framing serves patients better than enthusiasm-matched expectations followed by disappointment. Disappointment often reduces engagement with available evidence-based treatments and can compound treatment-resistance over time, with downstream consequences for clinical-care continuity.
Where Media Coverage Did Add Value
The Evers framework isn’t purely critical of media coverage.1
Coverage substantially raised public awareness of treatment-resistant depression and PTSD as serious conditions warranting better treatment options. This visibility likely improved help-seeking and reduced stigma in some patient populations.
Coverage also pressured regulatory agencies to engage more substantively with novel treatment paradigms, potentially supporting broader regulatory innovation around psychedelic and adjacent therapies.
The challenge isn’t that coverage existed but that volume outpaced calibration to evidence quality.
How the Field Could Communicate Better
Three improvements emerge from the analysis pattern.1
Researchers communicating to media could emphasize methodological context proactively rather than waiting for journalists to surface limitations. Framing trial findings against unresolved methodological questions helps coverage stay calibrated.
Journalists covering psychedelic medicine could systematically include functional-unblinding context, sample-size caveats, and replication patterns as standard elements rather than occasional additions.
And patient-facing health-communication infrastructure (advocacy organizations, mental-health resources) could provide reality-checked summaries that bridge between research papers and general media coverage.
The Evers Analysis Has Methodological Limits
Three caveats apply.
Coverage analysis depends on subjective coding decisions about sentiment and accuracy that reasonable analysts might score differently.
The U.S.-focused sample doesn’t capture international media patterns where psychedelic policy and coverage have evolved differently.
And the relationship between media volume and patient expectations is inferred rather than directly measured. The mechanistic link from coverage to patient behavior isn’t empirically established.
Common Questions About Psychedelic Treatment Evidence and Media
What does the actual evidence show for psychedelic treatments?
Psilocybin for treatment-resistant depression has shown signal across several phase 2 trials, though phase 3 evidence is still emerging. MDMA for PTSD showed positive phase 3 results but FDA rejection in 2024 due to methodological and regulatory concerns. Both areas remain active with ongoing trials.2,3
Why did the FDA reject MDMA for PTSD?
The 2024 rejection cited concerns about trial methodology including functional unblinding, therapist-patient relationship issues affecting outcome assessment, and unresolved questions about study integrity. The decision didn’t reject the underlying treatment concept but the specific evidence package submitted.3
What is functional unblinding?
The phenomenon where patients can tell whether they received active drug or placebo based on subjective effects. With psychedelics, the dissociative and perceptual effects make blinding nearly impossible, which can inflate effect-size estimates beyond what genuinely blinded studies would show.5
Are these treatments available now?
In limited contexts. Ketamine and FDA-approved esketamine are available for treatment-resistant depression. Psilocybin and MDMA are not FDA-approved for psychiatric indications but are accessible through clinical trials, religious-exemption frameworks, and (for ketamine) some clinical practices. State-level psilocybin programs exist in Oregon and Colorado.6
How should patients evaluate psychedelic-treatment claims?
Look for: peer-reviewed evidence in published trials, methodological context including blinding and sample size, replication patterns across studies, and realistic discussion of adverse events. Skepticism toward enthusiasm-only coverage is warranted.1
Does media coverage change patient outcomes?
Indirectly. High coverage shapes patient expectations, which affect placebo responses and treatment-seeking behavior. Whether the net effect on clinical outcomes is positive or negative depends on whether expectations align with realistic treatment effects.1
Are journalists overhyping psychedelics?
The Evers data suggest coverage volume has exceeded what evidence quality alone would warrant. Whether this constitutes problematic hype depends on whether the increased visibility produces net benefits (awareness, regulatory engagement) that outweigh the costs (inflated expectations, premature commercial activity).1
What’s the next study that needs to happen?
Direct measurement of how media coverage affects patient expectations and clinical-trial recruitment, plus continued tracking of evidence-coverage alignment as the regulatory landscape evolves through 2025-2027 with additional trial readouts and FDA decisions.
References
- Evers A, Stade EC, Salecha A, Tait Z, Khazanov G. Media hype regarding psychedelic treatments for depression and PTSD from 2017 to 2024. Scientific Reports. 2026. doi:10.1038/s41598-026-50186-x
- Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. New England Journal of Medicine. 2022;387(18):1637–1648. doi:10.1056/nejmoa2206443
- Mitchell JM, Bogenschutz M, Lilienstein A, et al. MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine. 2021;27:1025–1033. doi:10.1038/s41591-021-01336-3
- Pollan M. How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression, and Transcendence. Penguin Press; 2018. doi:10.1080/02791072.2018.1535149
- Muthukumaraswamy SD, Forsyth A, Lumley T. Blinding and expectancy confounds in psychedelic randomized controlled trials. Expert Review of Clinical Pharmacology. 2021;14(9):1133–1152. doi:10.1080/17512433.2021.1933434
- Yaden DB, Earp BD, Griffiths RR. Ethical issues regarding nonsubjective psychedelics as standard of care. Cambridge Quarterly of Healthcare Ethics. 2022;31(4):464–471. doi:10.1017/s096318012200007x