A 2026 longitudinal study found reassuring cognitive trajectories after mild-to-moderate COVID-19: Alpha/Delta and Omicron groups both improved by follow-up, and neither group showed persistent neuropsychological test deficits vs. population norms. Psychiatric symptoms and fatigue were also broadly similar across variants.1
Research Highlights
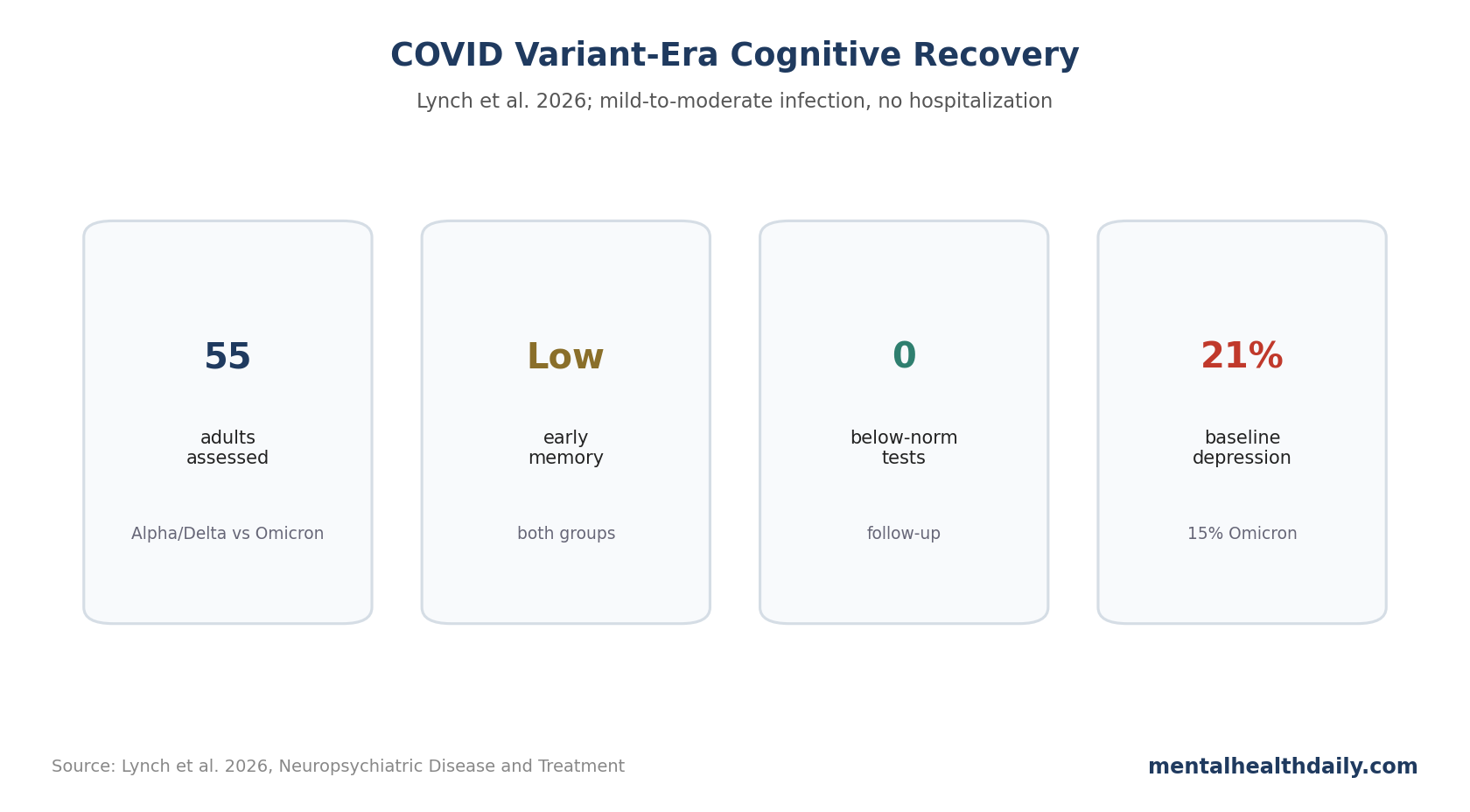
- 55 adults were assessed: 27 were infected during the Alpha/Delta era and 28 during the Omicron era; participants were not hospitalized and were not recruited from a specialty post-acute sequelae of COVID-19 clinic.1
- 1 early memory domain was low: both groups scored below norms on Repeatable Battery for the Assessment of Neuropsychological Status (RBANS) Immediate Memory at the first assessment.1
- 0 participants worsened at follow-up: at reassessment, no neuropsychological test score in either group remained significantly below population norms, and no participant worsened over time.1
- Depression remained worth watching: clinically significant depressive symptoms affected 21.4% of Alpha/Delta and 14.8% of Omicron participants at baseline, then 14.8% and 9.5% at follow-up.1
- Variant differences were limited: Omicron did not look clearly better or worse than Alpha/Delta on psychiatric distress, fatigue, or most cognitive outcomes in this 55-adult sample.
This cohort separates lower-severity COVID recovery from more disabled long-COVID clinic samples. It studied people after mild-to-moderate infection who were not hospitalized and were not seeking specialty care for post-acute sequelae of COVID-19 (PASC), so its findings should not be applied to severe, hospitalized, or highly symptomatic long-COVID cohorts.
Alpha/Delta and Omicron Groups Had Similar Neuropsychiatric Profiles
Lynch et al. compared adults infected during earlier Alpha/Delta waves with adults infected during the Omicron era. The Alpha/Delta group had 27 participants at follow-up; the Omicron group had 21 at follow-up.1
- Illness severity: participants had mild-to-moderate acute COVID-19 and were not hospitalized.
- Cognitive battery: testing included RBANS domains, Trail Making Test A/B, verbal fluency, and Stroop Color-Word.
- Psychiatric measures: depression, anxiety, PTSD symptoms, and fatigue were measured with standard symptom scales.
- Variant assignment: variant group was inferred from infection timing, not individual viral sequencing.
Referral bias was actively narrowed: the investigators excluded 47 Alpha/Delta participants and 1 Omicron participant who were seeking care through a post-COVID recovery program. That choice makes the study less representative of disabled long-COVID clinics, but more useful for asking what happens in lower-severity adults who recover outside specialty PASC care.1
Follow-up timing also differed by variant era: Alpha/Delta participants returned about 381 days after infection, while Omicron participants returned about 275 days after infection.1
At the first assessment, both groups showed some degree of neuropsychological test impairment. Both performed below normative expectations on RBANS Immediate Memory. The Omicron group also scored below norms on Trail Making Test A, a processing-speed/simple-attention measure.
Immediate Memory and Processing Speed Were Early Signals
Initial RBANS Immediate Memory performance was lower than expected in both groups: Alpha/Delta t = −2.636, p = 0.014, Cohen’s d = −0.498; Omicron t = −2.594, p = 0.015, Cohen’s d = −0.499.1
In plain English, immediate memory measures how efficiently someone can take in and reproduce new information right away. It is not the same as dementia or permanent memory loss.
The Omicron group also had lower Trail Making Test A performance at baseline: t = −3.499, p = 0.002, d = −0.673. Trail Making Test A is a timed visual scanning and processing-speed task.
Follow-Up Testing Showed Improvement Rather Than Decline
The follow-up results were the most clinically reassuring part. At reassessment, neither group had neuropsychological test scores significantly below population norms, and no participant showed worsening neuropsychological performance over time.1
Classification also improved. In the Alpha/Delta group at follow-up, 59.3% had no impairment, 37.0% had mild impairment, and 3.7% had moderate-to-severe impairment. In the Omicron group, 66.7% had no impairment, 33.3% had mild impairment, and 0% had moderate-to-severe impairment.
The clinical interpretation should stay calibrated: this study supports improvement in a lower-severity sample, not the claim that all long-COVID cognitive symptoms are mild or self-limited.
Depression, Anxiety, PTSD, and Fatigue Did Not Separate by Variant
At baseline, mean psychiatric scores were generally in the non-clinical range and did not differ significantly between Alpha/Delta and Omicron groups. Clinically significant depression was present in 21.4% of Alpha/Delta participants and 14.8% of Omicron participants at the initial visit.1
At follow-up, depression rates were lower: 14.8% in Alpha/Delta and 9.5% in Omicron. Anxiety was 14.8% and 9.5%, PTSD symptoms were 14.8% and 4.8%, and clinically significant fatigue was 11.1% and 0%.
Large database studies have found elevated neurological and psychiatric risks after SARS-CoV-2 infection, including risk trajectories that differ by diagnosis and age.2 Meta-analyses focused on long COVID also report depression, anxiety, and sleep problems, but often combine more symptomatic and more clinically selected samples than Lynch et al.’s cohort.5
Limitations of This COVID Recovery Cohort
The sample was modest. With 55 adults initially and fewer at follow-up, the study can miss smaller variant differences.
Variant status was inferred by timing. The timing-based method fits population surveillance, but it is not viral sequencing at the individual level.
The cohort was not a severe PASC clinic sample. Results should not be generalized to patients with disabling long COVID, prior hospitalization, intensive-care exposure, or marked autonomic or immune complications.
Recovery Averages Should Not Erase Persistent Outliers
The average recovery pattern is reassuring, but average improvement can hide people who remain impaired. Even at follow-up, 37.0% of the Alpha/Delta group and 33.3% of the Omicron group remained in the mild impairment classification.
That mild category is easy to dismiss on paper. In daily life, mild inefficiency can still matter if a person is returning to a cognitively demanding job, caring for children, managing complex medication schedules, or trying to study full-time.
Function can diverge from test scores. A clinic battery may look normal on a good morning, while symptoms later in the day still limit real-world cognition:
- Energy limits: fatigue, sleep disruption, and post-exertional symptom flares can reduce sustained attention even when brief testing looks normal.
- Body-state limits: orthostatic symptoms, migraine, and pain can make cognitive performance fluctuate across the day.
- Task-load limits: work, school, caregiving, driving, and medication management require longer concentration than many clinic tasks measure.
Test normalization is good news, but it is not a complete functional assessment.
For clinicians and patients, follow-up should stay concrete: can the person do the work, school, caregiving, driving, and decision-making tasks that their life requires? If not, symptom management, pacing, sleep treatment, rehabilitation, and mental-health support may still be appropriate.
Reassurance still needs follow-up. Improvement over time should lower catastrophic fear, while persistent impairment should still be taken seriously and evaluated on its own terms.
Variant Comparisons Are Hard Because Time Changed Everything
Alpha/Delta and Omicron occurred in different social, medical, and immunological eras. Vaccination availability, treatment access, public fear, isolation rules, prior infection, work disruption, and testing practices all changed across time.
That makes variant comparison difficult even with a consistent testing battery. If the Omicron group looks better, that could reflect variant biology, vaccination, less severe acute illness, prior immunity, or different pandemic context. If groups look similar, some of those forces may be pushing in opposite directions.
Lynch et al. handled the comparison cautiously by focusing on measured cognitive and psychiatric outcomes. The improvement in both groups carries more weight than any small variant-era difference, and the cohort cannot isolate a clean viral mechanism.
The reader-facing question is whether mild-to-moderate infection in lower-severity samples tends to show cognitive improvement over time. In this cohort, the answer was yes, while symptom persistence still deserved follow-up.
Depression Screening Still Belongs in Post-COVID Follow-Up
The depression signal is easy to miss because the cognitive recovery pattern is more reassuring. At baseline, depressive symptoms were above general-population estimates in both groups, and some symptoms persisted at follow-up.
Depression can worsen subjective cognition, sleep, fatigue, pain, and motivation. It can also coexist with objective cognitive inefficiency. Post-COVID follow-up should therefore avoid a false split between brain fog and mood: both can be assessed without implying that one makes the other fake.
Function Measures Belong Beside Cognitive Test Scores
Future studies should pair neuropsychological tests with work status, school performance, driving confidence, medication management, exercise tolerance, and daily fatigue ratings. A person can test within norms and still struggle in a cognitively loaded life.
Longer follow-up would also help separate recovery from adaptation. Some people may improve biologically; others may learn pacing strategies, reduce workload, or avoid tasks that trigger symptoms. Both matter clinically, but they imply different treatments.
Questions About COVID Brain Fog and Variant Differences
Does Omicron cause less brain fog than Alpha or Delta?
This study did not show a major Omicron advantage in this lower-severity sample. Both groups had early cognitive findings and both improved.
Does normal follow-up testing mean symptoms are imaginary?
No. Neuropsychological tests can miss fluctuating fatigue, sleep disruption, dysautonomia, or real-world cognitive load. Normal testing means the measured domains were not persistently below norms.
References
- Neurocognitive and Psychiatric Outcomes Associated with Mild-to-Moderate COVID-19 Infection Across Variant Eras. Lynch et al. doi:10.2147/ndt.s594322
- Neurological and psychiatric risk trajectories after SARS-CoV-2 infection. Taquet et al. doi:10.1016/s2215-0366(22)00260-7
- Cognition and Memory after COVID-19 in a Large Community Sample. Hampshire et al. doi:10.1056/nejmoa2311330
- Neurocognitive and psychiatric outcomes associated with postacute COVID-19 infection without severe medical complication: a meta-analysis. Knapp et al. doi:10.1136/jnnp-2024-333950
- Global prevalence of depression, anxiety, and sleep disorder among patients coping with long COVID. Seighali et al. doi:10.1186/s12888-023-05481-6