A 2026 preprint following 964 adults who used a Chicago mobile medical unit for opioid use disorder care found 5 follow-up patterns over 12 months: 56% made 1 visit, while the remaining patients showed slow decline, fast decline, infrequent use, or continued use.1
Research Highlights
- The cohort was large for mobile OUD care: 3,528 OUD-related encounters were recorded for 980 individuals, with 964 included after exclusions.1
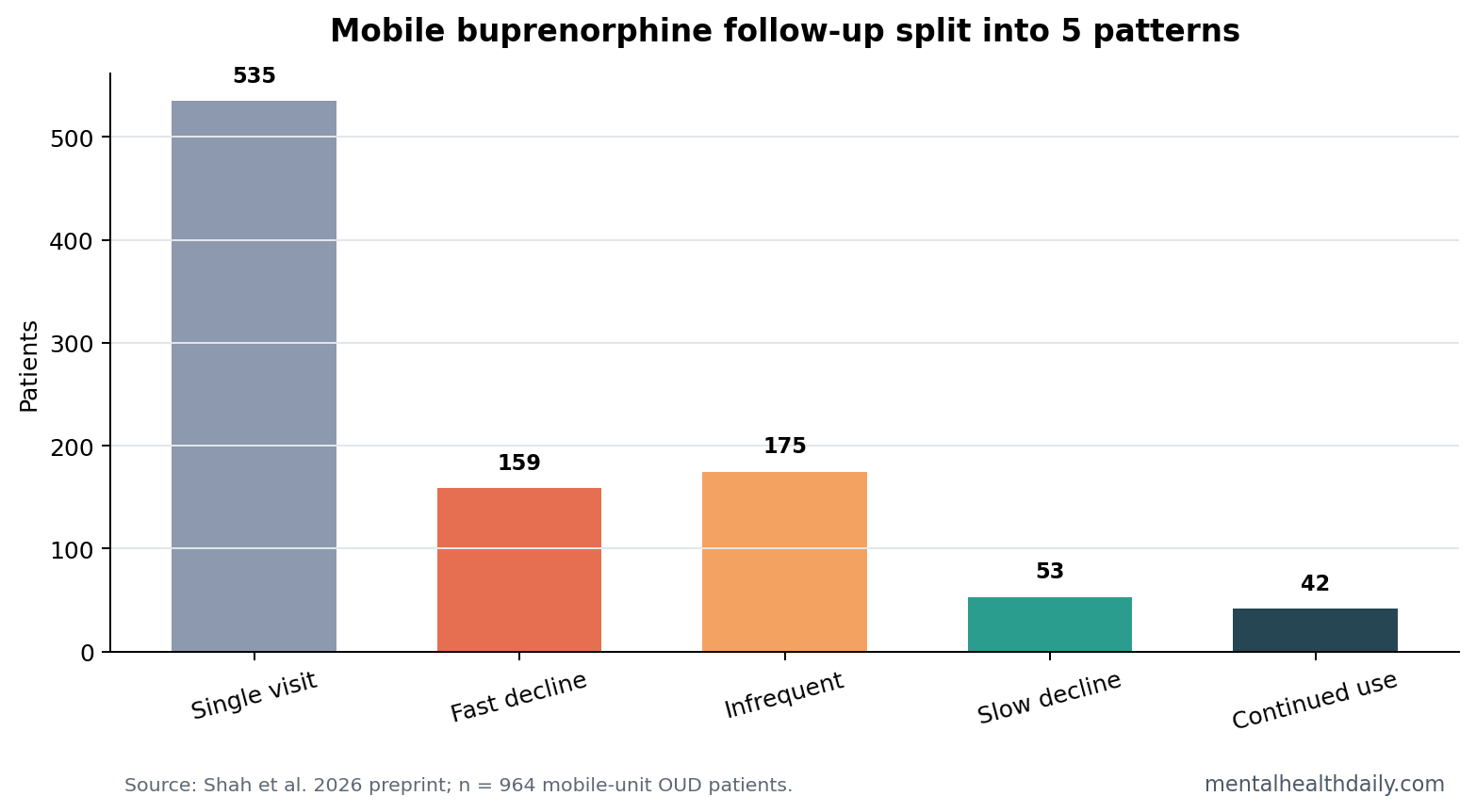
- Single visits dominated: 535 of 964 patients, or 56%, had only 1 mobile-unit visit during the 1-year observation window.1
- Repeat visitors split into 4 trajectories: slow-decline (6%), fast-decline (16%), infrequent (18%), and continued-use (4%) patterns appeared in group-based trajectory modeling.1
- On-site medication mattered descriptively: buprenorphine was dispensed on site in 51% of encounters, and slow-decline visitors had the highest on-site dispensing proportion at 57%.1
- Retention is not the whole story: low-threshold buprenorphine models intentionally reduce barriers, so a 1-visit or infrequent-use pattern may include bridge care, re-entry care, or backup access rather than simple disengagement.2,3
Medications for opioid use disorder (MOUD) are evidence-based medications such as buprenorphine, methadone, and extended-release naltrexone that reduce opioid craving, withdrawal, overdose risk, and illicit opioid use. Buprenorphine is a partial opioid agonist, meaning it activates opioid receptors enough to suppress withdrawal and craving while having a ceiling effect that lowers respiratory-depression risk compared with full agonists.
Low-threshold buprenorphine care tries to remove common access barriers: rigid appointment systems, abstinence demands, long intake processes, stigma, insurance friction, and pharmacy obstacles. A mobile unit carrying buprenorphine on site changes the care equation because medication can be delivered at the point of contact.
56% of Patients Made 1 Mobile-Unit Visit
Shah et al. analyzed 964 adults after excluding 16 people suspected of diversion. The cohort averaged 46.4 years of age; 72% were male, 58% identified as Black or African American, 26% identified as White, and 83.7% had insurance.1
The headline number is blunt: 535 people, or 56%, had a single mobile-unit visit over the 1-year period after their first encounter. Another 44% returned for at least 1 follow-up visit. The mean number of OUD-treatment visits across the full cohort was 3.5.
Repeat Visitors Split Into 4 Engagement Trajectories
Group-based trajectory modeling is a statistical approach that sorts people into groups with similar change patterns over time. Instead of asking only whether a patient returned, the method asks what the return pattern looked like during the year after the first visit.
- Slow-decline group: 53 people (6%) averaged 9.6 OUD-treatment visits, with predicted visit likelihood falling from 57% to 0% over about 30 weeks.
- Fast-decline group: 159 people (16%) averaged 3.1 visits, with predicted visit likelihood dropping from 45% to 0% over about 10 weeks.
- Infrequent group: 175 people (18%) averaged 4.9 visits, with predicted visit likelihood staying between 6% and 3%.
- Continued-use group: 42 people (4%) averaged 22.6 visits, with predicted visit likelihood between 39% and 19% across the year.
On-Site Buprenorphine Changed the Access Model
Buprenorphine was dispensed on site in 51% of encounters. The slow-decline group had the highest proportion of on-site buprenorphine dispensing at 57%, while the continued-use group had 44%.1 Fast-decline and infrequent visitors were significantly less likely than single-visit patients to receive buprenorphine at their mobile-unit visit.
That pattern should not be flattened into “more visits equals better care.” Mobile OUD services can function as several different things: primary medication source, emergency access point, bridge to another clinic, wound-care entry point, or medication backup after a return to use.
Low-Threshold Care Makes Retention Harder to Interpret
Jakubowski and Fox described low-threshold buprenorphine as care designed to maximize access and reduce treatment friction.2 Harris et al. described mobile low-threshold buprenorphine integrated with infectious-disease services, showing how mobile programs can reach people outside ordinary clinic pathways.3
Those models create a measurement problem. In a conventional clinic, not returning may mean treatment dropout. In a low-threshold mobile model, not returning may mean the person moved to another medication source, used the mobile unit as a bridge, or needed only a short burst of access.
The Best Metric May Be Matched to the Service Role
For a mobile unit dispensing buprenorphine, the right outcome depends on the intended role:
- Primary-care role: sustained visits, medication continuity, and overdose reduction matter most.
- Bridge role: linkage to ongoing MOUD elsewhere may matter more than mobile-unit retention.
- As-needed access role: rapid re-entry after relapse or treatment interruption may be the central outcome.
- Harm-reduction role: low-friction medication availability may reduce risk even when visit frequency is low.
Evidence Strength and Limits
Evidence-strength note: this was a preprint retrospective analysis from 1 urban mobile medical unit. It can describe follow-up patterns inside that program and generate better retention metrics. It cannot prove that mobile buprenorphine caused better recovery, lowered overdose risk, or outperformed fixed-site clinics.
The largest missing piece is care outside the mobile unit. Without pharmacy fills, methadone-clinic attendance, buprenorphine prescriptions from other clinicians, incarceration, hospitalization, and mortality data, mobile-unit visit patterns are only a partial view of treatment engagement.
Single-Visit Care Can Still Be Clinically Useful
The single-visit group is easy to misread. In a conventional retention framework, 1 visit looks like failure. In a low-threshold model, 1 visit may still mean the person received buprenorphine, had overdose risk addressed, got wound care, re-entered treatment after a gap, or used the mobile unit while another treatment path was being arranged.
That interpretation fits the program design. The mobile unit served neighborhoods with unmet OUD treatment need, carried buprenorphine on site, and recorded 3,528 encounters across the 964-person cohort.1
A low-barrier visit can therefore be clinically meaningful even when it does not become a year-long treatment relationship. The weaker reading is not “retention does not matter”; it is that retention has to be separated from access, bridging, and care received outside the mobile unit.
Program data also showed that the follow-up groups were demographically similar, so the trajectories should not be read as simple age, sex, or race categories. The more useful interpretation is operational: different visit patterns may need different outreach, medication, and linkage strategies.
Measurement implication: mobile-unit programs need outcomes that distinguish absence of care from care elsewhere. A patient who stops visiting because they stabilized with a clinic is different from a patient who stopped visiting because housing instability, incarceration, withdrawal, or stigma blocked treatment. The same visit count can represent opposite clinical stories.
Trajectory Groups Can Guide Program Design
The 5-pattern result is operationally useful because each group suggests a different service problem. Slow-decline patients may need step-down linkage before contact fades. Fast-decline patients may need early outreach within the first 10 weeks. Infrequent users may need an explicit as-needed medication plan. Continued-use patients may need the mobile unit protected as a stable care source rather than treated as a temporary bridge.
That is the value of trajectory modeling here. It turns a blunt retention percentage into a service map. The next version should connect those patterns to overdose, medication continuity, patient goals, and care received outside the mobile unit.
Insurance and On-Site Dispensing Point to Access Friction
The slow-decline group had the highest insurance proportion at 92%, while single-visit patients had the lowest at 78%.1 That does not prove insurance caused follow-up, but it fits the broader access story: even low-threshold care still sits inside insurance, transportation, pharmacy, housing, and documentation systems.
On-site dispensing: a mobile unit that hands buprenorphine to a patient at the encounter removes a major weak point in the usual pathway: leaving with a prescription that still has to survive pharmacy stock, cost, stigma, travel, and withdrawal timing. In this study, the mobile unit carried 2-, 3-, or 7-day dose packs, which made rapid medication access possible without a separate pharmacy step.1
Clinical Success Needs Patient-Goal Outcomes
A low-threshold OUD program may be successful even when the clinic’s own retention number looks modest. A patient may want withdrawal relief, safer use, medication after a lapse, wound care, bridge treatment, or a route into longer-term care. Those goals are different, and they need different outcome measures.
Future mobile-unit studies should therefore ask what the patient was trying to accomplish at the visit. If the goal was short-term medication access before reconnecting with another provider, leaving the mobile unit is not failure. If the goal was long-term mobile-unit treatment and contact faded after 2 visits, the same pattern signals an implementation problem.
Questions About Mobile Buprenorphine Follow-Up
Does 56% single-visit use mean the mobile unit failed?
No. It means most patients did not return to that specific mobile unit within 1 year. For low-threshold care, a single visit can still mean medication access, referral, bridge treatment, or a harm-reduction contact.
Which group looked most like ongoing treatment?
The continued-use group had 42 people and averaged 22.6 visits. The slow-decline group also looked clinically meaningful, averaging 9.6 visits with a gradual falloff across about 30 weeks.
What should future mobile OUD studies add?
Future work needs medication continuity outside the mobile unit, overdose events, patient goals, housing instability, incarceration, hospital use, and mortality. Visit counts alone cannot define recovery.
References
- Shah KK, et al. Follow-up patterns at a low-threshold mobile medical unit dispensing buprenorphine for opioid use disorder. Research Square. 2026. https://doi.org/10.21203/rs.3.rs-9173540/v1
- Jakubowski A, Fox A. Defining Low-threshold Buprenorphine Treatment. Journal of Addiction Medicine. 2020. https://doi.org/10.1097/adm.0000000000000555
- Harris MTH, et al. Mobile low-threshold buprenorphine integrated with infectious disease services. Journal of Substance Abuse Treatment. 2022. https://doi.org/10.1016/j.jsat.2021.108553
- Krawczyk N, et al. Expanding low-threshold buprenorphine to justice-involved individuals through mobile treatment. Drug and Alcohol Dependence. 2019. https://doi.org/10.1016/j.drugalcdep.2019.02.029