A 2026 randomized comparison study of 152 Rwandan genocide survivors and released perpetrators found that 3-day Community Resiliency Model training improved social cohesion, compassion, forgiveness, and resilience over time, with social cohesion F(1) = 36.1, compassion F(1) = 131, forgiveness F(1) = 19.8, and resilience F(1) = 8.10.1 Mixed survivor-perpetrator groups improved slightly more, but that format advantage was not statistically confirmed.
Research Highlights
- Sample size was substantial for community trauma work: The study randomized 152 participants into survivor-only, perpetrator-only, or mixed survivor-perpetrator training groups.1
- All outcomes improved over time: Social cohesion, compassion, forgiveness, and resilience all increased from baseline through post-training and 6-month follow-up.1
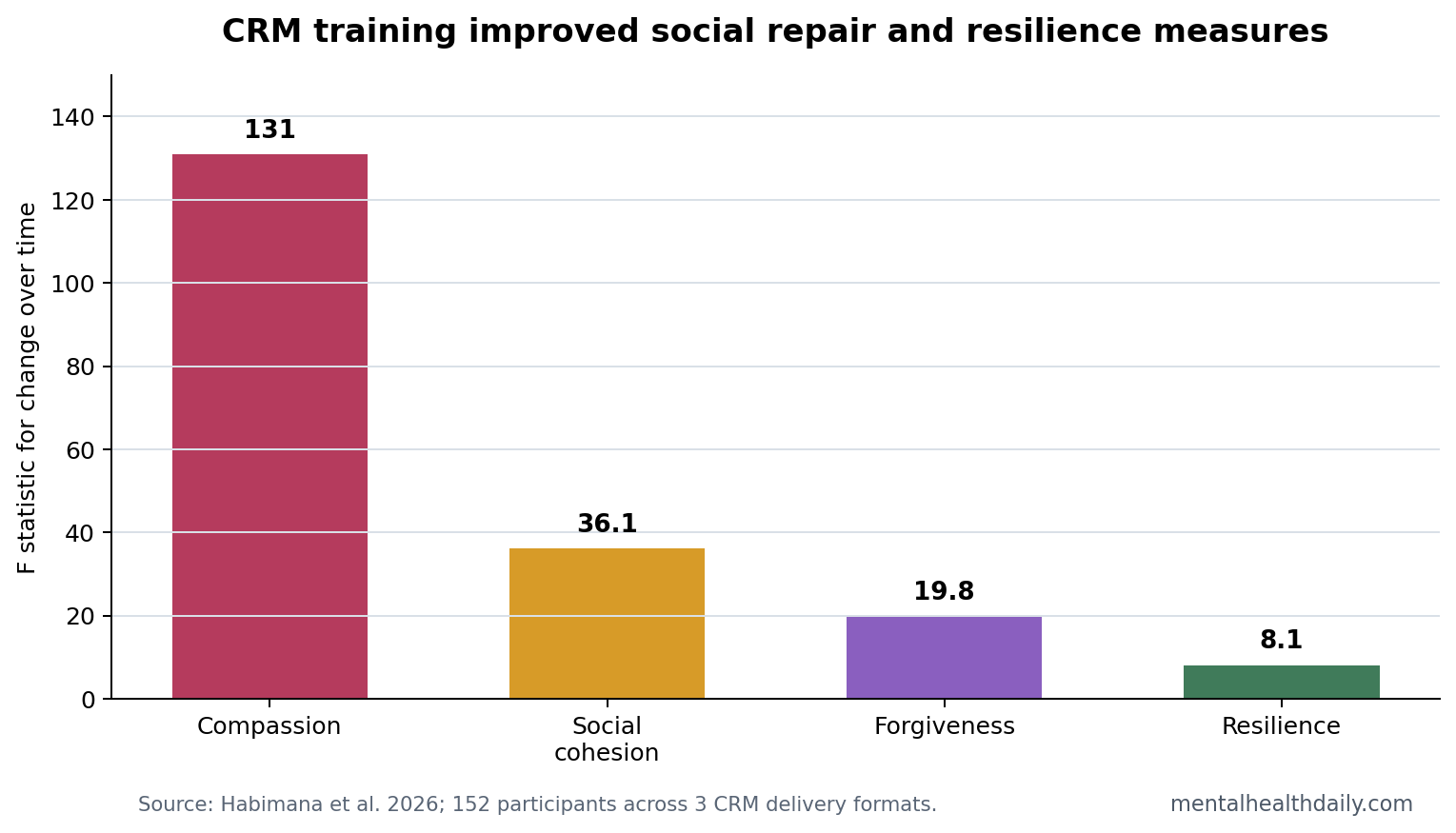
- Compassion had the strongest time effect: Compassion changed with F(1) = 131, p < .001, compared with forgiveness F(1) = 19.8 and resilience F(1) = 8.10.1
- Mixed delivery was not proven superior: Mixed survivor-perpetrator groups showed slightly more improvement, but between-format differences were not statistically significant.1
- Evidence strength is promising but bounded: Convenience sampling and absence of a no-treatment control mean the study supports feasibility and improvement over time more than definitive causal superiority.1
Community Resiliency Model (CRM) is a skills-based trauma-resilience intervention that teaches body awareness, grounding, tracking of nervous-system states, and practical self-regulation tools. It is not exposure therapy, and it is not primarily a narrative trauma-processing treatment.
Social cohesion in this study meant trust, connection, and willingness to function together after societal trauma. That endpoint is different from symptom reduction. The intervention was aimed at social repair as much as individual distress.
152 Participants Completed Survivor, Perpetrator, or Mixed Training
Habimana et al. assigned participants to 3 comparison groups: 51 genocide survivors, 51 released genocide perpetrators, and 50 mixed survivor-perpetrator participants. Each group completed 3 consecutive days of CRM training in community settings, with standardized measures collected at baseline, immediately after training, and 6 months later.1
The comparison was not “CRM vs. nothing.” It was CRM delivered in different social formats. That design answers a narrower but important question: whether the intervention appears useful across groups and whether mixed delivery outperforms homogeneous delivery.
Compassion, Forgiveness, Cohesion, and Resilience Improved
The within-person time effects were all statistically significant. Social cohesion improved with F(1) = 36.1, p < .001; compassion improved with F(1) = 131, p < .001; forgiveness improved with F(1) = 19.8, p < .001; and resilience improved with F(1) = 8.10, p = .005.1
- Social cohesion: stronger reported connection, trust, and group functioning.
- Compassion: stronger compassionate response toward others.
- Forgiveness: higher forgiveness-related scores in the post-genocide context.
- Resilience: stronger self-rated ability to recover from stress.
The strongest statistical signal was compassion. That fits the intervention’s mechanism: CRM does not ask participants only to think differently. It teaches nervous-system regulation skills that can make social contact less physiologically threatening.
Mixed Survivor-Perpetrator Groups Were Plausible, Not Clearly Better
The mixed group showed slightly more improvement than homogeneous groups, but the difference was not statistically significant. That is the key calibration. The mixed format may be socially important, and it may deserve more testing, but this study did not prove that mixed groups outperform separate survivor-only or perpetrator-only delivery.
Best reading: CRM appeared useful across all 3 group formats. If forced to choose based only on these data, the directional signal leans toward mixed delivery, but the statistical evidence supports broad improvement more strongly than format superiority.
Baseline Social Cohesion Was Already Uneven Across Groups
The groups were not identical at baseline. Social cohesion differed significantly before the intervention, F(2) = 3.59, p = .030. Post hoc testing found that participants in the perpetrators-only group reported higher baseline social cohesion than survivors-only participants, mean difference = 3.36, SE = 1.33, p = .038.1
Interpretation limit: a group that starts higher or lower can change differently for statistical reasons unrelated to the intervention format. Baseline imbalance does not erase the improvement over time, but it makes the mixed-vs.-homogeneous comparison harder to interpret cleanly.
The study also had no dropout, which is notable for a community intervention involving painful historical identities. Retention supports feasibility. It does not prove efficacy by itself, but it suggests the training format was acceptable enough for participants to complete.
Why This Belongs in Trauma Recovery Rather Than Wellness Framing
Rwanda’s 1994 genocide against the Tutsi left persistent psychological, family, and community damage. Prior work has documented long-term trauma burden, social disconnection, and gaps in trust after genocide exposure.2,3 In that context, social cohesion and forgiveness are not soft endpoints. They are community-function endpoints.
Body regulation: CRM focuses on recognizing and shifting stress physiology rather than generic positivity.
Post-conflict relevance: fear, arousal, shame, and defensive social withdrawal can block reconciliation even when people endorse reconciliation abstractly.
Body-Based Skills Could Affect Social Outcomes
Trauma recovery discussions often move quickly to beliefs, narratives, and attitudes. CRM starts lower in the system: noticing body sensations, identifying states of activation, and using grounding skills to return toward a tolerable zone. In a post-genocide context, that matters because social contact can trigger threat physiology before a person has time to reason through the interaction.
Resilience skills: participants learn to identify sensations linked to stability and distress, then practice shifting attention and behavior before arousal escalates.
Group delivery: practicing those skills with others may create repeated low-threat experiences of co-regulation. That is a plausible route to compassion and social cohesion, even when the training is not framed as direct forgiveness work.
Forgiveness endpoint: higher scores should not be read as moral closure. A forgiveness questionnaire can improve because avoidance, anger, or physiological reactivity softens, while historical accountability remains unchanged.
The Strongest Claim Is Improvement Over Time
The most defensible claim is that measured social functioning improved after CRM training and remained improved at follow-up. The study is less decisive about why improvement occurred and which delivery format should be preferred. A 3-day training can create skills, group contact, expectancy, facilitator support, and a rare structured space for painful social identities to be held together. Those ingredients are hard to separate without a stronger control condition.
Active-control need: future work should compare CRM against another credible group program with similar time, facilitator attention, and community contact. That would clarify whether body-based regulation skills add benefit beyond being gathered in a safe structured group.
Longer follow-up need: 6 months is useful, but community repair after genocide is a long-horizon outcome. Measures of trust, avoidance, community participation, conflict incidents, and intergroup cooperation would make the social-cohesion claim more concrete.
The paper remains valuable because it measured outcomes that are usually treated as too difficult or too political for intervention research. Compassion, forgiveness, and cohesion are not simple symptom scores, but they are central to whether post-conflict communities can function.
Implementation implication: the safest current use is as a community mental-health model that appears feasible across sensitive group compositions. Program planners should track adverse reactions, participant safety, facilitator training, cultural fit, local translation quality, follow-up support, and local accountability structures rather than treating improved questionnaire scores as enough by themselves in practice.
Post-genocide recovery also depends on economic conditions, justice systems, family networks, public memory, continuing local safety, and trusted institutions across generations in daily community life. A 3-day skills intervention cannot substitute for those systems. Its role, if replicated, is narrower: helping people regulate enough physiological threat to participate in repair processes that already have social and political support.
What This Rwanda Study Can and Cannot Support
Supported: in this sampled group, CRM training was followed by statistically significant improvements in social cohesion, compassion, forgiveness, and resilience across survivor-only, perpetrator-only, and mixed groups.
Not supported: proof that CRM caused all improvements independent of time, expectancy, community contact, or repeated measurement. The lack of a no-treatment control and use of convenience sampling limit causal certainty.
Best next test: larger community trials should compare CRM with waitlist or active control groups, test whether mixed delivery has delayed advantages, and measure practical outcomes such as community participation, avoidance, trust, and conflict resolution.
Follow-up timing is also essential. A short post-training improvement may reflect group support and attention, while durable change would require maintained forgiveness, safer interaction, and lower avoidance after participants return to ordinary community life.
Community trauma programs also need implementation outcomes: attendance, dropout reasons, facilitator fidelity, group safety, and whether participants continue using body-based skills after structured meetings end.
Those measures matter because reconciliation work can look improved in surveys while daily contact remains fragile.
Questions About CRM and Post-Genocide Recovery
Does this prove survivors and perpetrators should always train together?
No. Mixed groups improved slightly more, but the difference was not statistically confirmed. The data support feasibility and improvement across formats.
Is forgiveness the same as excusing harm?
No. In trauma research, forgiveness measures usually capture changes in resentment, avoidance, and willingness to relate. They do not erase responsibility or legal accountability.
Why measure compassion?
Compassion can indicate whether nervous-system regulation and group contact are translating into less defensive orientation toward others. In reconciliation work, that is a functional outcome.
References
- Habimana S, Freeman K, Biracyaza E, Lister Z, Montgomery S. Promoting social cohesion, compassion and forgiveness among Rwandan survivors and perpetrators through community resiliency model training: a longitudinal randomized comparison study. European Journal of Psychotraumatology. 2026;17:2621634. doi:10.1080/20008066.2026.2621634
- Fajth G, et al. Long-term mental health after the Rwandan genocide. PubMed
- Musanabaganwa C, et al. Burden of post-traumatic stress disorder among genocide survivors in Rwanda. PubMed
- Miller-Karas E. Community Resiliency Model and trauma resilience skills. PubMed