A 2026 functional magnetic resonance imaging study involving 54 adults found that pairing a formerly threatening cue with positive images, a laboratory method called counterconditioning, strengthened later neural safety-memory signals in people with posttraumatic stress disorder. The experiment measured fear-learning biology, not PTSD symptom improvement after therapy.1
Research Highlights
- 54 adults were analyzed: Cooper et al. included 22 trauma-exposed control participants and 32 participants with PTSD after exclusions.1
- Counterconditioning changed safety circuitry: cues paired with positive images produced lower activity than extinction cues in threat-related regions during safety learning.1
- vmPFC reinstatement persisted: at 1 month, the counterconditioned cue produced stronger ventromedial prefrontal cortex pattern reinstatement than the extinguished cue (β = 0.37, pFDR = .001).1
- Reward connectivity differed by group: basolateral amygdala-to-nucleus accumbens connectivity separated counterconditioning from safe cues in controls, but not significantly in PTSD.1
- Therapy claims need restraint: the 54-person study supports a mechanism for augmenting exposure learning, but it cannot show symptom reduction, relapse prevention, or treatment superiority.
Counterconditioning is a learning procedure that pairs a feared or threat-associated cue with a positive or rewarding outcome. Extinction learning repeatedly presents the feared cue without the expected bad outcome. Exposure therapy for anxiety and PTSD relies partly on extinction learning, but extinction can be fragile when threat memories return in new contexts or under stress.
Threat Cues Were Extinguished or Paired With Positive Images
The experiment used a fear-conditioning design during functional magnetic resonance imaging, which tracks blood-oxygen-level changes as an indirect measure of neural activity. Participants first learned that one visual cue predicted mild electric shock. Safety learning then split threat cues into 2 formats: standard extinction without shock and counterconditioning with positive image pairing.1
- CS+EXT: a previously threat-associated cue presented without shock during extinction.
- CS+CC: a previously threat-associated cue paired with positive images during counterconditioning.
- CS−: a cue that was never paired with shock and served as a safety comparison.
- Follow-up: participants returned after 24 hours and again after 1 month to test neural and behavioral recall.
vmPFC, or ventromedial prefrontal cortex, is a frontal brain region involved in safety learning, valuation, and regulation of threat responses. dACC, or dorsal anterior cingulate cortex, and the insula are commonly involved in threat appraisal, salience, and body-state monitoring.
Behavioral Fear Recall Did Not Fully Separate the 2 Safety Formats
Acquisition result: both groups learned the initial threat association. Shock expectancy and skin conductance responses were higher to the threat cue than to the safe cue during acquisition, and the difference diminished during safety learning.1
Behavioral recall: at 24 hours and 1 month, shock expectancy still showed moderate discrimination between the formerly shocked cue and the safe cue, with false-discovery-rate adjusted p values at or below .016. Skin conductance recall was less consistent, and the behavioral measures did not cleanly separate the extinguished cue from the counterconditioned cue.
The clearest counterconditioning evidence came from neural pattern and connectivity measures rather than from a simple self-report or sweat-response advantage.
Counterconditioning Lowered Threat-Region Activity During Safety Learning
Threat-region result: during safety learning, the counterconditioned cue produced lower activity than the extinguished cue in dorsal anterior cingulate cortex, insula, thalamus, and periaqueductal gray, with category-level false-discovery-rate adjusted p values at or below .03.1
Threat-region read: lower activity in those regions suggests that positive pairing changed how the formerly dangerous cue was represented while learning was happening. Bayesian analyses did not support strong group differences for this category effect, so the lower threat-region response applied broadly rather than being clearly PTSD-specific.
Basolateral amygdala-to-nucleus accumbens connectivity told a more group-specific story. Controls showed stronger connectivity for the counterconditioned cue than for the safe cue, with β = 0.63, 95% CI 0.23–1.04, and pFDR < .001. The PTSD group did not show significant connectivity differences.1
vmPFC Safety-Memory Reinstatement Lasted 1 Month
Durability result: at 1 month, the counterconditioned cue produced stronger vmPFC pattern reinstatement than the extinguished cue. The contrast was β = 0.37, 95% CI 0.11–0.62, with pFDR = .001.1
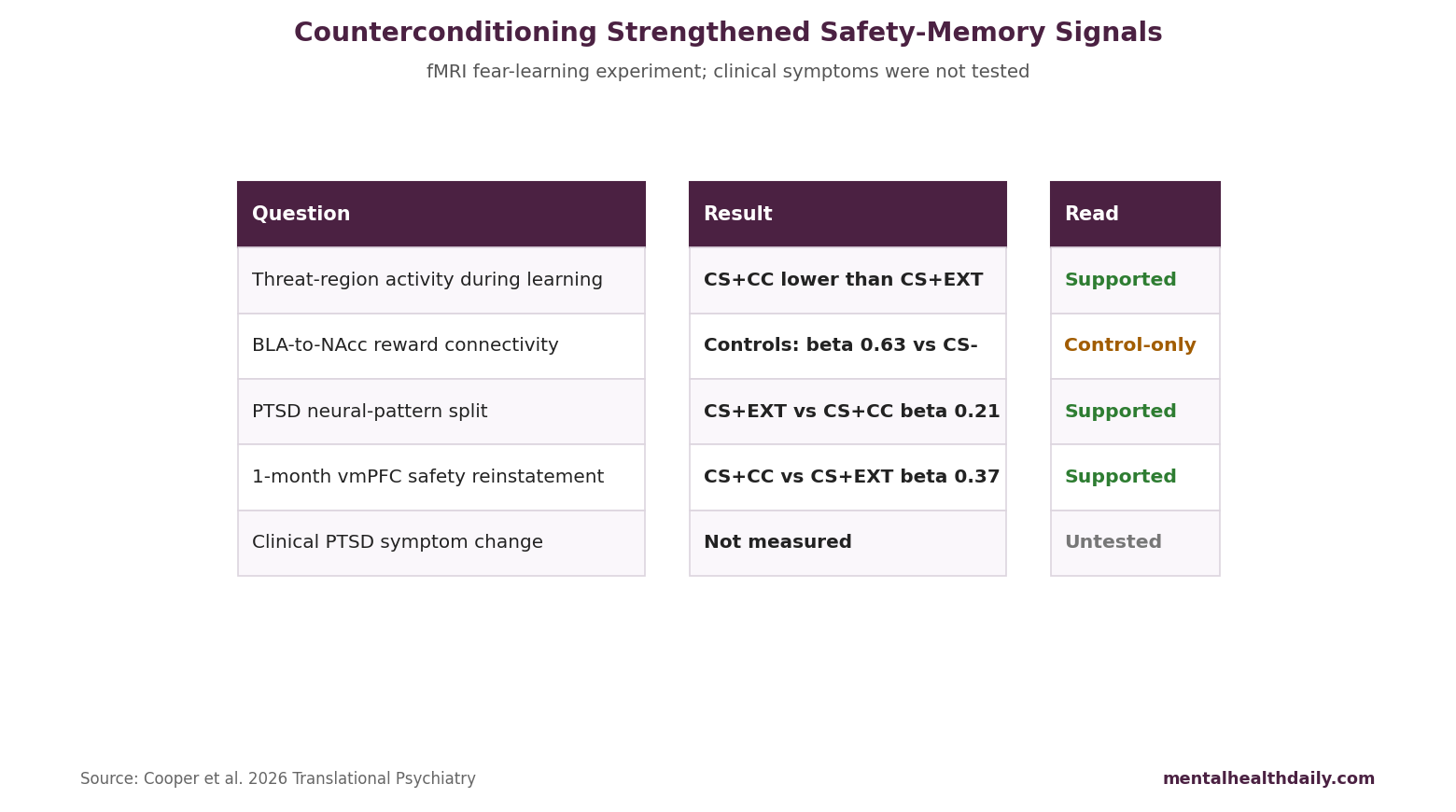
PTSD-specific pattern: participants with PTSD showed a significant neural-pattern difference between standard extinction and counterconditioning during recall, with β = 0.21, 95% CI 0.01–0.42, and pFDR = .02. Controls did not show the same cue-format split.1
Those neural findings fit the idea that positive-valence learning can strengthen safety representations after threat learning. They do not establish how much positive pairing should be added to exposure therapy, which patients should receive it, or whether it improves symptoms.
Adjacent Extinction Research Supports the Mechanism
Craske et al. argued that exposure therapy can be improved by focusing on inhibitory learning: new safety learning that competes with fear memory, rather than erasing the original fear association.2 Vervliet et al. similarly emphasized relapse phenomena after extinction, including renewal, reinstatement, and spontaneous recovery.3
Counterconditioning rationale: pairing a threat cue with positive value may create a richer safety memory than omission of shock alone. Keller et al. reviewed behavioral and neural counterconditioning processes and highlighted reward-related learning as a route to reduce fear expression.4
- Exposure mechanism: the person learns that feared cues can occur without catastrophe.
- Counterconditioning mechanism: the cue gains positive or rewarding associations beyond “no shock” associations.
- Clinical challenge: real trauma cues are complex, personal, contextual, and harder to pair cleanly with positive outcomes than laboratory images.
Evidence-Strength Note for This fMRI Experiment
What the design supports: this study can support mechanistic claims about fear learning, safety representations, and neural pattern reinstatement under controlled laboratory conditions. It cannot support claims about PTSD remission, exposure-therapy response, medication effects, relapse prevention, or real-world trauma recovery.
Design limits: the analysis sample was modest, follow-up behavioral differentiation was incomplete, and some analyses were exploratory. Electric-shock conditioning with visual cues is useful for isolating learning mechanisms, but PTSD symptoms arise from autobiographical trauma, avoidance, hyperarousal, sleep disruption, shame, threat appraisal, and social context.
Clinical translation would require a randomized therapy trial that adds positive-valence learning to trauma-focused treatment and measures PTSD symptoms, dropout, adverse effects, functional recovery, and relapse.
Counterconditioning Is a Mechanistic Exposure-Therapy Lead
Exposure link: exposure therapy already tries to build new safety learning. Counterconditioning suggests one possible enhancement: pair feared memories, cues, or contexts with structured positive value when doing so is clinically appropriate and not avoidant.
Implementation caution: positive pairing should not become reassurance, distraction, or avoidance that prevents trauma memory processing. A clinical version would need to preserve engagement with feared material while adding new meaning, reward, mastery, or safety cues.
For now, the strongest claim is mechanistic. Counterconditioning altered neural safety-memory signals in PTSD-relevant circuitry. Whether that improves therapy belongs to the next trial.
What a Therapy Trial Would Need to Measure
A clinical trial could test whether counterconditioning improves exposure therapy by adding positive-valence learning to trauma-focused sessions. The important endpoints would be PTSD symptom severity, dropout, avoidance, functional recovery, relapse after treatment, adverse reactions, and fear-learning brain signals.
Design requirement: the comparator would need to be credible exposure therapy without the positive pairing component. Otherwise, any advantage could come from extra therapist time, novelty, expectancy, or a more pleasant treatment experience rather than counterconditioning itself.
- Primary endpoint: clinician-rated PTSD severity after treatment and at follow-up.
- Mechanism endpoint: whether vmPFC safety-memory changes mediate symptom improvement.
- Safety endpoint: whether positive pairing reduces dropout or accidentally reinforces avoidance.
Patient-selection issue: PTSD is heterogeneous. Combat trauma, sexual assault, childhood maltreatment, medical trauma, and repeated community violence may not respond the same way to positive-valence learning. People with severe dissociation, moral injury, psychosis, mania risk, substance withdrawal, or ongoing threat may need different sequencing before any exposure-based augmentation is tested.
A useful clinical trial would also measure whether counterconditioning changes daily-life avoidance. Neural reinstatement is valuable only if it travels into behavior: fewer avoided places, better sleep after reminders, less physiological panic during cues, and improved functioning outside the scanner.
Dose and sequence: a therapy version would need to define when positive pairing is added. Adding it too early could become avoidance; adding it after initial exposure learning may strengthen safety without blunting emotional processing. That sequencing question is both clinical and neuroscientific.
Therapist training would matter too. Positive pairing has to be delivered as new learning, not as reassurance that prevents contact with feared material. The treatment manual would need rules for when to pause, when to intensify exposure, and when to stabilize first.
Those rules would decide whether the mechanism survives real therapy.
Questions About Counterconditioning and PTSD
Did this study test PTSD therapy?
No. It tested a laboratory fear-learning procedure during brain imaging.
Could counterconditioning improve exposure therapy for PTSD?
Positive pairing may strengthen safety learning beyond standard extinction. Therapy trials need to test whether that mechanism improves symptoms.
Why is vmPFC important here?
Ventromedial prefrontal cortex helps represent safety and value. Stronger vmPFC reinstatement suggests the counterconditioned cue kept a more durable safety memory.
References
- Augmenting extinction with counterconditioning strengthens and sustains neural safety representations in PTSD. Cooper SE, Helpman L, Dunsmoor JE, et al. Translational Psychiatry. 2026;16:305. doi:10.1038/s41398-026-03966-y
- Maximizing exposure therapy: an inhibitory learning approach. Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Behaviour Research and Therapy. 2014;58:10–23. doi:10.1016/j.brat.2014.04.006
- Fear extinction and relapse: state of the art. Vervliet B, Craske MG, Hermans D. Annual Review of Clinical Psychology. 2013;9:215–248. doi:10.1146/annurev-clinpsy-050212-185542
- The behavioral and neural processes in counterconditioning: past and future directions. Keller NE, Dunsmoor JE. Behaviour Research and Therapy. 2020;125:103532. doi:10.1016/j.brat.2019.103532